How to approach anemia pediatrics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anemia" AND "children" AND "diagnosis"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content from the Harriet Lane Handbook. Let me compile a thorough, well-organized answer.
Approach to Anemia in Pediatrics
Source: The Harriet Lane Handbook (Johns Hopkins Hospital), 23rd edition
1. Screening
The AAP recommends screening between 9-12 months, with a repeat level 6 months later.
Screen yearly in high-risk children with:
- Prematurity or low birth weight
- Lead exposure
- Exclusive breastfeeding without iron supplementation beyond 4 months
- Diet lacking iron-fortified cereals or iron-rich foods
- Feeding problems, poor growth, or inadequate nutrition
2. Definition
Anemia = Hb two standard deviations below the mean for age. Normal ranges are age-dependent (not a single cutoff across all pediatric ages).
3. Framework: Approach by MCV + Reticulocyte Index
The core approach uses MCV (cell size) and reticulocyte index to guide the workup.
Step 1 - Calculate the Reticulocyte Index
Reticulocyte Index = % reticulocytes × patient Hct / normal Hct
- >2 = adequate RBC production (hemolytic or blood loss)
- <2 = hypoproliferative anemia (bone marrow failure, nutritional deficiency, chronic disease)
Step 2 - Classify by MCV
| MCV | Pathway |
|---|---|
| Low (microcytic) | Check Fe, TIBC, Ferritin |
| Normal (normocytic) | Check reticulocyte index |
| High (macrocytic) | Check B12, folate, MMA/homocysteine |
4. Diagnostic Flowcharts
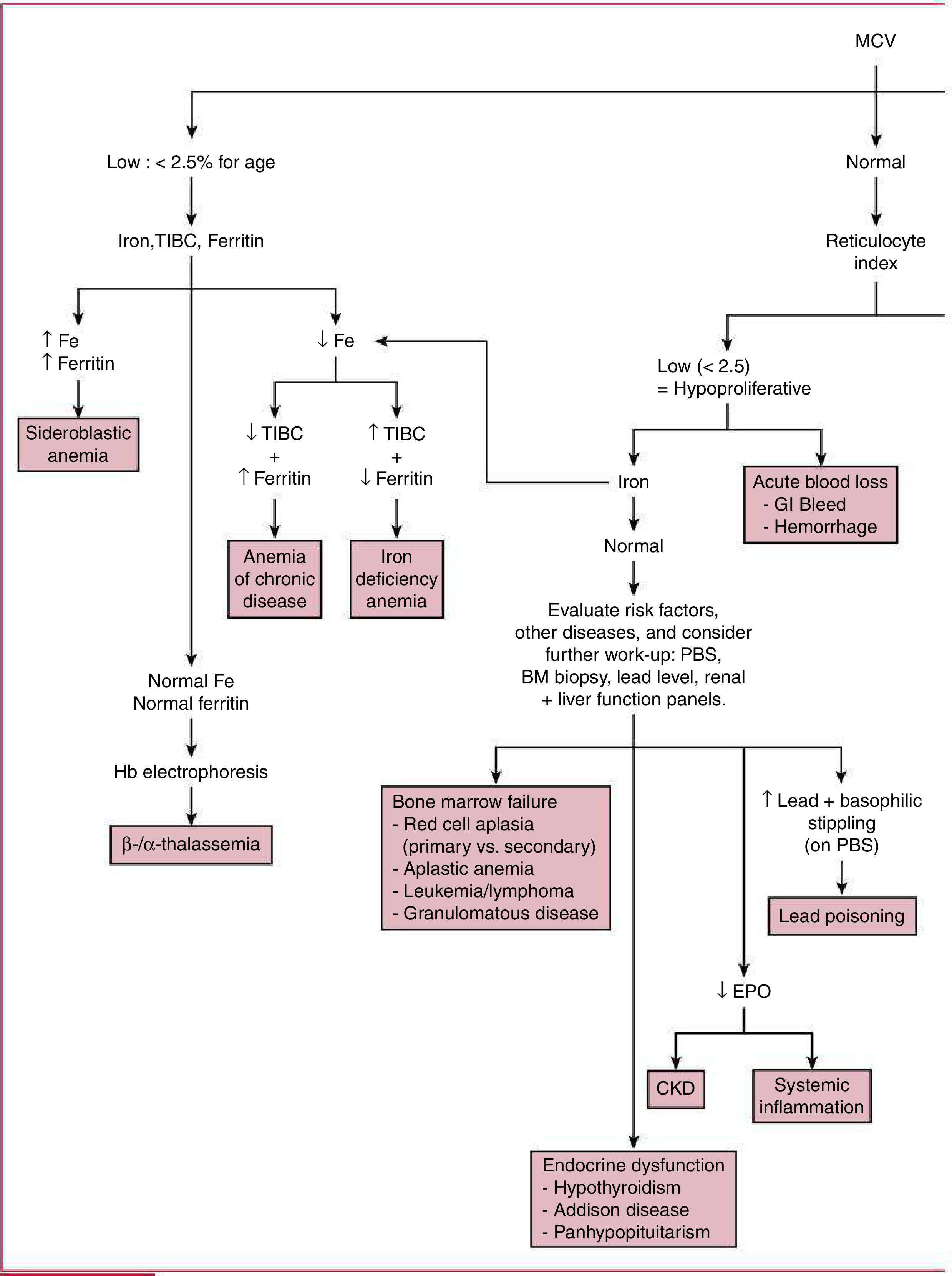
Part A - Low or Normal MCV:
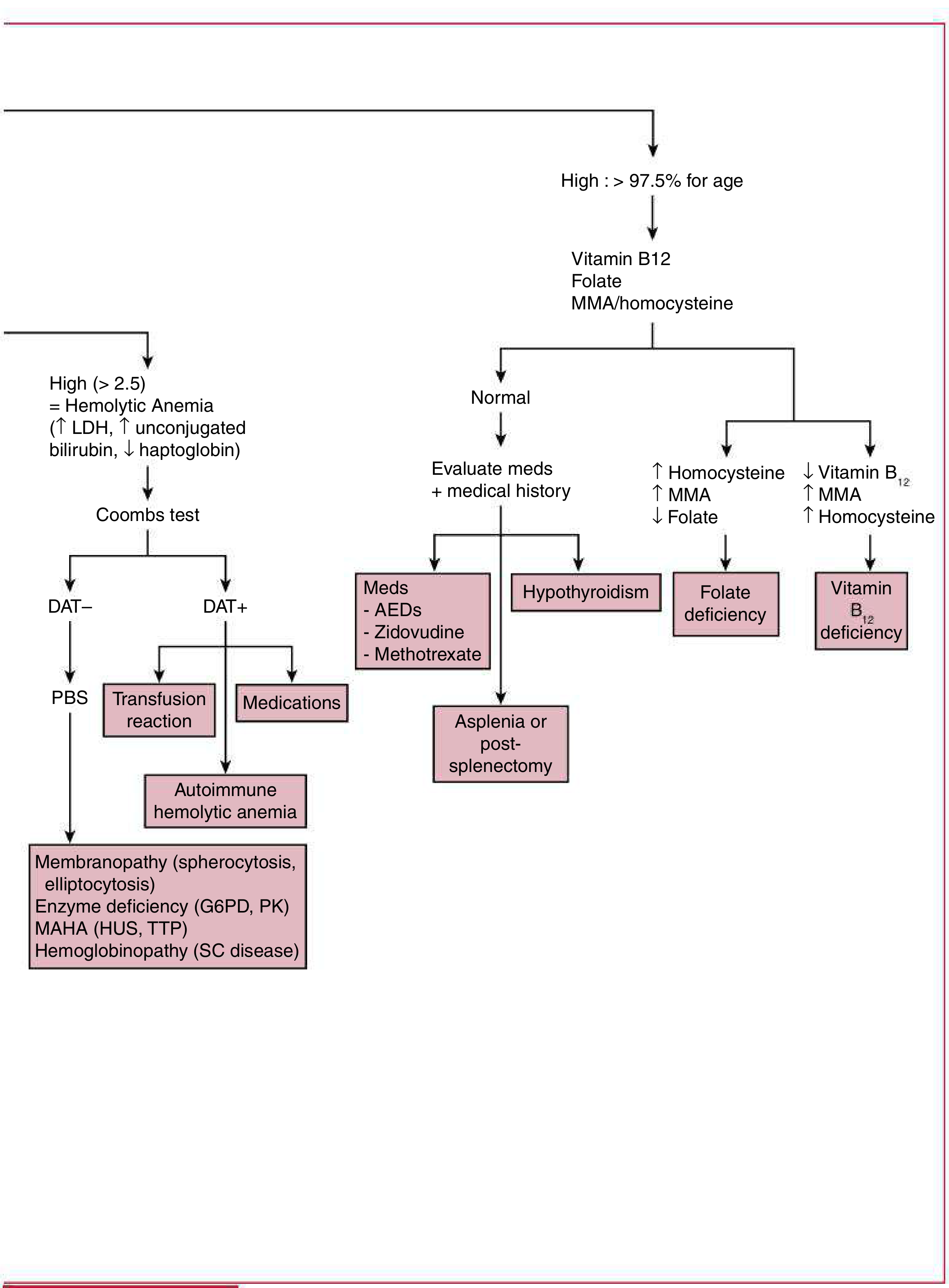
Part B - High MCV and high reticulocyte index:
5. Key Indices and Calculations
| Tool | Formula | Interpretation |
|---|---|---|
