Here is the complete, detailed explanation for all slides based on the case of J.C., 25-year-old male, post-Open Appendectomy, with final histopath confirming Appendiceal Neuroendocrine Tumor (Carcinoid). All content is referenced to Schwartz's Principles of Surgery.
MODULE 6: SMALL INTESTINE AND APPENDIX — CASE 5
Complete Slide-by-Slide Explanation
SLIDE 1: TITLE SLIDE
Title: Appendiceal Neuroendocrine Tumor (Carcinoid): A Surgical Case Discussion
Case: J.C., 25-year-old male, post-Open Appendectomy for Acute Appendicitis — incidental carcinoid on final histopath
Reference: Schwartz's Principles of Surgery, 11th Edition
SLIDE 2: OBJECTIVES
By the end of this case presentation, the learner should be able to:
- Identify the clinical presentation of acute appendicitis and its mimickers
- Recognize the histopathologic features of appendiceal neuroendocrine tumors (NETs/carcinoids)
- Interpret gross and microscopic pathological findings of incidentally discovered appendiceal carcinoid
- Discuss the differential diagnosis for right lower quadrant pain
- Formulate a complete diagnostic and management plan for appendiceal NET based on tumor size and staging
- Understand the indications for appendectomy alone vs. right hemicolectomy in appendiceal NETs
- Outline adjuvant therapy, surveillance, and follow-up for appendiceal neuroendocrine tumors
SLIDE 3: HISTORY OF PRESENT ILLNESS (HPI)
Patient: J.C., 25-year-old male
Chief Complaint: Follow-up consult, 1 week post-operatively
History:
- Patient was admitted 1 week prior with complaints of:
- Fever (exact temperature not recorded at first admission)
- Right Lower Quadrant (RLQ) pain
- Clinical diagnosis of Acute Appendicitis was made
- Patient underwent Open Appendectomy
- On follow-up visit today:
- Wound is well-coaptated
- No complaints of post-operative pain
- Patient is afebrile, vitally stable
- Patient brought the final histopathology result which revealed an incidental finding
Key Surgical Note: The primary reason for surgery was acute appendicitis. The carcinoid/NET was an incidental finding on final histopath — a classic scenario in clinical surgery, occurring in approximately 0.3–0.9% of appendectomy specimens.
SLIDE 4: PAST MEDICAL HISTORY (PMH)
| # | History | Details |
|---|
| 1 | S/P ORIF Plating, Left Humerus | 2005 — previous orthopedic surgery, not relevant to current case |
| 2 | Open Appendectomy | 1 week prior — current surgery for acute appendicitis |
Surgical Relevance:
- No prior abdominal surgery besides current appendectomy — this is important because adhesion formation is relevant in any subsequent surgery (e.g., right hemicolectomy if indicated)
- No history of cancer, GI disease, or hereditary syndromes noted
- No known drug allergies documented
SLIDE 5: PERSONAL AND SOCIAL HISTORY / FAMILY HISTORY
Personal and Social History:
| Finding | Clinical Significance |
|---|
| Alcohol | Occasional alcoholic beverage drinker | Minimal risk factor; relevant for hepatic metabolism, anesthesia risk |
