Stroke and mi management in emergency er….with pnemonics
Reading File
Finding Sources
Finding Sources
Searching the Web
stroke MI emergency management mnemonics ER 2024
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have solid content from Rosen's Emergency Medicine and Fuster's The Heart. Let me compile the complete answer with all mnemonics.
Stroke & MI: Emergency Management with Mnemonics
PART 1: ACUTE ISCHEMIC STROKE
Recognition - "BE-FAST"
| Letter | Meaning |
|---|---|
| B | Balance - sudden loss |
| E | Eyes - sudden vision change |
| F | Face drooping |
| A | Arm weakness |
| S | Speech difficulty |
| T | Time to call 911 |
Classic older version: FAST (Face, Arm, Speech, Time)
Initial ER Assessment - "ROSIER" Score
(Recognition Of Stroke In the Emergency Room)
| Item | Points |
|---|---|
| Loss of consciousness/syncope | -1 |
| Seizure | -1 |
| Asymmetric facial weakness | +1 |
| Asymmetric arm weakness | +1 |
| Asymmetric leg weakness | +1 |
| Speech disturbance | +1 |
| Visual field defect | +1 |
| Score >0 = likely stroke |
Immediate ER Management - "TIME IS BRAIN"
"DONT" - Initial stabilization before specific treatment:
| Letter | Meaning |
|---|---|
| D | Dextrose (check glucose - treat hypoglycemia) |
| O | Oxygen (maintain SpO2 >94%) |
| N | Naloxone (if opioid overdose suspected) |
| T | Thiamine (before dextrose) |
tPA/Alteplase Eligibility - "SMART"
| Letter | Meaning |
|---|---|
| S | Symptoms onset <4.5 hours |
| M | Mild-moderate deficit (NIHSS documented) |
| A | Age ≥18 (no upper age cutoff per current guidelines) |
| R | Rule out hemorrhage (CT head negative) |
| T | Target BP <185/110 before giving tPA |
tPA dose: 0.9 mg/kg IV (max 90 mg) - 10% as bolus, rest over 60 min
tPA Contraindications - "NO tPA"
| N | No anticoagulants (recent therapeutic heparin/warfarin) |
| O | Onset >4.5 hours OR unknown |
| t | Trauma/surgery within 3 months (head or major) |
| P | Prior stroke + diabetes combo |
| A | Active bleeding / intracranial hemorrhage |
BP Management in Acute Ischemic Stroke
- No tPA planned: Only treat if BP >220/120 mmHg; reduce ~15% over 24 hours
- tPA planned: Must get BP <185/110 before dosing, maintain <180/110 after
- Agents of choice: Labetalol (20 mg IV bolus q10 min) or Nicardipine (5-15 mg/hr IV)
- Avoid sodium nitroprusside (raises ICP)
(Rosen's Emergency Medicine)
Mechanical Thrombectomy (Large Vessel Occlusion)
- Consider in all eligible patients with LVO within 24 hours of last known well (extended window with DAWN/DEFUSE-3 criteria)
- NIHSS ≥6, CT perfusion showing salvageable tissue
Hemorrhagic Stroke (ICH) BP Target
- Systolic >220: Rapid IV reduction
- Systolic 150-220: Target SBP 140 mmHg
- Use nicardipine/labetalol/clevidipine
PART 2: ACUTE MI (STEMI/NSTEMI)
Recognition - "CHEST PAIN"
| Letter | Meaning |
|---|---|
| C | Characteristic: crushing, pressure, radiating |
| H | History: prior CAD, risk factors |
| E | ECG: ST elevation, new LBBB, reciprocal changes |
| S | Sweating, nausea, vomiting |
| T | Troponin elevation |
| P | Pulse oximetry / BP check |
| A | Age/sex risk |
| I | Imaging (CXR, echo) |
| N | Note time of symptom onset |
Initial ER Management - "MONA" (classic) + "BATMAN"
Classic MONA:
| Letter | Meaning | Notes |
|---|---|---|
| M | Morphine | Use cautiously - may worsen outcomes in some ACS |
| O | Oxygen | Only if SpO2 <90% |
| N | Nitrates | Sublingual NTG → IV if ongoing pain; avoid if RV infarct |
| A | Aspirin | 162-325 mg chewed immediately |
Extended - "BATMAN" (modern ACS bundle):
| Letter | Meaning |
|---|---|
| B | Beta-blocker (oral, avoid IV in acute decompensation) |
| A | Aspirin 325 mg |
| T | Ticagrelor or clopidogrel (P2Y12 inhibitor - dual antiplatelet) |
| M | Morphine (judicious) / Monitor continuously |
| A | Anticoagulation (UFH/enoxaparin/bivalirudin) |
| N | Nitrates |
STEMI Reperfusion Strategy - "4 Ds"
(from Rosen's Emergency Medicine)
| D | Meaning |
|---|---|
| Door | Events before arrival / prehospital |
| Data | ECG within 5-10 min of arrival |
| Decision | STEMI diagnosis + therapy decision |
| Drug/Device | Fibrinolytic drug OR balloon catheter across lesion |
Goal: Door-to-balloon (PCI) <90 min | Door-to-needle (fibrinolysis) <30 min
PCI vs Fibrinolysis Decision - "PPCI Preferred If..."