| Mentzer Index | MCV / RBC | >13 = IDA; <13 = thalassemia trait |
| RDW | Automated | Normal RDW favors thalassemia; elevated in IDA |
| MCHC | Automated | Low in IDA & thalassemia; elevated + spherocytes = hereditary spherocytosis |
| Serum ferritin | Lab | Reflects total body iron stores (reliable after 6 months of age) |
6. Causes by Category
Non-Hemolytic Anemia
Nutritional:
- Iron deficiency anemia (IDA) - Most common. Causes: poor intake, GI bleed, menstrual losses, malabsorption (celiac, H. pylori, IBD). Ferritin falls first. Low MCHC, elevated transferrin receptor. Usually normocytic; microcytic if severe/prolonged.
- B12 deficiency - Macrocytic; elevated MMA + homocysteine
- Folate deficiency - Macrocytic; elevated homocysteine, normal MMA
Anemia of Chronic Disease:
- Secondary to prolonged/frequent infections, autoimmune conditions (SLE, JIA, IBD), vasculitis
- Labs: low Fe, low TIBC, low transferrin; HIGH ferritin, CRP, ESR
Toxins:
- Lead poisoning - Interferes with iron absorption and inhibits heme synthesis; look for basophilic stippling on PBS
Bone Marrow - Acquired Failure:
- Primary red cell aplasia (autoimmune, autoantibody-mediated)
- Secondary red cell aplasia (parvovirus B19, EBV, CMV, HHV-6, HIV, hepatitis, medications)
- Aplastic anemia (parvovirus, EBV, benzene, alkylating agents, chloramphenicol; hypocellular BM + peripheral cytopenia)
Bone Marrow - Inherited Syndromes:
| Syndrome | Features |
|---|---|
| Diamond-Blackfan anemia | Infants ~3 months; RBC aplasia; congenital anomalies (triphalangeal thumb, short stature, craniofacial) |
| Fanconi anemia | AR/X-linked; pancytopenia, radial/thumb abnormalities, renal anomalies, café-au-lait spots |
| Shwachman-Diamond | AR (SBDS gene); neutropenia ± thrombocytopenia, macrocytic anemia, exocrine pancreatic dysfunction |