| Tobacco | Smoker, 1 pack-year | Low cumulative exposure; mild cardiovascular/pulmonary risk |
Family History: Not documented in the case — should be asked about:
- Any family history of Multiple Endocrine Neoplasia type 1 (MEN-1) — associated with pancreatic and other NETs
- History of GI cancers or hereditary cancer syndromes (Lynch, FAP)
- These should be elicited during the follow-up visit as the carcinoid diagnosis is now confirmed
Social Relevance: Young, 25-year-old male — excellent functional baseline; good surgical candidate for any further procedure if indicated
SLIDE 6: PHYSICAL EXAMINATION
Vital Signs:
| Parameter | Value | Interpretation |
|---|
| BP | 120/80 mmHg | Normal |
| HR | 80 bpm | Normal |
| RR | 20 cpm | Normal |
| Temp | 36.7°C | Afebrile |
| O2 Sat | 98% at room air | Normal |
| Height | 5'6" | — |
| Weight | 50 kg | BMI ~17.7 — mildly underweight |
Physical Exam Findings:
- HEENT: Anicteric sclerae (no jaundice), trachea at midline, no palpable lymphadenopathy
- C/L: Clear breath sounds, equal chest expansion, equal tactile fremitus — no pulmonary compromise
- CV: Adynamic precordium, regular rate and rhythm — notably, no murmur (carcinoid heart disease — tricuspid regurgitation — is absent, appropriate for localized disease)
- Abdomen: (+) Post-op wound at RLQ, well-coaptated, no erythema — healing well, no wound infection signs
- Extremities: Strong peripheral pulses, CRT <2 seconds, Full ROM — no edema, no stigmata of carcinoid syndrome (no flushing, no telangiectasia)
- GUT: (-)KPS — no costovertebral angle tenderness
Overall Impression from PE: Patient appears to be recovering well post-appendectomy with no signs of surgical site infection or systemic disease. No clinical features of carcinoid syndrome (absent because disease is localized — serotonin gets metabolized by the liver before reaching systemic circulation).
SLIDE 7: PRIMARY IMPRESSION / DIAGNOSIS
Pre-histopath Primary Impression:
Acute Appendicitis, NOS — Post-Operative Day 7, Status Post Open Appendectomy
Basis:
- Classical presentation: fever + RLQ pain
- McBurney's point tenderness (presumed at initial admission)
- Leukocytosis (expected at initial admission)
- Confirmed surgically — inflamed appendix with surrounding fat stranding on gross specimen
Post-histopath Primary Impression:
Well-Differentiated Appendiceal Neuroendocrine Tumor (NET G1), Carcinoid, Incidentally Discovered
- Tumor at base of appendix, 1.8–2.8 cm
- Chromogranin A (+), Synaptophysin (+)
- Salt-and-pepper chromatin, nested architecture
SLIDE 8–9: DIFFERENTIAL DIAGNOSIS
The initial presentation of fever + RLQ pain has a broad differential. Here are at least 3:
DDx 1: Acute Appendicitis ✅ (Confirmed initially)
- Clinical features: Fever, anorexia, periumbilical pain migrating to RLQ, rebound tenderness at McBurney's point, Rovsing's sign, psoas sign
- Labs: Leukocytosis with left shift
- Imaging: CT abdomen/pelvis — dilated appendix >6mm, periappendiceal fat stranding, appendicolith
- Most common diagnosis — confirmed in this patient, prompting the open appendectomy
