Causes for finger contracture
Reading File
Finding Sources
Finding Sources
Searching PubMed
finger contracture etiology classification
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
I now have solid textbook content. Let me compile the comprehensive answer.
Causes of Finger Contracture
Finger contractures occur when shortened or fibrosed tissue structures - skin, fascia, tendons, joint capsule, intrinsic muscles, or bone - prevent normal range of motion. They are best understood by anatomical layer and etiology.
I. Fascia / Connective Tissue Causes
Dupuytren's Contracture
The most common cause of progressive finger flexion contracture. It results from proliferation and fibrosis of the palmar fascia, forming a cord that draws the finger into flexion. The ring and little fingers are most commonly affected. Risk factors include Northern European ancestry, male sex, diabetes, epilepsy, alcohol use, and family history. Treatment options include needle aponeurotomy, collagenase injection (Clostridium histolyticum), or open fasciectomy.
- Rosen's Emergency Medicine, p. 3414; Sabiston Textbook of Surgery
II. Ischemia / Compartment Syndrome
Volkmann's Ischemic Contracture
A serious sequela of untreated acute compartment syndrome, classically from a displaced supracondylar fracture of the humerus in children. Ischemia causes necrosis and fibrosis of the forearm flexors, leading to characteristic wrist flexion, finger flexion, and thumb adduction. Three grades:
-
Mild (localized): Partial profundus ischemia; 2-3 fingers involved with flexion contracture
-
Moderate: Long finger flexors + FPL + wrist flexors; intrinsic minus deformity; median/ulnar sensory changes
-
Severe: All forearm flexors and extensors involved; nerves strangulated in fibrotic muscle
-
Campbell's Operative Orthopaedics 15th Ed 2026, p. 4326-4360
III. Causes by Tissue Layer
Based on the PIP joint classification in Campbell's Operative Orthopaedics:
Limited FLEXION (extension contracture):
| Tissue Layer | Cause |
|---|---|
| Skin | Contracture of dorsal skin (scar, burn) |
| Extrinsic tendon | Contracture or adhesion of long extensor |
| Intrinsic muscle | Contracture or adhesion of interosseous muscle |
| Joint | Contracture of capsular/collateral ligaments |
| Bone | Bony block or exostosis |
Limited EXTENSION (flexion contracture):
| Tissue Layer | Cause |
|---|---|
| Skin | Volar skin scarring |
| Fascia | Contracture of superficial fascia (e.g., Dupuytren's) |
| Tendon sheath | Contracture of flexor tendon sheath |
| Tendon/Muscle | Flexor muscle contracture or tendon adhesion |
| Volar plate | Volar plate contracture |
| Ligament | Collateral ligament adhesion in flexed position |
| Bone | Bony block or exostosis |
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 7575-7592
IV. Neurological Causes
Spasticity (Upper Motor Neuron Syndrome)
- Stroke, traumatic brain injury, spinal cord injury, cerebral palsy
- Spastic finger flexors cause flexion contractures due to prolonged abnormal muscle tone
- Common target: wrist and finger flexors post-stroke
Peripheral Nerve Injury
- Ulnar nerve palsy - "Claw hand" (intrinsic minus deformity) - ring and little finger clawing from unopposed extrinsic flexors with loss of intrinsic muscles
- Median nerve palsy - "Ape hand" deformity with thenar wasting; less clawing because FDP to index/middle is also lost
- Combined median + ulnar injury - Severe claw deformity
V. Skin and Soft Tissue Causes
| Cause | Mechanism |
|---|---|
| Burns | Scar contracture, especially over volar or dorsal surface; burn scar syndactyly common |
| Post-traumatic scarring | Crush injuries, lacerations, degloving |
| Infection | Flexor tenosynovitis healing with adhesions |
| Radiation | Skin and soft tissue fibrosis after RT |
VI. Musculoskeletal / Inflammatory Causes
| Cause | Mechanism |
|---|---|
| Rheumatoid arthritis | Synovitis, tendon rupture/adhesion, intrinsic tightness, volar plate laxity (swan neck, boutonniere deformities) |
