Cystoscpy + turp
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a thorough, textbook-based overview of Cystoscopy and TURP.
Cystoscopy
Definition
Direct endoscopic visualisation of the urethra and bladder using a cystoscope. The entire lower urinary tract from the urethral meatus to the bladder can be inspected, and with progressively longer instruments (ureteroscope) the ureters and renal pelvis can also be visualised. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Types
| Type | Anaesthesia | Primary role |
|---|---|---|
| Flexible cystoscopy | Local (lidocaine gel) | Diagnostic; poorly tolerated in young males due to angulated male urethra |
| Rigid cystoscopy | General or spinal | Diagnostic + operative; preferred for surgical procedures |
Available telescope angles: 0°, 12°, 30°, and 70° lenses.
Indications
-
Haematuria (macroscopic or microscopic, not explained by UTI)
-
Bladder tumour - diagnosis, staging (TURBT), surveillance
-
Recurrent UTIs
-
Overactive bladder (OAB) refractory to treatment
-
Suspected vesicovaginal fistula
-
Lower urinary tract symptoms (LUTS) due to BPH / bladder outlet obstruction
-
Foreign body, bladder stone
-
Urethral stricture assessment
-
Pre-TURP - mandatory cystourethroscopy before resection to exclude concomitant bladder tumour, stone, or stricture
-
Intraoperative check after pelvic/incontinence surgery (injury exclusion)
-
Berek & Novak's Gynecology; Bailey and Love's
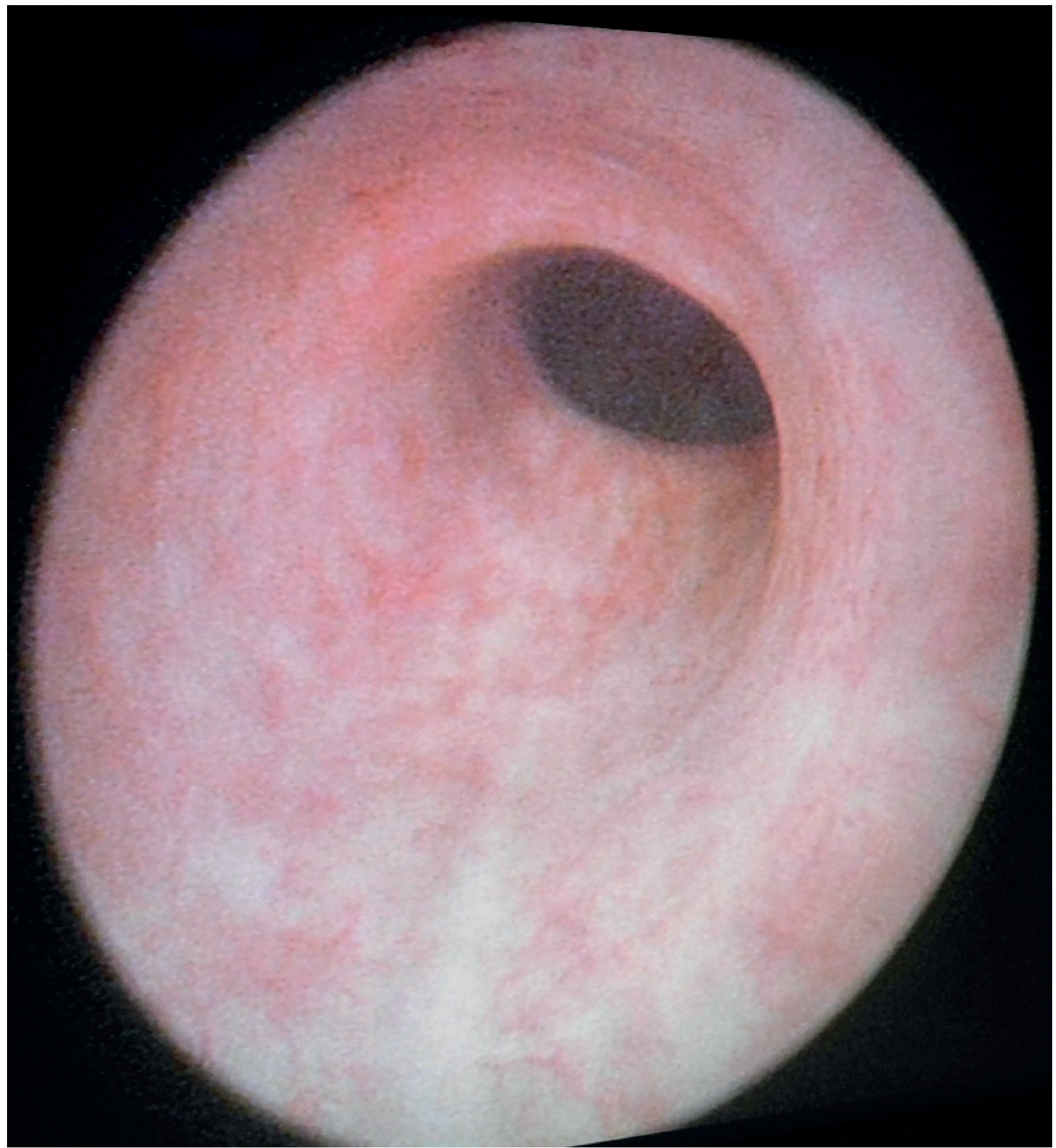
Cystoscopic images
Normal urethra on urethroscopy:
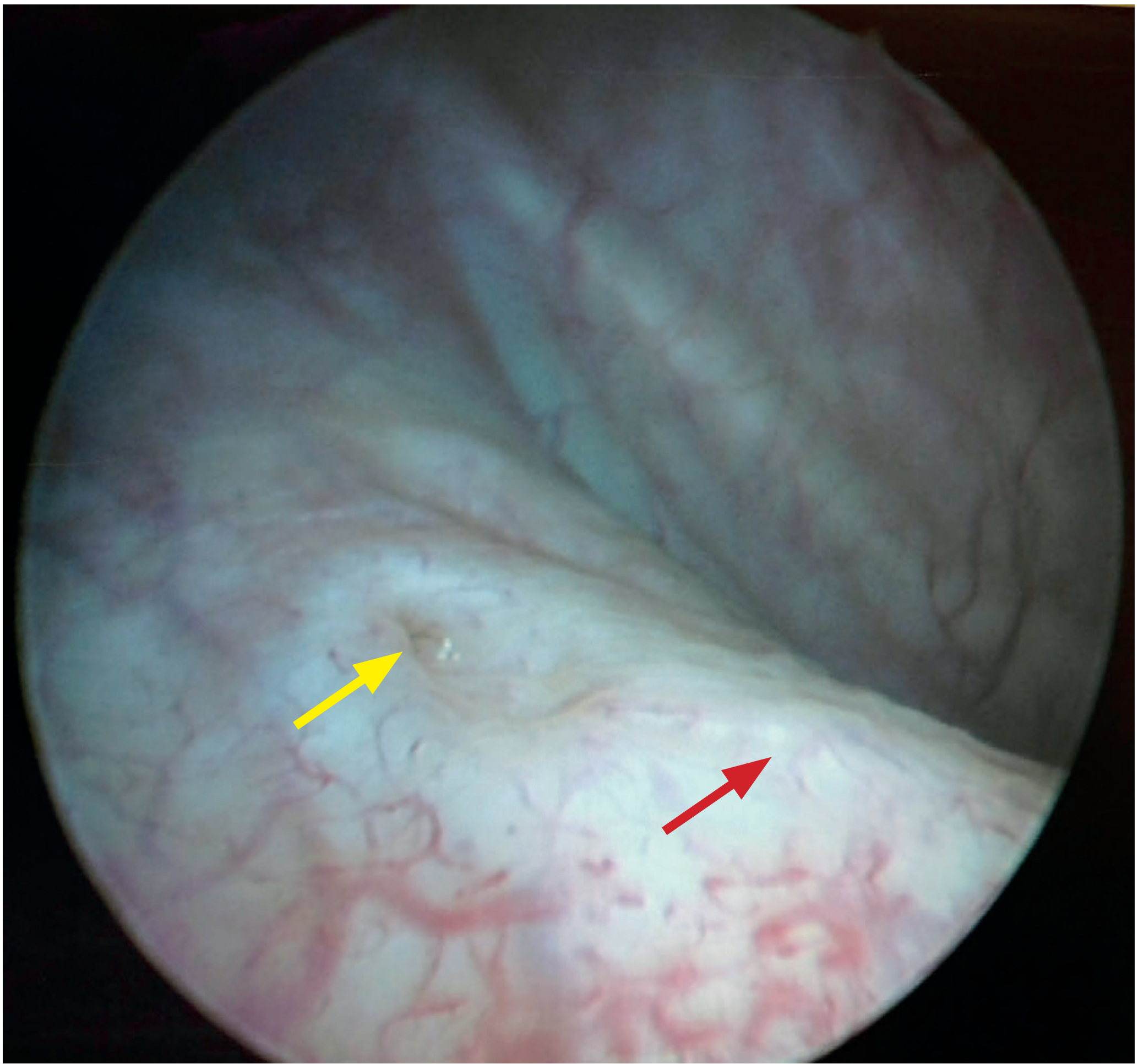
Normal bladder mucosa with right ureteric orifice (yellow arrow) and interureteric bar (red arrow):
TURP (Transurethral Resection of the Prostate)
Definition and Status
TURP is the gold standard surgical treatment for bladder outlet obstruction (BOO) caused by benign prostatic hyperplasia (BPH). Among all BPH therapies, TURP produces the largest decrease in urinary symptoms, the largest increase in urinary flow rate, and the largest decrease in voiding pressure. - Hinman's Atlas of Urologic Surgery
Indications
- Symptomatic BPH refractory to medical therapy (alpha-blockers, 5-alpha reductase inhibitors)
- Acute urinary retention (refractory)
- Recurrent haematuria from BPH
- Bladder stones / diverticula secondary to BOO
- Renal impairment from BOO
- Prostate cancer patients not suitable for radical prostatectomy (palliation of obstruction)
- Concomitant prostatic calculi release - Campbell-Walsh-Wein Urology; Bailey and Love's
Preoperative
- Prophylactic IV antibiotics (single dose before resection)
- Cystourethroscopy must be performed before any cutting begins - to exclude bladder tumour, stone, or stricture
- Gentle meatal/fossa navicularis dilation if needed (Van Buren sounds, 18 Fr upward)
Patient Positioning
Dorsal lithotomy position, perineum at the table edge to allow the resectoscope to angle upward for anterior prostatic access.
The Resectoscope
A specialised endoscopic instrument with an electrode capable of both cutting and coagulating. Available in monopolar and bipolar configurations:
- Monopolar: requires non-conductive (electrolyte-free) irrigant (glycine 1.5%, sorbitol 3.3%, mannitol 5%) - risk of TUR syndrome
- Bipolar: uses normal saline irrigant - eliminates risk of dilutional hyponatremia
Cutting devices: thin loops (cleaner cut, less coagulation), thick loops, rollers/roller balls/buttons (desiccation, better haemostasis for larger glands).