- PCI available within 120 min of first medical contact
- Cardiogenic shock
- Fibrinolysis contraindicated
- Large anterior STEMI / high-risk features
Fibrinolysis if PCI not timely available:
Agents: Alteplase (tPA), Reteplase, Tenecteplase, Streptokinase
Anticoagulation in STEMI - "HAB"
| Agent | Setting |
|---|---|
| H | Heparin (UFH) - most common, 70-100 U/kg bolus for pPCI |
| A | Alteplase/fibrinolytic setting - UFH or enoxaparin |
| B | Bivalirudin - HIT patients or alternative to UFH |
(Fuster and Hurst's The Heart, 15th Ed)
Antiplatelet Therapy - "DAPT"
Dual AntiPlatelet Therapy:
- Aspirin 325 mg loading → 81 mg daily
- P2Y12 inhibitor: Ticagrelor (preferred) or Clopidogrel or Prasugrel
Give loading dose BEFORE PCI!
STEMI Contraindications to Fibrinolysis - "BASH"
| Letter | Meaning |
|---|---|
| B | Bleeding history (active/recent intracranial) |
| A | Aortic dissection suspected |
| S | Surgery/trauma within 3 weeks |
| H | Hypertension uncontrolled (>180/110) |
Nitroglycerin Absolute Contraindications - "SHoP"
| S | Sildenafil/PDE5 inhibitor use within 24-48 hrs |
| H | Hypotension (SBP <90) |
| P | (Right ventricular) infarct (inferior STEMI with RV involvement) |
QUICK COMPARISON TABLE
| Feature | Acute Stroke | Acute MI (STEMI) |
|---|---|---|
| Time window | <4.5 hrs (tPA) / <24 hrs (thrombectomy) | <12 hrs (PCI optimal) |
| Key drug | tPA (alteplase) | Aspirin + P2Y12 + heparin |
| Imaging | CT head immediately | 12-lead ECG immediately |
| BP target (no intervention) | <220/120 (permissive) | Control if hypertensive |
| BP target (pre-procedure) | <185/110 (tPA) | <180/110 |
| Reperfusion | IV tPA or mechanical thrombectomy | Primary PCI (preferred) or fibrinolysis |
| Antiplatelets | Aspirin 325 mg (after 24 hrs if tPA given) | Aspirin + P2Y12 immediately |
MASTER MNEMONIC - "STROKE" vs "HEART"
STROKE (Ischemic):
- S - Sugar check (glucose)
- T - Time onset (<4.5 hrs for tPA)
- R - Rule out hemorrhage (CT)
- O - O2 if SpO2 <94%
- K - Keep BP permissive (unless tPA)
- E - Evaluate LVO → thrombectomy
HEART (MI):
- H - Heparin + anticoagulation
- E - ECG in 10 min (diagnose STEMI)
- A - Aspirin 325 mg + P2Y12
- R - Reperfusion (PCI <90 min / lysis <30 min)
- T - Troponin + monitoring
Sources:
- Rosen's Emergency Medicine - ACS and stroke ER management chapters
- Fuster and Hurst's The Heart, 15th Ed - STEMI antiplatelet/anticoagulation protocols
- Bradley and Daroff's Neurology in Clinical Practice - Acute stroke treatment guidelines
Ecg in mi in ER things to know must from basics
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG changes acute MI STEMI basics leads localization ER interpretation 2024
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive textbook content and real ECG images. Let me compile the complete answer.