| Psoriatic arthritis | "Sausage digit," periarticular fibrosis |
| Systemic sclerosis (Scleroderma) | Skin fibrosis causing progressive finger flexion contracture - classic "prayer sign" |
| Trigger finger (stenosing tenosynovitis) | Locked flexion from nodular thickening at A1 pulley |
| Post-fracture/dislocation | Immobilization in poor position, periarticular fibrosis |
| OA | Osteophytes causing bony block |
VII. Congenital Causes
| Condition | Features |
|---|---|
| Camptodactyly | Non-traumatic PIP flexion contracture, usually little finger, onset in childhood |
| Clinodactyly | Angular deviation with bony/soft tissue abnormality |
| Syndactyly | Web space fusion limiting independent motion |
| Arthrogryposis multiplex congenita | Multiple joint contractures from fetal akinesia |
| Trigger thumb/finger (pediatric) | Nodule at A1 pulley |
VIII. Metabolic / Systemic Causes
| Condition | Notes |
|---|---|
| Diabetes mellitus | "Cheiroarthropathy" - progressive painless PIP/MCP stiffness from glycosylation of connective tissue; positive "prayer sign" |
| Hyperparathyroidism | Periarticular calcification |
| Amyloidosis | Infiltration of carpal tunnel and tendon sheaths |
Summary by Deformity Type
| Deformity | Common Causes |
|---|---|
| Flexion contracture | Dupuytren's, Volkmann's, spasticity, volar burn scar, RA, diabetes |
| Extension contracture | Dorsal burn/scar, extensor tendon adhesion, dorsal capsular contracture |
| Claw deformity | Ulnar/median nerve palsy, intrinsic minus state |
| Boutonniere | Central slip injury, RA synovitis |
| Swan neck | Volar plate laxity, intrinsic tightness, FDS rupture |
Depuytrain contracture
Reading File
Finding Sources
Searching PubMed
"Dupuytren contracture"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative textbooks plus recent PubMed meta-analyses. Here is the full answer:
Dupuytren's Contracture
Dupuytren's contracture is a fibroproliferative disorder of the palmar fascia causing progressive flexion deformity of the fingers. First described by Felix Plater in 1614, and later eponymized after Baron Dupuytren who performed an open fasciotomy before a class of students in 1831.
Epidemiology
-
Most common in men aged 50-70 years of Northern European (particularly Scottish, Scandinavian) descent
-
4:1 male-to-female ratio (estrogen may be protective)
-
About 4 out of 7 cases have a positive family history; many are sporadic
-
Bailey and Love's Short Practice of Surgery 28th Ed, p. 3070
Etiology and Risk Factors
| Category | Risk Factor |
|---|---|
| Genetic | Autosomal dominant with variable penetrance; no single gene identified |
| Metabolic | Diabetes mellitus, hypothyroidism, hyperlipidemia |
| Toxic | Alcoholic cirrhosis, smoking |
| Neurological | Epilepsy (especially phenobarbitone use) |
| Other | HIV infection, manual labor/vibration (debated) |
The fibrous nodules are composed of myofibroblasts that express androgen receptors; 5α-dihydrotestosterone drives fibroblast proliferation - this partly explains the male predominance. Unlike deep fibromatoses, Dupuytren's lacks β-catenin and APC gene mutations.
- Andrews' Diseases of the Skin, p. 491; Bailey and Love, p. 3070
Pathology and Pathophysiology
The disease progresses through distinct tissue changes:
- Normal bands - The palmar fascia consists of collagen bundles (longitudinally oriented) between the skin and underlying tendons/neurovascular structures
- Nodule formation - Increased collagen deposition + myofibroblast proliferation creates palpable nodules in the palm (typically proximal to the 4th finger)
- Cord formation - Collagen becomes linearly organized; myofibroblasts cause contraction, forming cords that are the hallmark of symptomatic disease
- Joint contracture - Cords tighten the MCP and PIP joints into fixed flexion
The key pathological cells are myofibroblasts (a hybrid between fibroblasts and smooth muscle cells). TGF-β2 is implicated as a driver of the fibrotic process.
