Bishops score and it's indications regarding delivery and induction
"Bishop score" AND "labor induction"
Bishop Score (Pelvic Scoring for Elective Induction of Labor)
The Scoring System
| Parameter | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Dilation | Closed | 1–2 cm | 3–4 cm | ≥5 cm |
| Effacement | 0–30% | 40–50% | 60–70% | ≥80% |
| Station | −3 | −2 | −1/0 | +1/+2 |
| Consistency | Firm | Moderate | Soft | — |
| Position | Posterior | Mid | Anterior | — |
Dilation is considered the single most predictive component; Lange et al. (808 patients) recommended scoring it at twice its assigned value. — Creasy & Resnik's Maternal-Fetal Medicine
Score Modifiers
- Preeclampsia
- Each prior vaginal delivery
- Postdates pregnancy
- Nulliparity
- Premature or prolonged rupture of membranes (PROM)
Interpretation & Clinical Thresholds
| Score | Cervical Status | Clinical Implication |
|---|---|---|
| ≥9 | Favorable/Ripe | Induction success approaches spontaneous labor; average labor ~4 hours in multiparas. No failed inductions in Bishop's original multipara series |
| >8 | Favorable | Likelihood of successful vaginal delivery with oxytocin approximates spontaneous labor |
| 6–8 | Intermediate | Induction may succeed; cervical ripening may be considered |
| <6 | Unfavorable | Correlates with prolonged labor or failed induction; cervical ripening strongly recommended before oxytocin |
| ≤5 | Unfavorable | 50% risk of failed induction in nulliparous women at term |
Indications for Induction of Labor (where Bishop Score guides management)
- Pregnancy-induced hypertension, preeclampsia, eclampsia (>80% of inductions)
- Prolonged/post-term pregnancy (>40–42 weeks)
- Maternal medical complications: diabetes mellitus, renal disease, chronic pulmonary disease, chronic hypertension
- Abruptio placentae
- Chorioamnionitis
- Abnormal antepartum testing requiring delivery
- Premature rupture of membranes (PROM)
- Fetal demise
- Isoimmunization
- Distance from hospital
- History of rapid labor/precipitous delivery
- Psychosocial factors
- To ensure presence of familiar physician/staff