ECG in MI - Everything You Must Know (Basics to ER)
1. THE BASICS: ECG PAPER & MEASUREMENTS
ECG paper speed = 25 mm/s
- 1 small box = 0.04 sec (40 ms) horizontally = 0.1 mV vertically
- 1 large box = 0.20 sec (200 ms) = 0.5 mV
The Normal ECG Wave Sequence: "PQRST"
- P = atrial depolarization
- PR interval = 0.12-0.20 sec (3-5 small boxes)
- QRS = ventricular depolarization (<0.12 sec)
- ST segment = early repolarization (should be on the isoelectric line)
- T wave = ventricular repolarization
2. SEQUENTIAL ECG CHANGES IN MI - "HOT Q"
The ECG changes in MI follow a time-based sequence:
| Time | Change | What It Means |
|---|---|---|
| Minutes | Hyperacute T waves (tall, peaked, symmetric) | Very earliest sign - subendocardial injury |
| 1-4 hrs | ST elevation (convex/tombstone) | Transmural injury - STEMI |
| Hours | T wave inversion | Ischemia/evolving infarct |
| 6-24 hrs | Q waves develop (pathologic) | Myocardial necrosis |
| Days-weeks | ST normalizes, Q waves persist | Old/evolving MI |
Mnemonic: "H-I-Q-T" (Hours-Injury-Ischemia-Quilts of necrosis)
Hyperacute T → ST Elevation → T inversion → Q waves