- Schwartz's Principles of Surgery 11th Ed, p. 2946-2948
Clinical Features
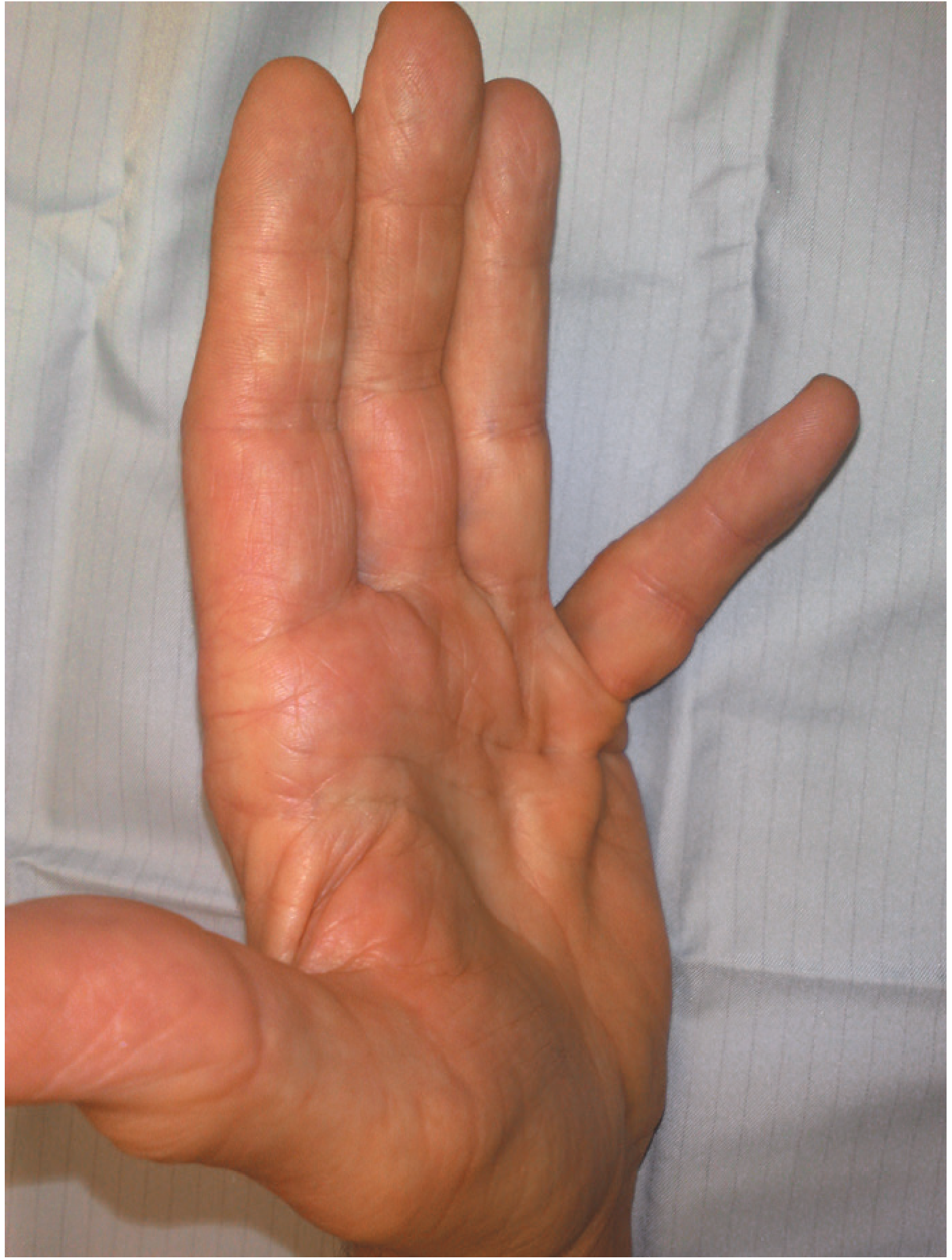
Signs and Symptoms (in order of progression):
- Palmar nodules - firm, non-tender (or mildly tender initially), typically proximal to ring finger
- Skin puckering - dimpling/pitting of the palmar skin (due to skin-fascia attachments)
- Palpable cords - longitudinal fibrous bands in the palm extending into the digits
- Flexion deformity - MCP joint first, then PIP joint; ring > little > middle > index > thumb
- Bilateral in ~45% of cases
Associated Features:
- Garrod's knuckle pads - thickened skin over the dorsal PIP joints (more severe disease)

- Peyronie's disease - fibrous cord in the penis causing curvature (penile Dupuytren's)
- Ledderhose disease - plantar fibromatosis (fibrous nodules on sole of foot)
- Involvement is commonest on the ulnar side of the hand
Indications for Treatment
The classic test is the "table-top test" (Hueston's test):
- Patient places hand flat on a table - if they cannot, intervention is indicated
- Positive = significant contracture requiring treatment
General surgical thresholds:
- MCP contracture ≥ 30°
- PIP contracture ≥ 20°
- Any PIP joint contracture (as PIP corrections are less predictable and worsen with delay)
Treatment
Non-operative (mild/early disease)
| Modality | Notes |
|---|---|
| Observation | Slow progression, no treatment needed for asymptomatic disease |
| Corticosteroid injection | Softens nodules, reduces early discomfort; not effective against cords; does not halt disease progression |
| Splinting | Does NOT retard disease progression (shown in studies) |
Minimally Invasive
| Modality | Notes |
|---|---|
| Needle fasciotomy (percutaneous) | Cord disrupted with a needle; faster recovery; less durable than fasciectomy; best for MCP contractures |
| Collagenase injection (Clostridium histolyticum / Xiaflex) | FDA-approved 2009; enzymatically dissolves cord; good early results; high treatment cost; risk of tendon rupture |
Recent evidence: A 2023 meta-analysis (PMID 37725027) comparing collagenase vs. needle fasciotomy for single-digit Dupuytren's contracture found similar early efficacy, but fasciectomy remains more durable long-term. A 2024 network meta-analysis (PMID 37246411) of surgical approaches supports limited fasciectomy as the standard.