| Dyskeratosis congenita | Telomerase mutations; anemia, thrombocytopenia, skin hyperpigmentation, nail dystrophy, oral leukoplakia |
Hemolytic Anemia
When reticulocyte index >2.5 with elevated LDH, unconjugated bilirubin, and low haptoglobin:
Step: Perform Coombs (DAT) test
DAT positive:
- Autoimmune hemolytic anemia
- Transfusion reaction
- Medications
DAT negative (PBS to classify):
- Membranopathy - hereditary spherocytosis, elliptocytosis
- Enzyme deficiency - G6PD, pyruvate kinase (PK) deficiency
- MAHA - HUS, TTP
- Hemoglobinopathy - sickle cell disease
7. Peripheral Blood Smear (PBS) Findings
| Finding | Associations |
|---|---|
| Microcytes | IDA, thalassemia |
| Macrocytes | B12/folate deficiency, reticulocytosis, liver disease |
| Hypochromia | IDA, thalassemia, sideroblastic anemia |
| Spherocytes | Hereditary spherocytosis, autoimmune hemolytic anemia |
| Target cells | Thalassemia, HbC, liver disease |
| Sickle cells | Sickle cell disease |
| Schistocytes | MAHA (HUS, TTP, DIC) |
| Bite cells | G6PD deficiency |
| Basophilic stippling | Lead poisoning, thalassemia |
| Teardrop cells | Myelofibrosis, thalassemia |
| Echinocytes (burr cells) | Uremia, PK deficiency |
8. Management
Iron Deficiency Anemia
- Oral iron (ferrous sulfate): First-line. Empirically treat microcytic anemia with poor dietary iron history.
- Expect reticulocyte rise within 1 week
- Hb increase of 1 g/dL in 4 weeks (if Hb <9 g/dL, response expected in 2 weeks)
- In anemia of chronic disease, only use iron if ferritin <100 ng/mL with evidence of absolute iron deficiency
- IV iron (low-molecular-weight iron dextran or iron sucrose): For malabsorption (PPI use, short bowel syndrome), oral iron intolerance, poor response, or hemodialysis patients on EPO
Sickle Cell Anemia