Contraindications to Induction
Absolute
- Placenta previa or vasa previa
- Transverse fetal lie
- Prolapsed umbilical cord
- Previous classical (vertical) uterine incision
- Severe hydrocephalus
- Active genital herpes
- Invasive cervical carcinoma
- Non-reassuring fetal status
- Known hypersensitivity to prostaglandins
Relative
- Multiple gestation
- Polyhydramnios
- Appreciable macrosomia
- Maternal cardiac disease
- Previous uterine surgery (non-classical)
Management Based on Bishop Score
Bishop Score ≥8–9
→ Proceed directly with oxytocin or amniotomy
Bishop Score <6
→ Cervical ripening first:
Mechanical: Foley balloon catheter, laminaria
Pharmacologic: Dinoprostone (PGE₂), Misoprostol (PGE₁)
→ Then reassess → oxytocin if appropriate
- Amniotomy alone is effective when the cervix is favorable (Bishop ≥8); only 3.4% require additional oxytocin in such patients (Keettel series)
- If oxytocin is needed, a minimum of 12 hours of stimulation after membrane rupture should be required before diagnosing failed induction
- Elective induction carries a ~2× increased cesarean risk in nulliparas with an unfavorable cervix — this risk is nearly eliminated with a favorable cervix
Simplified Bishop Score
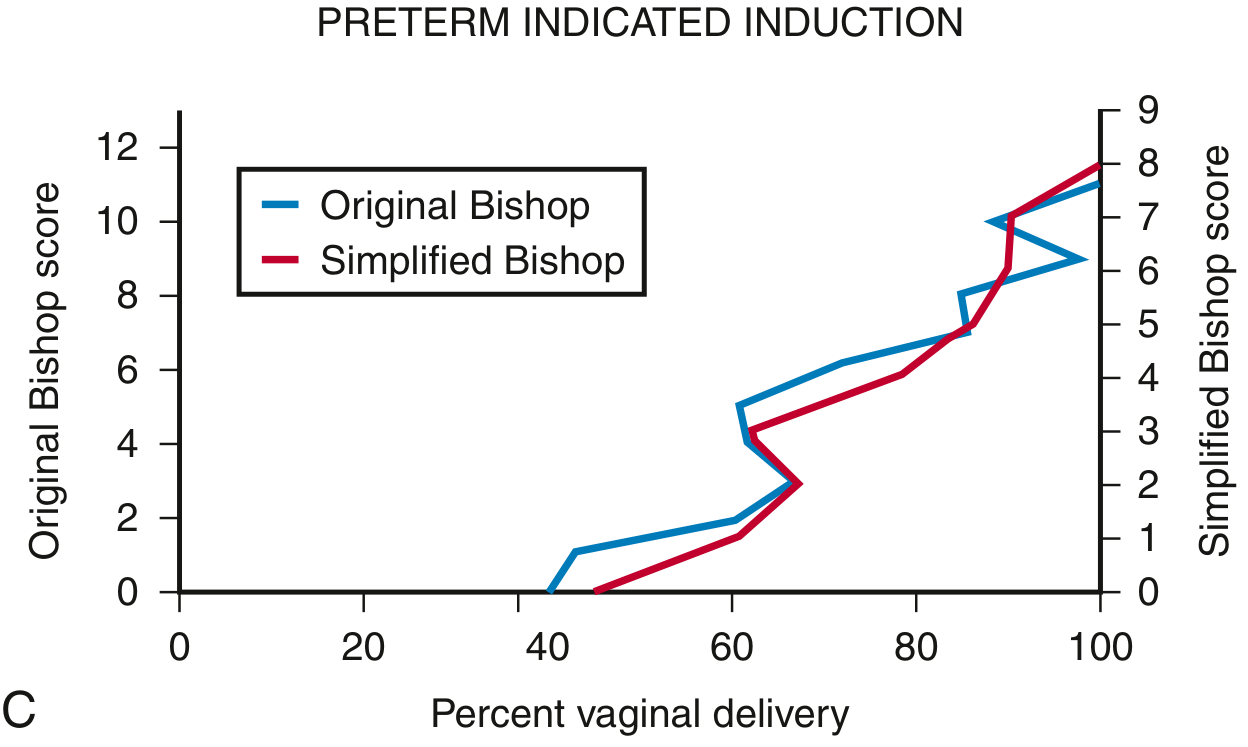
Bishop Score & Prediction of Preterm Birth
Recent Evidence
A 37 year old mother of 2 children presents with spontaneous onset vaginal delivery. Previous births are uncomplicated vaginal deliveries with babies weighing 3.5 kg and 3.6 kg respectively. Fetus is in extended breech position, Cervix is fully dilated, Station +1, Contractions are 4 per 10 minutes. What is the best management option
- 37-year-old, para 2 (multiparous)
- Previous uncomplicated vaginal deliveries, babies 3.5 kg and 3.6 kg → proven adequate pelvis
- Extended (frank) breech presentation
- Fully dilated cervix (second stage of labor)
- Station +1 (breech already engaged and descended)
- Contractions 4 per 10 min (adequate)
- Spontaneous onset labor
Best Management: Assisted Vaginal Breech Delivery
Why NOT Cesarean Section Here?