Surgical Steps (Key Landmarks)
- Cystourethroscopy to survey the entire urothelium
- Pass resectoscope sheath into bladder
- Median lobe resection first (if enlarged) - resected down to circular bladder neck fibres
- Bladder neck and prostatic floor resected toward verumontanum
- Anterior prostate resected at 12 o'clock
- Lateral lobes taken down
- Verumontanum is the key distal landmark - must NOT be resected (risk of sphincter damage and incontinence)
- Chips irrigated out; haemostasis achieved; 3-way catheter placed
- Hinman's Atlas of Urologic Surgery
Anaesthesia
- Spinal (regional) or general anaesthesia - outcomes equivalent
- Historically spinal was preferred because an awake patient allows early detection of TUR syndrome
- Today, bipolar TURP with saline and less aggressive resection makes general anaesthesia widely acceptable
Irrigating Solutions
| Solution | Osmolality (mOsm/L) | Advantages | Disadvantages |
|---|---|---|---|
| Distilled water | 0 | Best visibility | Haemolysis, haemoglobinuria, hyponatraemia |
| Glycine 1.5% | 200 | Less TUR syndrome risk | Transient visual disturbance, hyperammonaemia |
| Sorbitol 3.3% | 165 | Similar to glycine | Hyperglycaemia, possible lactic acidosis |
| Mannitol 5% | 275 | Isosmolar, not metabolised | Osmotic diuresis, volume expansion |
| Normal saline (0.9%) | ~308 | Eliminates hyponatraemia risk | Only usable with bipolar TURP |
- Barash Clinical Anesthesia, 9e; Miller's Anesthesia, 10e
TUR Syndrome
Definition
Symptomatic hyponatraemia + hypervolaemia resulting from absorption of hypotonic, electrolyte-free irrigant through open venous sinuses during TURP (or TURBT, hysteroscopy, ureteroscopy).
- Complicates 10-15% of TURP procedures
- Onset: 15 minutes to 24 hours after start of resection
Risk Factors
- Prolonged resection (> 1 hour)
- Increased intravesical pressure
- Hypotonic irrigant
- Open venous sinuses (large gland, capsular tear)
Clinical Features
| System | Features |
|---|---|
| CNS | Nausea/vomiting, visual disturbance (glycine toxicity), confusion, agitation, seizures, reduced consciousness |
| CVS | Hypertension, then hypotension; bradycardia |
| Biochemical | Hyponatraemia (Na+ < 120 mEq/L in severe cases), hypo-osmolality |
The classic CNS signs are due to acute serum hypoosmolality causing brain oedema rather than hyponatraemia per se.
Prevention
- Use bipolar TURP with normal saline irrigant (eliminates hyposmolar risk)
- Monitor fluid balance - halt if > 1000 mL absorbed (males)
- Limit intravesical pressure < 15-25 mmHg
- Limit resection duration to < 1 hour unless carefully monitoring for syndrome
- Regional anaesthesia allows neurological monitoring in awake patient
Management
| Severity | Na+ | Treatment |
|---|---|---|
| Mild | > 120 mEq/L | Fluid restriction + furosemide (loop diuretic) |
| Severe | < 120 mEq/L | 3% NaCl IV at < 100 mL/hr; stop when Na+ > 120 mEq/L |
| Seizures | Any | IV magnesium (counteracts glycine's NMDA excitation) |
| Normal osmolality | Any | Haemodialysis preferred over hypertonic saline |
-
Avoid rapid correction - risk of central pontine myelinolysis (demyelination)
-
Terminate procedure, ensure oxygenation and circulatory support, ECG, electrolytes/ABG
-
Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e; Morgan & Mikhail's Clinical Anesthesiology 7e
Key Differences: Monopolar vs Bipolar TURP
| Feature | Monopolar | Bipolar |
|---|---|---|
| Irrigant | Non-conducting (glycine/sorbitol) | Normal saline |
| TUR syndrome risk | Yes | Eliminated (no hyponatraemia) |
| Haemostasis | Good | Good |
| Laser TURP | - | No requirement for non-conductive fluid; less blood loss; lower transfusion rates |
Comparison with TUIP (Transurethral Incision of Prostate)
- TUIP: no tissue removed; 1-2 incisions from bladder neck to verumontanum - widens the prostatic channel
- Ideal for younger men, prostate < 30 g, no significant lateral lobe hypertrophy, primary bladder neck obstruction
- Not gold standard; less durable than TURP for larger glands; not suitable when median lobe is obstructive
This is a shared conversation. Sign in to Orris to start your own chat.