DDx 2: Appendiceal Mucinous Neoplasm (LAMN/HAMN)
- Why consider: RLQ pain, appendiceal mass, bulbar lesion at base
- Difference: Gross appearance is mucin-filled, distended appendix ("mucocele"); microscopy shows mucin-secreting columnar epithelium, NOT neuroendocrine nests
- Danger: Rupture can cause pseudomyxoma peritonei
- Against this case: Histopath showed neuroendocrine cells with chromogranin/synaptophysin positivity, not mucinous cells
DDx 3: Appendiceal Adenocarcinoma
- Why consider: Mass at base of appendix, firm lesion
- Difference: Shows gland-forming structures, mucin production, marked pleomorphism, aggressive invasion
- Against this case: Cells are small and uniform with salt-and-pepper chromatin; IHC shows neuroendocrine markers, not CK20/CDX2-dominant adenocarcinoma profile
DDx 4: Goblet Cell Carcinoid (GCC) / Adenocarcinoid
- Why consider: Hybrid neoplasm, occurs at appendix, can present similarly
- Difference: Shows both glandular (goblet cell) and neuroendocrine differentiation; more aggressive behavior; mixed IHC pattern
- Against this case: Pure neuroendocrine morphology with no mucinous/goblet cell component described; diffuse Chromogranin A and Synaptophysin without CDX2
DDx 5: Mesenteric Lymphadenitis / Crohn's Disease (RLQ mimic)
- Why consider: RLQ pain, fever in young patients
- Difference: No discrete appendiceal mass; ileal wall thickening and skip lesions on imaging/pathology for Crohn's
- Against this case: Appendix was surgically confirmed as the source; no ileitis described
SLIDE 10: INTERPRETATION OF RESULTS
Gross Pathology:
| Finding | Significance |
|---|
| Appendix: 90mm long, 7mm diameter | Inflamed — normal diameter is 3–6mm |
| Surrounding fat stranding | Confirms acute periappendiceal inflammation |
| 1.8 cm firm, yellow, bulbar mass at base | Classic gross appearance of carcinoid — firm, yellow-tan, solid |
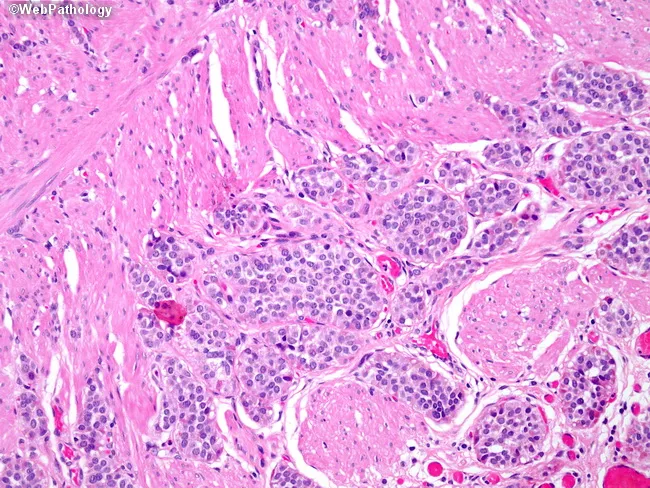
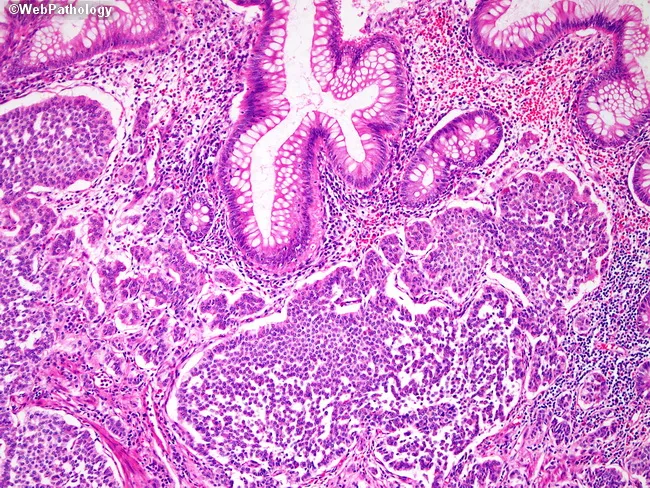
Microscopic Pathology:
| Finding | Significance |
|---|
| 2.8 cm lesion at base, submucosal, nodular | Concerning size — >2 cm = high-risk for metastasis (Schwartz's: 30% metastatic rate at >2 cm) |
| Nested/organoid pattern | Classic architecture of well-differentiated NET |
| Small, uniform cells | Low-grade morphology |
| Round nuclei, central prominent nucleoli | Neuroendocrine cytology |
| Salt-and-pepper chromatin | Pathognomonic for neuroendocrine differentiation |
| Chromogranin A (+) — diffuse | Confirms neuroendocrine secretory granules |
| Synaptophysin (+) — diffuse | Confirms neuroendocrine differentiation (synaptic vesicle marker) |
Histopathology Images from the Case:
Left image (H&E): Shows the classic nested pattern of small uniform cells — "insular" growth pattern typical of midgut-type carcinoid
Right image (IHC — Chromogranin A): Diffuse brown cytoplasmic positivity — confirms neuroendocrine lineage
Classification per WHO 2022 / ENETS:
- NET G1 (if Ki-67 <3%, mitoses <2/10 HPF) — most likely given low-grade morphology
- NET G2 if Ki-67 3–20%