Why This Patient is a Good Candidate
| Factor | Patient's Finding | Score |
|---|---|---|
| Parity | >1 (para 2) | 1 |
| Gestational age | Term (~38–39 wk assumed) | 1 |
| Estimated fetal weight | Likely ~3.5 kg (based on prior babies) | 1 (3176–3629 g range) |
| Previous breech deliveries | None | 0 |
| Dilation | Fully dilated (≥4 cm) | 2 |
| Station | +1 or lower | 2 |
| Criterion | Status |
|---|---|
| Frank (extended) or complete breech | ✅ Frank/extended breech |
| Estimated fetal weight 2000–3800 g | ✅ ~3.5 kg (inferred from prior babies) |
| Normal gynecoid pelvis | ✅ Proven — 2 prior vaginal deliveries with large babies |
| Flexed fetal head | Needs confirmation (ideally ultrasound) |
| Skilled obstetrician available | Required |
Immediate Management Steps
1. Call for senior obstetrician + anesthetist + neonatologist immediately
2. Confirm fetal head position (ultrasound if possible)
3. Continuous fetal heart rate monitoring
4. IV access, consent, and prepare for emergency cesarean as backup
5. Consider episiotomy
Conduct of Delivery: Assisted Breech (Burns-Marshall / Lovset / Mauriceau-Smellie-Veit)
- Allow spontaneous descent with maternal effort
- Perform Pinard's maneuver to deliver flexed legs (flex knees, sweep out legs one at a time)
- Once umbilicus delivers → pull out 10–15 cm loop of cord to prevent traction/compression
- Grasp the baby by the bony pelvis (iliac crests), never the abdomen (risk of visceral injury)
- Rotate trunk to bring posterior shoulder to anterior position → deliver arms by sweeping them across the face
- If nuchal arm occurs: rotate in direction of arm to dislodge
- Place baby astride the forearm; insert index and middle fingers of that hand into mouth to maintain flexion
- Two fingers of other hand on the occiput
- Apply gentle downward traction to deliver the head under the symphysis, then lift upward
- Burns-Marshall technique is an alternative: allow the baby to hang by gravity for 1–2 minutes (promotes head flexion), then sweep upward in an arc
What to AVOID
- Traction on the fetus during delivery (before the head)
- Grasping the waist → abdominal organ injury
- Fundal pressure during delivery of head
- Oxytocin augmentation in breech labor — use with extraordinary caution (Hannah trial: 64% of perinatal deaths in vaginal arm occurred in induced/augmented labors)
- Inappropriate transfer during imminent delivery
Summary Answer
The best management is assisted vaginal breech delivery by a skilled obstetrician, with the neonatologist and anesthesia team present. This multiparous patient with a proven adequate pelvis (two prior vaginal deliveries of 3.5–3.6 kg babies), frank breech, full dilatation, and advanced station (+1) is an ideal candidate. The Zatuchni-Andros prognostic score is highly favorable. Cesarean section at this stage is not the best option given advanced labor and high probability of successful vaginal delivery, though it must remain available as a fallback.
Situations where vacuum is contraindicated and forceps is not and vice versa
Vacuum vs Forceps: Differential Contraindications
Situations Where VACUUM is Contraindicated but FORCEPS is NOT
| Situation | Reason vacuum fails/harms | Forceps role |
|---|---|---|
| Face presentation (mentum anterior) | Cup cannot achieve flexion point on a deflexed head; scalp traction worsens deflexion | Forceps can be applied to a face (Kielland's or Wrigley's) |
| Breech — aftercoming head | No scalp to apply cup to; mechanism requires controlled flexion of the head | Piper forceps specifically designed for aftercoming head |
| Preterm infant (<34 weeks' gestation) | Immature skull/fragile vessels → greatly increased risk of subgaleal and intracranial hemorrhage | Forceps distributes force over larger surface area; preferred if operative delivery needed |
| Fetal coagulation defect / suspected bleeding disorder (e.g., alloimmune thrombocytopenia, haemophilia) | Vacuum creates a scalp chignon → compresses vessels → subgaleal/intracranial haematoma in coagulopathic infant | Forceps avoids suction-induced scalp vascular stress |
