Vitals normal patient feels dizzy. Opd
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a structured OPD approach for a patient presenting with dizziness and normal vitals.
Dizziness with Normal Vitals - OPD Approach
Step 1: Clarify What "Dizziness" Actually Means
Patients use "dizziness" loosely. Pin it down first - it changes everything:
| Type | Patient Description | Think Of |
|---|---|---|
| Vertigo | Spinning, room moving | Vestibular (BPPV, neuritis, Meniere's) |
| Presyncope | About to faint, blackout feeling | Cardiac, orthostatic (check lying/standing BP) |
| Disequilibrium | Imbalance, unsteady gait | Cerebellar, neuropathy, Parkinson's |
| Lightheadedness | Floating, vague wooziness | Anxiety, hyperventilation, anemia |
Step 2: Focused History
Timing - key diagnostic clue:
- Seconds (<1 min, position-provoked) - BPPV is most likely
- Minutes - TIA posterior circulation, vestibular migraine
- Hours (2-12 hrs) - Meniere's disease
- Days (constant, acute onset) - Vestibular neuritis / labyrinthitis
Provoking factors:
- Head position changes (lying down, rolling in bed, looking up) → BPPV
- Standing up → Orthostatic hypotension (check lying/standing BP even if "normal")
- Stress, hyperventilation → Anxiety/panic
Associated symptoms:
- Hearing loss, tinnitus, ear fullness → Peripheral (Meniere's, labyrinthitis)
- Diplopia, dysarthria, facial numbness, limb weakness/ataxia → Central - URGENT (posterior fossa stroke)
- Headache → Vestibular migraine
- First episode, sudden severe → Do not miss stroke
Medications: Antihypertensives, antiepileptics, aminoglycosides, sedatives
Step 3: Examination
Ocular motility:
- Nystagmus direction: Unidirectional horizontal = peripheral; direction-changing or vertical = central
- Nystagmus suppressed by fixation = peripheral; not suppressed = central
- Pure vertical or pure torsional nystagmus = central sign
Head Impulse Test (HIT / VOR test):
- Abnormal (corrective saccade seen) = peripheral vestibular lesion (reassuring)
- Normal HIT in acute vertigo = suspect central cause (stroke until proven otherwise)
HINTS exam (for acute prolonged vertigo):
- Head Impulse = Normal → central
- IN = direction-changing nystagmus → central
- Test of Skew = skew deviation → central Any one "central" feature → neuroimaging urgently
Dix-Hallpike test (if BPPV suspected):
- Positive: upbeat-torsional nystagmus with latency, fatigable → posterior canal BPPV confirmed
Romberg, tandem gait, cerebellar tests - check for central features
Step 4: Peripheral vs Central - Red Flags
| Red Flag - Refer/Investigate URGENTLY | Benign Peripheral Features |
|---|---|
| New headache + dizziness | Brief episodes (<1 min), position-provoked |
| Neurological deficits (diplopia, dysarthria, ataxia, weakness) | Nystagmus suppressed by fixation |
| Direction-changing nystagmus | Unilateral hearing loss/tinnitus |