3. STEMI DIAGNOSTIC CRITERIA (Must Memorize)
ST Elevation Thresholds (ACC/AHA):
| Leads | ST Elevation Required |
|---|---|
| V2-V3 (men ≥40 yr) | ≥2 mm |
| V2-V3 (men <40 yr) | ≥2.5 mm |
| V2-V3 (women) | ≥1.5 mm |
| All other leads | ≥1 mm in ≥2 contiguous leads |
Mnemonic: "2-2.5-1.5-1" (V2-V3 men / V2-V3 young men / V2-V3 women / all others)
Must be in ≥2 contiguous leads to diagnose STEMI
4. LOCALIZATION BY LEADS - THE MOST IMPORTANT TABLE
(from Tintinalli's Emergency Medicine)
| Territory | Leads with ST Elevation | Culprit Vessel |
|---|---|---|
| Anteroseptal | V1, V2 (±V3) | LAD (proximal) |
| Anterior | V1, V2, V3, V4 | LAD |
| Anterolateral | V1-V6, I, aVL | LAD (proximal) |
| Lateral (High) | I, aVL | Circumflex or Diagonal |
| Inferior | II, III, aVF | RCA (80%) or LCx (20%) |
| Inferolateral | II, III, aVF + V5, V6 | RCA or LCx |
| Posterior | Tall R in V1-V2, ST depression V1-V3 | RCA or LCx |
| Right Ventricle | ST elevation II,III,aVF + V3R-V6R | RCA (proximal) |
Mnemonic to remember leads: "I See Pretty Leads, A Really Intelligent Physician"
- Inferior = II, III, aVF
- Septal = V1, V2
- Anterior = V3, V4