SLIDE 11: FINAL IMPRESSION / DIAGNOSIS
Final Diagnosis:
Appendiceal Well-Differentiated Neuroendocrine Tumor (NET), Grade 1
Incidentally discovered in a background of Acute Appendicitis, Status Post Open Appendectomy
Key diagnostic criteria met:
- ✅ Submucosal, nested/organoid architecture
- ✅ Small, uniform cells with salt-and-pepper chromatin
- ✅ Diffuse Chromogranin A positivity
- ✅ Diffuse Synaptophysin positivity
- ✅ Gross: firm, yellow, bulbar mass at appendix base
- ✅ Size: 2.8 cm (clinically significant — exceeds 2 cm threshold)
Critical Size Implication (per Schwartz's):
- Tumors <1 cm: >95% cure rate with appendectomy alone
- Tumors 1–2 cm: consider clinical factors; may need hemicolectomy
- Tumors >2 cm: appendectomy alone is NOT sufficient — right hemicolectomy is indicated due to ~30% risk of lymph node metastasis
This patient's 2.8 cm tumor → Right Hemicolectomy is indicated
CASE DISCUSSION
SLIDES 12–13: BRIEF ANATOMY AND PHYSIOLOGY
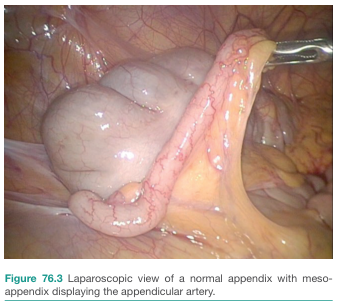
Anatomy of the Appendix
The vermiform appendix is a blind-ended tubular structure arising from the posteromedial wall of the cecum, approximately 2–3 cm below the ileocecal valve. It is a midgut-derived structure.
Key anatomical facts:
| Feature | Detail |
|---|
| Length | 2–20 cm, average 9 cm |
| Diameter | 3–8 mm (normal) |
| Position | Variable — retrocecal (most common, 65%), pelvic, subcecal, pre-ileal, post-ileal |
| Blood supply | Appendicular artery (branch of ileocolic artery → from superior mesenteric artery); runs in mesoappendix |
| Venous drainage | Appendicular vein → ileocolic vein → superior mesenteric vein → portal vein |
| Lymphatics | Drain to ileocolic lymph nodes along superior mesenteric artery |
| Innervation | Sympathetic (T10), parasympathetic (vagus nerve) |
Layers of the Appendiceal Wall (inside out):
- Mucosa — columnar epithelium, goblet cells, crypts of Lieberkühn
- Submucosa — rich in lymphoid tissue (250+ lymphoid follicles), site of carcinoid origin
- Muscularis propria — inner circular, outer longitudinal
- Serosa — visceral peritoneum
Neuroendocrine Cells (Enterochromaffin/Kulchitsky Cells):
- Located in the crypts of the mucosa/submucosa
- Part of the diffuse neuroendocrine system (DNES) / APUD system
- Produce serotonin (5-HT), substance P, motilin, and other peptides
- These are the cells of origin of carcinoid tumors
Physiology:
- Appendix has immune function — high density of lymphoid tissue; acts as a "safe house" for gut microbiome
- Neuroendocrine cells regulate gut motility, secretion, and vascular tone via paracrine/endocrine signaling
- Serotonin produced by enterochromaffin cells → vasoactive; in excess (metastatic NET) causes carcinoid syndrome
SLIDES 14–15: DEFINITION, PATHOPHYSIOLOGY, ETIOLOGY & RISK FACTORS
Definition
A Neuroendocrine Tumor (NET), previously called "carcinoid tumor," is a neoplasm arising from the enterochromaffin (Kulchitsky) cells of the neuroendocrine system. In the appendix, these are the most common primary tumor (accounts for 50–77% of appendiceal tumors).