| Prior fetal scalp blood sampling | Sampling wound + vacuum suction = high-risk scalp haematoma and haemorrhage | Forceps acceptable |
| Fetal scalp electrode (FSE) in situ | Cup cannot achieve seal over an electrode; electrode site bleeds under suction | Forceps delivery unaffected by electrode placement |
| Head position not precisely determined | Correct cup placement (over flexion point) requires knowing exact position; misapplication → asynclitism, failure, injury | Experienced operator can apply forceps by palpating sutures/fontanelles for exact placement |
| Need for very rapid delivery (acute cord prolapse, severe prolonged bradycardia) | Vacuum requires contractions; slower to achieve delivery | Forceps allows immediate traction regardless of contractions |
Situations Where FORCEPS is Contraindicated but VACUUM is NOT (or Vacuum Preferred)
| Situation | Reason forceps is contraindicated/unfavourable | Vacuum role |
|---|---|---|
| Occipitoposterior (OP) or occipitotransverse (OT) position — when rotation is needed but operator lacks rotational forceps skill | Rotational forceps (Kielland's) require advanced expertise; risk of severe perineal/vaginal trauma if inexperienced | Vacuum allows autorotation — the head rotates naturally as it descends; no rotational skill required |
| Operator inexperienced with forceps | Forceps requires significant training; misapplication causes severe maternal and fetal injury | Vacuum is easier to learn and apply; lower skill threshold for safe use |
| Maternal desire to minimise perineal trauma | Forceps → significantly more cervical, vaginal, and perineal lacerations (including 3rd/4th degree tears) | Vacuum causes fewer maternal soft tissue injuries |
| Inadequate analgesia / no regional block available | Forceps application requires adequate analgesia (typically regional or pudendal); painful without | Vacuum requires less anesthesia; can be used with minimal or no regional block |
Absolute Contraindications to BOTH Instruments
- Unengaged fetal head (station above 0)
- Incomplete cervical dilatation (except urgent delivery of a second twin or severe FHR abnormality without immediately available cesarean)
- Brow presentation
- Cephalopelvic disproportion (CPD)
- Transverse lie
- Delivery requiring excessive traction
- Position of fetal head unknown (also specific to forceps)
Summary Table
| Clinical Scenario | Vacuum | Forceps |
|---|---|---|
| Face presentation | ❌ Contraindicated | ✅ Use forceps |
| Breech aftercoming head | ❌ Contraindicated | ✅ Piper forceps |
| Preterm <34 weeks | ❌ Contraindicated | ✅ Preferred |
| Fetal coagulopathy | ❌ Contraindicated | ✅ Preferred |
| Prior scalp sampling / FSE | ❌ Contraindicated | ✅ Acceptable |
| Head position uncertain | ❌ Contraindicated | ✅ Use forceps (with careful assessment) |
| Acute fetal distress, rapid delivery needed | ⚠️ Slower (contraction-dependent) | ✅ Preferred for speed |
| OP/OT position needing rotation | ✅ Autorotation occurs | ⚠️ Only if skilled (Kielland's) |
| Inexperienced operator | ✅ Easier, safer | ❌ Higher injury risk |
| Minimal analgesia available | ✅ Less anesthesia needed | ❌ Requires adequate block |
| Minimising maternal soft tissue trauma | ✅ Fewer lacerations | ❌ More perineal/vaginal tears |
Critical Warning: Sequential Use
Never follow a failed vacuum with forceps. Towner et al. showed that combined vacuum + forceps use resulted in intracranial haemorrhage rates 7.4× greater than spontaneous delivery and 3.4× greater than vacuum alone. ACOG guidelines explicitly recommend against sequential instrument use. If vacuum fails → proceed to cesarean section.
A 35-year-old primi with an uncomplicated antenatal history presents with spontaneous onset of labor at 39 weeks of gestation. The station is static at +2 with adequate maternal pushing and uterine contractions for 2 hours in theactive stage of the second stage of labor. The fetus is in direct occipito anterior position with mild caput and moulding +1. What is the most appropriate management?