- Lateral = V5, V6, I, aVL
5. REAL ECG EXAMPLES FROM TEXTBOOKS
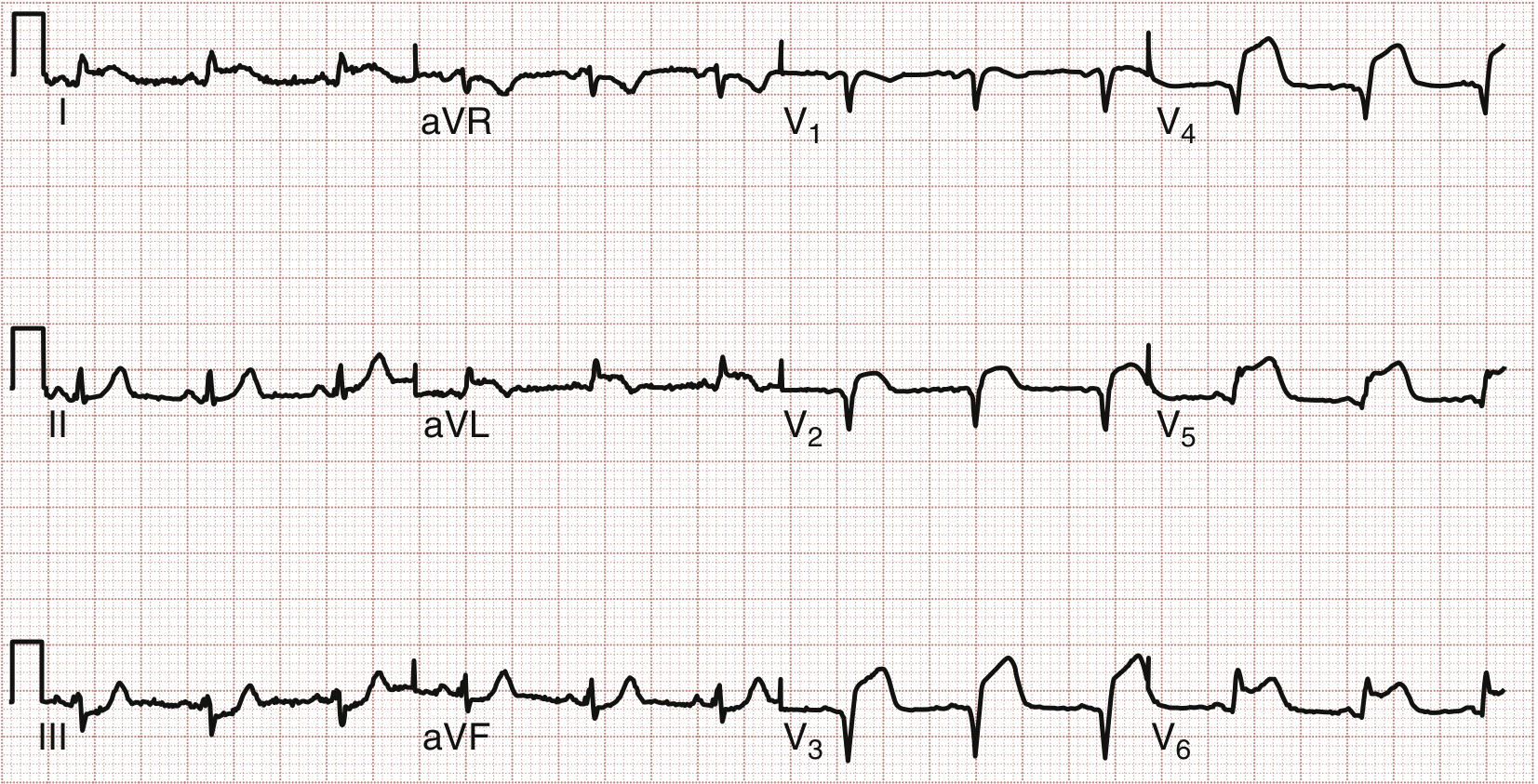
Anterolateral STEMI (Rosen's Emergency Medicine)
Proximal LAD occlusion - ST elevation in V1-V4 (anterior) and I, aVL, V5, V6 (lateral):
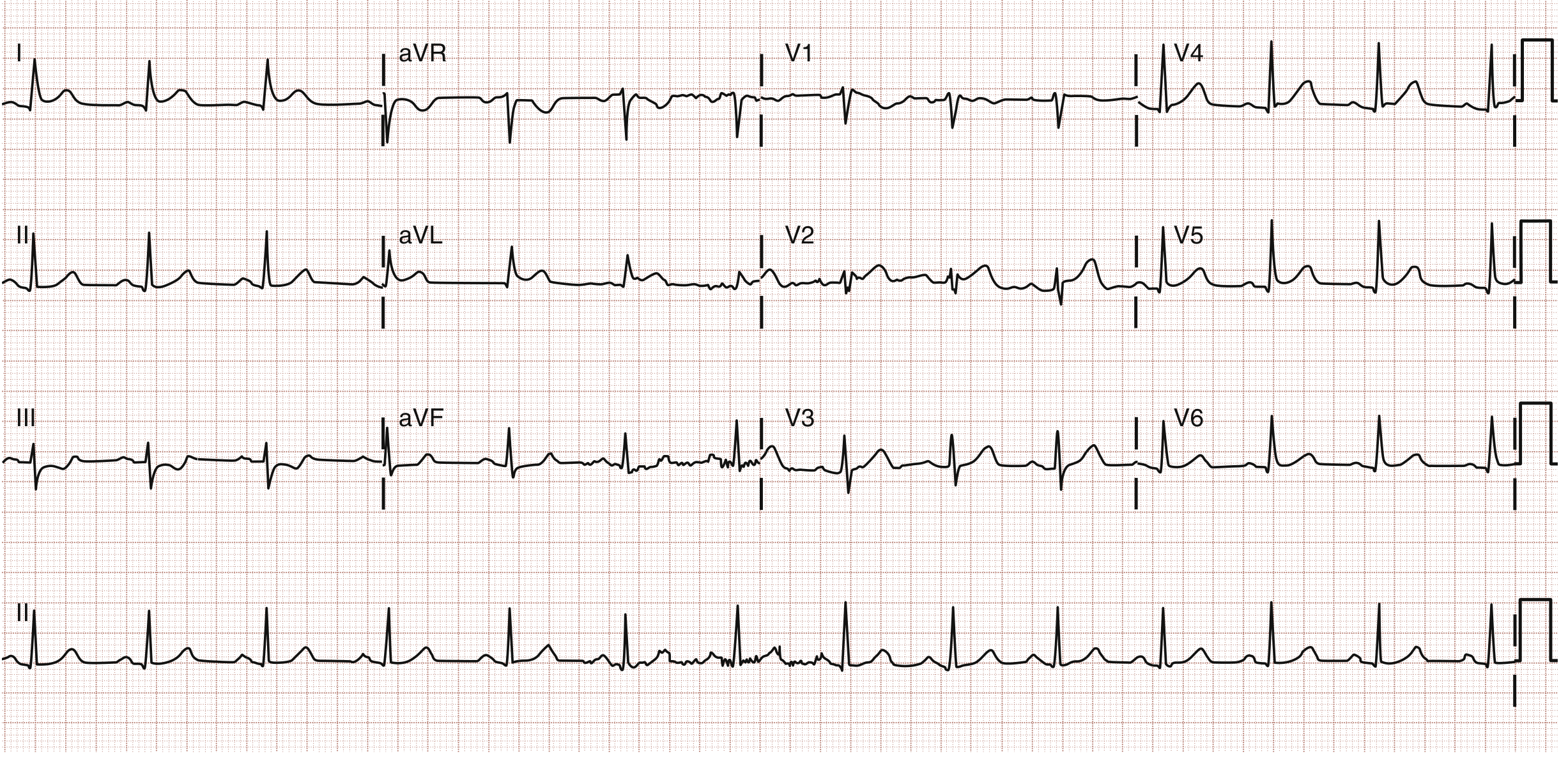
High Lateral MI (I and aVL elevation - Circumflex/D1 occlusion)
ST elevation in leads I and aVL with reciprocal changes in II, III, aVF:
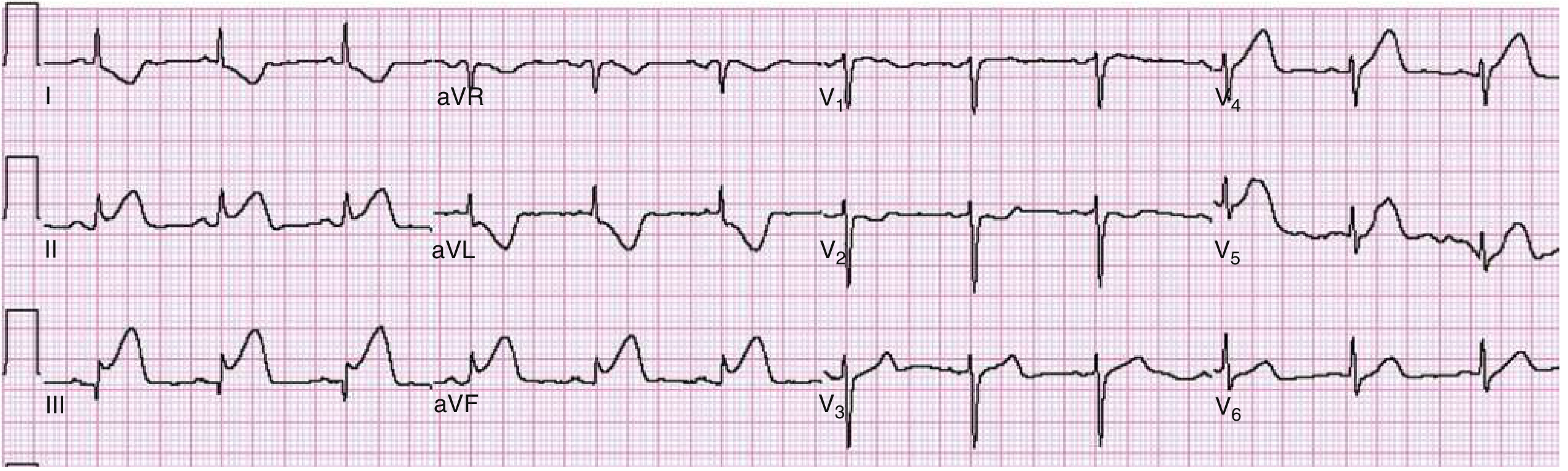
Inferior MI with Reciprocal Changes
Marked ST elevation in II, III, aVF - classic reciprocal ST depression in I and aVL:
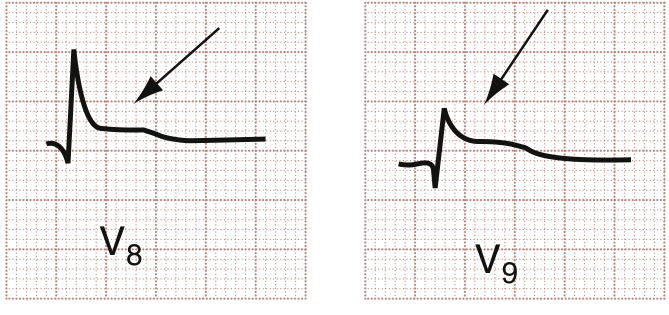
Posterior MI - Leads V8, V9
ST elevation visible in posterior leads V8, V9 (subtle but diagnostic):
6. RECIPROCAL CHANGES - "THE MIRROR RULE"
Reciprocal changes = ST depression in leads facing the opposite wall.
| Primary STEMI | Reciprocal Depression Seen In |
|---|---|
| Inferior (II, III, aVF) | I, aVL |
| Anterior (V1-V4) | II, III, aVF (occasionally) |
| Lateral (I, aVL) | II, III, aVF |
Why they matter: Reciprocal changes indicate a LARGER infarct, increased mortality, and higher risk of cardiogenic shock (Tintinalli's; Rosen's).