Per WHO 2022 classification:
- NET G1: Ki-67 <3%, mitoses <2/10 HPF
- NET G2: Ki-67 3–20%, mitoses 2–20/10 HPF
- NET G3: Ki-67 >20% (well-differentiated but high proliferation)
- NEC (Neuroendocrine Carcinoma): High grade, poorly differentiated
Pathophysiology
Step 1 — Origin:
Kulchitsky/enterochromaffin cells in appendiceal crypts undergo neoplastic transformation → form clusters → expand into submucosa
Step 2 — Growth Pattern:
- Slow-growing (doubling time: months to years)
- Organoid/insular architecture — nests surrounded by fibrovascular stroma
- Invades submucosa → muscularis propria → mesoappendix → regional nodes
Step 3 — Secretory Function:
- Produce serotonin (5-HT), substance P, histamine, bradykinin
- In localized disease: metabolized by liver → no systemic syndrome
- In metastatic disease (especially liver mets): serotonin bypasses hepatic metabolism → Carcinoid Syndrome:
- Episodic flushing
- Secretory diarrhea
- Bronchospasm
- Right-sided cardiac valvular disease (carcinoid heart disease)
Step 4 — Malignant Potential by Size (Schwartz's):
| Tumor Size | Metastasis Rate |
|---|
| <1 cm | <2% |
| 1–2 cm | ~10% |
| >2 cm | ~30% |
Etiology
- Sporadic — majority of cases; no identified genetic cause
- MEN-1 (Multiple Endocrine Neoplasia Type 1) — rare association
- NF-1 (Neurofibromatosis Type 1)
- No direct causation from alcohol or tobacco
Risk Factors
| Factor | Detail |
|---|
| Age | Peak: 40s–50s (but can occur at any age, including 25 as in this case) |
| Sex | Slight female predominance for appendiceal carcinoid |
| Race | Higher incidence in Black Americans |
| MEN-1 | Germline MEN1 mutation — associated with multiple NETs |
| Prior appendicitis | May theoretically promote microenvironmental changes |
| Chronic atrophic gastritis | Risk factor for gastric NETs specifically |
SLIDE 16: DIAGNOSTICS (IDEAL LABORATORY AND IMAGING STUDIES)
Laboratory Studies
| Test | Rationale |
|---|
| CBC with differential | Leukocytosis in acute appendicitis; baseline pre-operative |
| Serum Chromogranin A (CgA) | Primary biomarker for NETs; elevated in >80% of NETs; correlates with tumor burden |
| 24-hour urinary 5-HIAA (5-hydroxyindoleacetic acid) | Metabolite of serotonin; elevated in functional/metastatic carcinoid; sensitivity ~70% |
| Serum serotonin | Direct measure; useful if 5-HIAA unavailable |
| Serum pancreastatin | More specific NET marker, less affected by diet than CgA |
| LFTs, AFP | Evaluate for liver metastases |
| BMP/CMP | Metabolic baseline |
| Coagulation studies | Pre-operative if hemicolectomy planned |
Imaging Studies
| Modality | Use |
|---|
| CT Abdomen/Pelvis with contrast (3-phase) | Evaluate for mesenteric/lymph node involvement, liver mets; NET mets are hypervascular — best seen on arterial phase |
| MRI Abdomen | Superior to CT for detecting small liver metastases; no radiation |
| Ga-68 DOTATATE PET/CT (Somatostatin Receptor PET) | Gold standard functional imaging; detects somatostatin receptor-positive NETs; superior to OctreoScan |