| Normal head impulse test in acute vertigo | Abnormal HIT (corrective saccade) |
| Age >50, vascular risk factors | Dix-Hallpike positive with torsional nystagmus |
| Sudden onset ("thunderclap") | Gradual onset, known migraine history |
Step 5: Most Likely Diagnoses in OPD
BPPV (most common overall)
- Brief positional vertigo (<1 min), triggered by lying down, rolling in bed, looking up
- Dix-Hallpike positive
- Treat with Epley Maneuver (see below) - highly effective, no medications needed
Vestibular Neuritis
- Acute onset, sustained vertigo for days, often post-viral
- No hearing loss (if hearing loss = labyrinthitis)
- Abnormal HIT on affected side
- Treat: Short-course corticosteroids (evidence uncertain); vestibular suppressants for acute phase only (max 3 days - prolonged use impedes recovery); encourage early mobilization + vestibular rehab
Vestibular Migraine
- Episodic vertigo (minutes to hours), often without headache
- Prior or current migraine history
- Treat like migraine (triptans acutely; preventive therapy for frequent episodes)
Meniere's Disease
- Triad: episodic vertigo (2-12 hrs) + fluctuating low-frequency hearing loss + tinnitus + ear fullness
- Refer ENT
Anxiety / Functional
- Persistent dizziness, worse with crowds/movement, often history of anxiety/panic
- Persistent Postural-Perceptual Dizziness (PPPD) is a recognized entity
- Vestibular rehab + CBT
Step 6: Epley Maneuver (for BPPV)
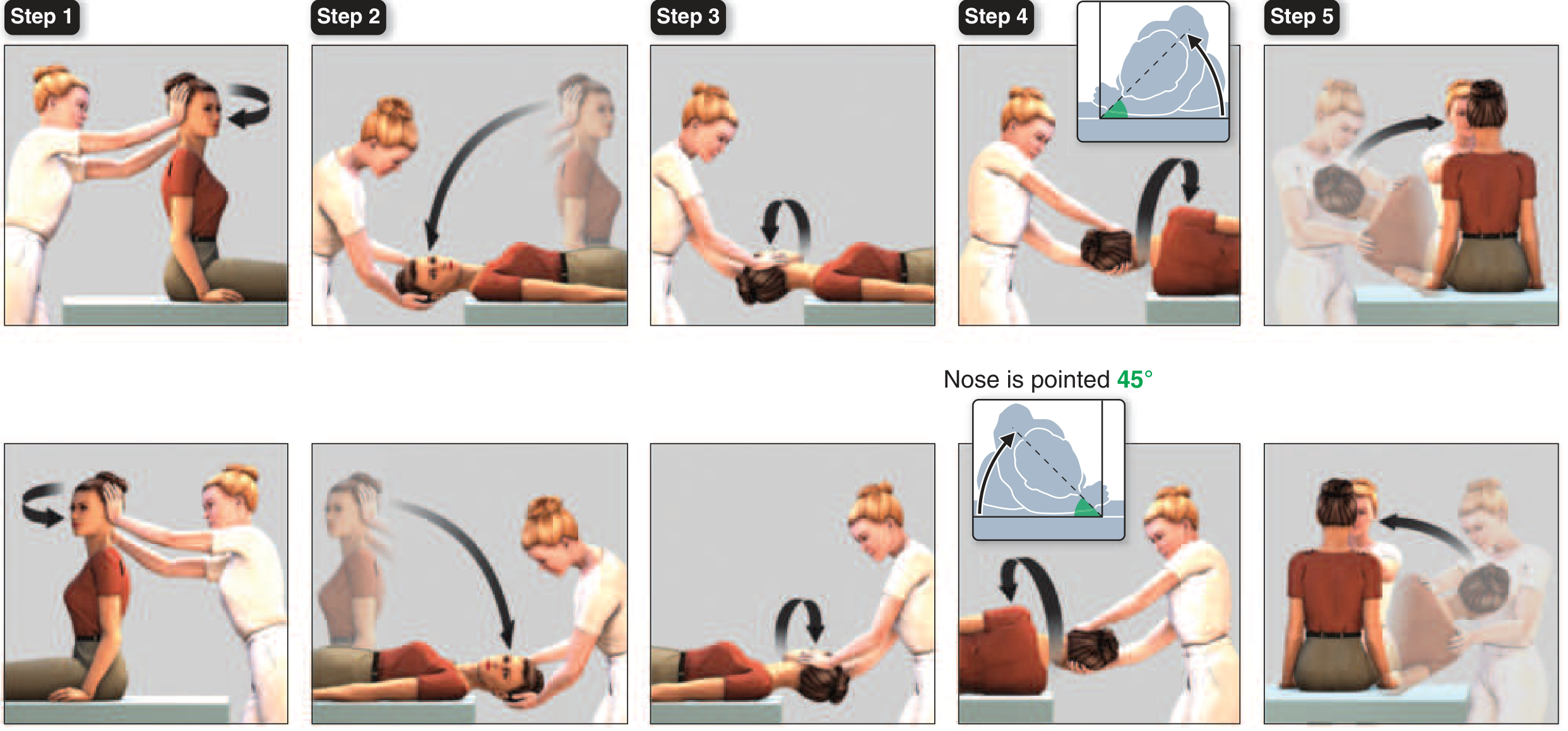
Steps (for right posterior canal BPPV):
- Seat patient, turn head 45° toward affected (right) ear
- Quickly lower to head-hanging position - hold 30 s until nystagmus resolves
- Rotate head 90° to opposite side (now 45° left) - hold 30 s
- Roll patient onto their side, rotating head another 90° so nose points 45° downward - hold 30 s
- Sit patient up slowly
Repeat to confirm. Highly effective in a single session.
(Source: Harrison's Principles of Internal Medicine 22E, Fig. 24-1)
Step 7: Investigations (as needed)
| Test | When |
|---|---|
| Lying/standing BP | Any presyncope component, elderly |
| CBC | Anemia-related dizziness |
| Blood glucose | Hypoglycemia |
| ECG | Palpitations, presyncope, elderly |
| Pure tone audiogram | Hearing loss present |
| MRI brain (posterior fossa) | Any central red flag, HINTS central, first severe episode |
| Thyroid function | If other features suggest thyroid disease |
Summary
In an OPD with normal vitals, BPPV is the single most common cause of dizziness - quick Dix-Hallpike and Epley maneuver can diagnose and treat it in the same visit. The most important task is ruling out central (posterior fossa) pathology using the HINTS exam before labeling any acute prolonged vertigo as peripheral. Normal vitals do not exclude TIA or early stroke.
Sources: Harrison's Principles of Internal Medicine 22E, Ch. 24; Scott-Brown's Otorhinolaryngology, Ch. 62
This is a shared conversation. Sign in to Orris to start your own chat.