- Diagnosis often made on newborn screen (Hb electrophoresis)
- Most severe subtypes: HbSS and HbSβ⁰
- Collect baseline labs: CBC, reticulocyte count, Hb electrophoresis (% HbF), renal/liver function, UA, fractionated bilirubin
- RBC exchange transfusion indications: stroke, acute chest syndrome (ACS), multi-organ failure, intrahepatic cholestasis, refractory priapism, prior stroke, or transcranial Doppler >200 cm/sec
- Use HbS-negative cells; keep Hct <30% to avoid hyperviscosity
Summary Algorithm
Pediatric Anemia
└── MCV (age-adjusted)
├── LOW (microcytic)
│ └── Fe, TIBC, Ferritin
│ ├── Low Fe + Low TIBC + High Ferritin → Anemia of Chronic Disease
│ ├── Low Fe + High TIBC + Low Ferritin → Iron Deficiency Anemia
│ └── Normal Fe + Normal Ferritin → Hb Electrophoresis → Thalassemia
│
├── NORMAL (normocytic)
│ └── Reticulocyte Index
│ ├── High (>2.5) = Hemolytic → Coombs test
│ │ ├── DAT+ → Autoimmune / Transfusion Rx / Drugs
│ │ └── DAT- → PBS → Membranopathy / Enzyme deficiency / MAHA / Hemoglobinopathy
│ └── Low (<2.5) = Hypoproliferative
│ ├── Acute blood loss (GI bleed, hemorrhage)
│ ├── Bone marrow failure (aplasia, leukemia, granulomatous disease)
│ ├── Lead poisoning (elevated lead + basophilic stippling on PBS)
│ ├── Low EPO → CKD or Systemic inflammation
│ └── Endocrine (hypothyroidism, Addison disease, panhypopituitarism)
│
└── HIGH (macrocytic)
└── B12, Folate, MMA/Homocysteine
├── Low B12 + High MMA + High homocysteine → B12 deficiency
├── Normal B12 + High homocysteine + Low folate → Folate deficiency
├── Normal → Review meds (AEDs, zidovudine, methotrexate) / hypothyroidism / asplenia
The Harriet Lane Handbook - The Johns Hopkins Hospital, 23rd ed., Chapter 14 (Hematology)
This is a shared conversation. Sign in to Orris to start your own chat.