| Octreotide Scan (In-111 OctreoScan) | Older alternative to Ga-68 DOTATATE; detects SSTR2-positive tumors; identifies distant mets |
| Echocardiography | If elevated 5-HIAA: screen for carcinoid heart disease (tricuspid regurgitation, pulmonary stenosis) |
| Endoscopy (colonoscopy) | Evaluate cecum and appendiceal orifice; assess base margins |
SLIDES 17–23: MANAGEMENT
Pre-operative Management (for the upcoming Right Hemicolectomy)
Indication: Tumor size 2.8 cm — exceeds the >2 cm threshold per Schwartz's Principles of Surgery → Right Hemicolectomy is the standard of care
Pre-op workup:
- Complete staging: CT abdomen/pelvis + chest (3-phase); Ga-68 DOTATATE PET/CT
- Biomarkers: Serum CgA, 24-hr urine 5-HIAA → establish baseline
- Echocardiography: Rule out carcinoid heart disease before surgery
- Optimization: Correct anemia/malnutrition — this patient is mildly underweight (50 kg, 5'6"), consider nutritional support
- Bowel preparation: Mechanical bowel prep + oral antibiotics (per institutional protocol) — essential before hemicolectomy
- DVT prophylaxis: LMWH + TED stockings initiated pre-operatively
- Informed consent: Discuss right hemicolectomy, anastomosis, risks, ostomy possibility
- Anesthesia clearance: Standard pre-anesthetic evaluation; note prior ORIF surgery (musculoskeletal history)
Note on Octreotide: Pre-operative octreotide infusion is indicated if the patient has carcinoid syndrome (flushing, diarrhea) to prevent carcinoid crisis during anesthesia/surgery. In this patient (no syndrome, localized disease), it may not be mandatory but should be available intraoperatively.
Neoadjuvant Treatment
Not applicable in standard localized appendiceal NET G1. These tumors are resection-first — there is no role for neoadjuvant chemotherapy or radiation in well-differentiated, localized appendiceal NETs. Neoadjuvant approaches are reserved for unresectable or borderline-resectable high-grade NECs.
Surgical Treatment: Right Hemicolectomy
Indication in this case: Appendiceal NET ≥2 cm with potential mesoappendiceal invasion
Goal: Achieve R0 resection with adequate lymph node sampling (minimum 12 nodes)
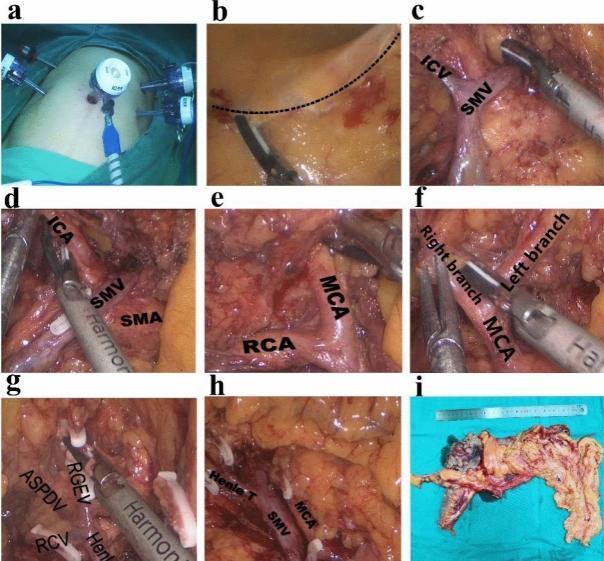
Procedure Description:
Step 1 — Positioning and Access:
- Patient supine, general endotracheal anesthesia
- Open (midline laparotomy) or laparoscopic approach (preferred if expertise available)
- Explore peritoneal cavity — assess for liver metastases, peritoneal implants, lymphadenopathy
Step 2 — Mobilization of the Right Colon:
- Incise the lateral peritoneal attachments (white line of Toldt) from terminal ileum to hepatic flexure
- Medial-to-lateral dissection preferred laparoscopically
- Dissect in the avascular retroperitoneal plane (anterior to Gerota's fascia)
- Protect ureter, gonadal vessels, duodenum
Step 3 — Vascular Ligation (D3 Lymphadenectomy):
- Ligate the ileocolic artery and vein at their origins from the superior mesenteric vessels → ensures oncologic nodal clearance
- Divide right colic artery if present
- Right branch of middle colic artery may be divided depending on hepatic flexure involvement