Surgical
| Procedure | Indication |
|---|---|
| Fasciotomy | Division of cord without excision; quicker, more recurrence |
| Limited (partial) fasciectomy | Excision of involved cord only; standard treatment for most cases |
| Radical (total) fasciectomy | Excision of all palmar fascia; higher complication rate, not preferred |
| Dermatofasciectomy | Fascia + overlying skin removed + skin graft; used when skin cannot be separated from cord; lowest recurrence rate |
| Amputation | Reserved for severe, fixed, non-correctable deformity preventing useful hand function |
Skin closure after fasciectomy:
- Z-plasties to lengthen skin
- Full-thickness skin graft (from anteromedial forearm - hairless area)
- Occasionally, open wound healing (McCash technique - open palm technique)
Surgical complications occur in up to 24% of cases:
- Digital nerve laceration (most feared)
- Digital artery injury
- Skin buttonholing / necrosis
- Hematoma
- CRPS (complex regional pain syndrome)
- Recurrence
Postoperative Care
- Hand therapy starts within 1 week of surgery (edema control, early mobilization)
- Extension splinting: 4-6 weeks continuous, then nighttime splinting for 6-8 more weeks
- Serial follow-up for recurrence
Prognosis and Recurrence
- Recurrence is the rule, not the exception - occurs in all forms of treatment
- Needle fasciotomy: highest recurrence (~50% at 5 years)
- Fasciectomy: more durable but recurs in ~20-30% at 5-10 years
- Dermatofasciectomy: lowest recurrence rate
- "Dupuytren's diathesis" (young age of onset, bilateral disease, knuckle pads, Peyronie's, family history) = higher recurrence risk
Summary Box (Bailey and Love)
- Autosomal dominant inheritance, many sporadic cases
- Fibroblastic hyperplasia → palmar nodules → cords → fixed flexion deformity
- Intervention indicated when hand cannot be placed flat on a table
- Severe fixed deformity at PIP joint may ultimately require amputation
Sources: Bailey and Love's Short Practice of Surgery 28th Ed, p. 3070-3124; Schwartz's Principles of Surgery 11th Ed, p. 2944-2962; Andrews' Diseases of the Skin, p. 491-493
This is a shared conversation. Sign in to Orris to start your own chat.