7. POSTERIOR MI - "THE INVISIBLE INFARCT"
The posterior wall has no direct leads in standard 12-lead ECG.
You must recognize it from mirror image changes in V1-V3:
Mnemonic "HURT" in V1-V2 = Posterior MI:
| Letter | Finding |
|---|---|
| Horizontal | ST depression (not sloped) |
| Upright | T wave (should be inverted normally if ischemic) |
| R wave | Tall, wide R wave (>0.04 sec) |
| Tall R/S | Ratio >1 in V1-V2 |
Confirm with posterior leads: V7 (left mid-axillary), V8 (left posterior axillary), V9 (left paraspinal) - look for ≥0.5 mm ST elevation.
8. RIGHT VENTRICULAR (RV) MI - "CRITICAL PEARL"
- Always occurs with inferior STEMI
- Present in ~30-40% of inferior MIs
- Clue: ST elevation greater in lead III than lead II + ST elevation in V1
How to diagnose: Get right-sided leads (V3R-V6R)
- ST elevation ≥0.5 mm in V4R = diagnostic
Clinical triad of RV infarct:
Hypotension + Elevated JVP + Clear lungs (Kussmaul's sign)
ER Management rule:
AVOID nitrates - they drop preload and will cause cardiovascular collapse in RV infarct! GIVE IV fluids (500-1000 mL NS bolus) to maintain RV filling pressure.