Step 4 — Bowel Division:
- Divide terminal ileum ~10–15 cm proximal to ileocecal valve using linear cutting stapler
- Divide transverse colon at the mid-transverse level
- Remove specimen including: terminal ileum, cecum, ascending colon, hepatic flexure, mesentery with lymph nodes
Step 5 — Anastomosis:
- Ileocolic anastomosis (side-to-side or end-to-end):
- Stapled (preferred) or hand-sewn
- Tension-free, adequate blood supply confirmed
- Side-to-side functional end-to-end anastomosis is most common
Step 6 — Closure:
- Inspect anastomosis and hemostasis
- Close mesenteric defect to prevent internal herniation
- Layer-by-layer fascial closure; skin closure
Post-operative Complications and Management
| Complication | Incidence | Management |
|---|
| Anastomotic leak | 1–5% | NPO, IV antibiotics, CT-guided drainage vs. re-exploration |
| Surgical site infection (SSI) | 5–15% | Wound opening, antibiotics, wound care |
| Ileus | Common (3–5 days) | NPO/clear liquids, ambulation, chewing gum (enhanced recovery) |
| Intra-abdominal abscess | 2–5% | CT-guided drainage, antibiotics |
| Bleeding | <2% | Transfusion, re-exploration if hemodynamically unstable |
| DVT/PE | 1–3% | LMWH prophylaxis continued; therapeutic anticoagulation if confirmed |
| Urinary retention | Common | Foley catheter, alpha-blockers |
| Carcinoid crisis | Rare intraoperatively | IV octreotide bolus (300–500 mcg) + infusion |
Enhanced Recovery After Surgery (ERAS) Protocol:
- Early oral intake (clear liquids POD0–1)
- Early mobilization
- Multimodal pain management (minimize opioids)
- Remove urinary catheter POD1–2
- Target discharge: POD 3–5
Adjuvant Therapy and Surveillance
Adjuvant Chemotherapy / Radiation:
- Not indicated for completely resected (R0) NET G1/G2
- Reserved for: incomplete resection (R1/R2), high-grade NEC, or metastatic disease
Somatostatin Analogs (SSA) — Octreotide LAR / Lanreotide:
- Indication in resected disease: If evidence of residual disease, high Ki-67, or metastatic component
- Antiproliferative effect: PROMID trial (octreotide LAR) and CLARINET trial (lanreotide) showed significant improvement in progression-free survival in metastatic midgut NETs
- Dose: Octreotide LAR 20–30 mg IM every 4 weeks; Lanreotide 120 mg deep SC every 4 weeks
PRRT (Peptide Receptor Radionuclide Therapy — Lu-177 DOTATATE):
- Indicated for metastatic, somatostatin receptor-positive NETs
- NETTER-1 trial: significant PFS benefit vs. high-dose octreotide in midgut NET
- Not indicated for this patient if R0 resection achieved
Surveillance Protocol (post-curative resection of appendiceal NET >2 cm):
| Timepoint | Action |
|---|
| Every 3–6 months × 3 years | Serum CgA, 24-hr urine 5-HIAA |
| 6 months post-op | CT abdomen/pelvis (3-phase) |
| Annually × 5 years | CT abdomen/pelvis |
| Annually | Clinical exam, biomarkers |
| If symptoms arise (flushing, diarrhea) | Echocardiography, Ga-68 DOTATATE PET/CT |
| After 5 years (if disease-free) | Reduce surveillance frequency |
SLIDES 24–25: CASE RESOLUTION
Complete Management Plan for J.C.