9. PATHOLOGIC Q WAVES
(Washington Manual of Medical Therapeutics)
Q waves = myocardial necrosis (irreversible cell death)
Criteria for pathologic Q wave:
- In V2-V3: ≥0.02 sec (1 small box) wide, or any QS complex
- In other leads: ≥0.03 sec wide AND ≥0.1 mV deep, in ≥2 contiguous leads
- Isolated Q in lead III or V1 = normal variant (don't panic)
Important:
- New Q waves alone are NOT an indication for thrombolysis if ST is normalized
- Always compare with an old ECG to determine chronicity
10. STEMI EQUIVALENTS - "NOT JUST ST ELEVATION"
Some STEMIs do NOT show classic ST elevation. Know these:
| Pattern | What It Means |
|---|---|
| New LBBB | STEMI equivalent (if truly new) - but <10% have AMI |
| De Winter T waves | Tall, upright T with ST depression in V1-V6 = proximal LAD occlusion (no elevation!) |
| Wellens' syndrome | Biphasic or deep T inversion in V2-V3 = critical LAD stenosis (post-ischemia) |
| aVR ST elevation | Left main or proximal LAD occlusion (global ischemia) |
| Posterior ST depression V1-V3 | Posterior STEMI (mirror image - see above) |
Mnemonic "DWWA":
- De Winter = LAD proximal occlusion (no STE)
- Wellens = Threatened LAD (critical stenosis)
- Wide new LBBB = STEMI equivalent
- AVR elevation = Left main/proximal LAD
11. ST ELEVATION MIMICS - MUST RULE OUT
(Washington Manual of Medical Therapeutics)
Mnemonic "PHELP B":
| Letter | Mimic |
|---|---|
| P | Pericarditis (saddle-shaped, diffuse STE, PR depression) |
| H | Hyperkalemia (peaked T, widened QRS, sine wave) |
| E | Early repolarization (J-point notching, usually young males) |
| L | LVH with strain pattern |
| P | PE (Pulmonary embolism - S1Q3T3 pattern) |
| B | Brugada syndrome (V1-V2 coved ST elevation) |
Key differentiator for Pericarditis vs STEMI:
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST shape | Saddle/concave up | Convex/tombstone |
| PR segment | Depressed (pathognomonic) | Normal |
| Leads affected | Diffuse (all except aVR) | Regional |
| Reciprocal changes | None | Present |
| Q waves | No | Yes (later) |
12. ER ECG PROTOCOL - "10-MINUTE RULE"
Goal: ECG within 10 minutes of patient arrival for ALL chest pain
Step-by-step ER ECG approach:
1. RATE → Normal (60-100), Tachy, Brady
2. RHYTHM → Regular? P before every QRS?
3. AXIS → Normal (-30° to +90°)
4. INTERVALS → PR, QRS, QTc
5. ST/T → Elevation? Depression? Inversion?
6. Q WAVES → Pathologic?
7. COMPARE → Old ECG (most important!)
Mnemonic: "RRAISTQ-C" = Rate, Rhythm, Axis, Intervals, ST, T waves, Q waves, Compare
13. QUICK-FIRE PEARLS FOR ER
| Pearl | Rule |
|---|---|
| Inferior MI → always get right-sided leads | Rule out RV infarct |
| Inferior MI → ST III > ST II | Suggests RCA occlusion |
| Inferior MI → ST II > ST III | Suggests LCx occlusion |
| ST depression V1-V3 + upright T | Think posterior MI |
| aVL reciprocal change | Strong marker of inferior STEMI |
| New LBBB + symptoms | Treat as STEMI until proven otherwise (use Sgarbossa criteria) |
| Serial ECGs | If first ECG non-diagnostic but high suspicion, repeat at 15-30 min |
| Right-sided ECG | Get V4R - ST elevation ≥0.5 mm = RV MI confirmed |
| ST elevation in aVR | Left main occlusion - highest risk patient |
14. SGARBOSSA CRITERIA (for LBBB + suspected MI)
When LBBB is present, standard STEMI criteria don't apply. Use Sgarbossa:
| Criterion | Points |
|---|---|
| ST elevation ≥1 mm concordant with QRS (in same direction) | 5 |
| ST depression ≥1 mm in V1, V2, or V3 | 3 |
| ST elevation ≥5 mm discordant with QRS (in opposite direction) | 2 |
Score ≥3 = highly suggestive of AMI in LBBB
Modified Sgarbossa: discordant STE/QRS ratio >0.25 is more specific than the 5mm cutoff.
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study - ECG chapter (Table 49-4, 49-5)
- Rosen's Emergency Medicine - Anatomic localization of AMI, posterior/RV MI sections
- Washington Manual of Medical Therapeutics - ST elevation differential diagnosis and Q wave criteria
This is a shared conversation. Sign in to Orris to start your own chat.