Current status: POD 7 post Open Appendectomy, wound well-healing, asymptomatic
STEP 1 — IMMEDIATE (This follow-up visit):
- Review histopath: 2.8 cm appendiceal NET, Chromogranin A (+), Synaptophysin (+)
- Counsel patient on diagnosis: incidental carcinoid, implications of size >2 cm
- Recommend completion Right Hemicolectomy — explain rationale (lymph node risk ~30% at this size)
- Wound care instructions — suture removal at 10–14 days
STEP 2 — STAGING WORKUP (Next 1–2 weeks):
- CT abdomen/pelvis/chest with triple phase contrast — assess lymph nodes, liver, peritoneum, lung
- Serum Chromogranin A (baseline)
- 24-hour urine 5-HIAA (baseline functional marker)
- Ga-68 DOTATATE PET/CT — somatostatin receptor imaging for staging
- Echocardiography — screen for carcinoid heart disease
- Oncology referral — multidisciplinary tumor board discussion
STEP 3 — SURGERY (Once staging complete, ~2–4 weeks post-appendectomy, once patient fully recovered):
- Right Hemicolectomy (open or laparoscopic)
- Adequate lymphadenectomy (≥12 nodes)
- Intraoperative octreotide available
- ERAS protocol
STEP 4 — POST-OP MANAGEMENT:
- ERAS protocol: early ambulation, multimodal analgesia, early feeding
- DVT prophylaxis
- Target discharge POD 3–5
- Wound and drain management
STEP 5 — PATHOLOGY OF HEMICOLECTOMY SPECIMEN:
- Assess: lymph node involvement (number positive/total), resection margins (R0 vs R1), vascular/perineural invasion, Ki-67 index
- Final staging (TNM per AJCC/ENETS):
- T3 (>2 cm or mesoappendix invasion) N0/N1 M0
STEP 6 — ADJUVANT THERAPY:
- If R0, N0: Surveillance only — no adjuvant chemotherapy
- If N1 (nodal mets) or R1: Somatostatin analog (Octreotide LAR or Lanreotide)
- If distant mets discovered: multidisciplinary management — SSA, PRRT (Lu-177 DOTATATE), cytoreductive surgery
STEP 7 — LONG-TERM SURVEILLANCE:
- Serum CgA + 24-hr urine 5-HIAA every 3–6 months × 3 years, then annually
- CT abdomen/pelvis every 6–12 months × 5 years
- Annual clinical review for carcinoid syndrome symptoms (flushing, diarrhea, wheezing)
- Echocardiography if symptoms or rising 5-HIAA
PROGNOSIS:
| Scenario | 5-Year Survival |
|---|
| Localized, R0 resection (<2 cm) | >95% |
| Localized, R0 resection (this patient, 2.8 cm with hemicolectomy) | ~85–90% |
| Regional nodal disease | ~65–70% |
| Distant metastases | ~35–50% |
Summary Table
| Aspect | Finding / Decision |
|---|
| Patient | 25M, post-appendectomy |
| Histopath | Well-differentiated NET G1, 2.8 cm base of appendix |
| IHC | Chromogranin A (+), Synaptophysin (+) |
| Critical finding | Size >2 cm → lymph node risk ~30% |
| Next surgery | Right Hemicolectomy |
| Staging | CT 3-phase + Ga-68 DOTATATE PET/CT |
| Biomarkers | CgA + 24-hr urine 5-HIAA |
| Adjuvant (if R0 N0) | Surveillance only |
| Adjuvant (if N1/R1) | Octreotide LAR or Lanreotide |
| Surveillance | q3–6 months × 3yr, then annually |
Reference: Schwartz's Principles of Surgery, 11th Edition — Chapter on Small Intestine and Appendix; ENETS Consensus Guidelines 2023; NANETS Guidelines; WHO Classification of Tumors 2022 (Digestive System)