Q. Surgeries for Meniere's disease in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
Meniere disease surgery endolymphatic sac decompression shunt labyrinthectomy vestibular nerve section diagram
Reading File
Loading Image
Reading File
I now have comprehensive information from Cummings. Let me compile the complete answer.
Surgical Management of Ménière's Disease
(50-Mark Answer — RGUHS Standard)
INTRODUCTION
Ménière's disease (MD) is a disorder of the membranous labyrinth characterized by the clinical tetrad of:
- Episodic vertigo (30 min – several hours)
- Fluctuating sensorineural hearing loss (low-frequency, initially)
- Tinnitus
- Aural fullness
The underlying pathology is endolymphatic hydrops — distension of the endolymphatic compartment of the membranous labyrinth. About 85% of cases are unilateral; bilateral involvement, when it occurs, usually manifests within 36 months of the first ear.
"Because the stage at which a spontaneous remission occurs cannot be predicted, several medical and surgical therapies have evolved to alter the natural history. The surgical therapies are either destructive, or preservative of residual hearing." — KJ Lee's Essential Otolaryngology
INDICATIONS FOR SURGERY
Surgery is considered when:
- Medical management has failed after 6–12 months
- Patient has disabling vertigo affecting quality of life
- Attacks are frequent and severe (≥3 definitive attacks/6 months despite treatment)
- Medical: low-salt diet, diuretics, vestibular suppressants, betahistine have failed
- Before ablative surgery — intratympanic gentamicin (chemical ablation) is usually tried
CLASSIFICATION OF SURGICAL PROCEDURES
╔══════════════════════════════════════════════════════════════╗
║ SURGERIES FOR MÉNIÈRE'S DISEASE ║
╠══════════════════════╦═══════════════════════════════════════╣
║ CONSERVATIVE ║ ABLATIVE / DESTRUCTIVE ║
║ (Hearing Preserving)║ ║
╠══════════════════════╬═══════════════════════════════════════╣
║ 1. Endolymphatic ║ A. CHEMICAL ABLATION ║
║ Sac Surgery: ║ • Intratympanic Gentamicin ║
║ a) Decompression ║ (IT Aminoglycoside) ║
║ b) Shunts ║ B. SURGICAL ABLATION ║
║ (mastoid, ║ • Cochleosacculotomy ║
║ subarachnoid)║ • Labyrinthectomy: ║
║ 2. Cochleosacculotomy║ – Transcanal (Cody tack) ║
║ (elderly/poor ║ – Transmastoid ║
║ hearing) ║ – Translabyrinthine ║
║ 3. Vestibular ║ C. NEURECTOMY ║
║ Neurectomy ║ • Vestibular Nerve Section: ║
║ (hearing present)║ – Middle fossa approach ║
║ ║ – Retrolabyrinthine ║
║ ║ – Retrosigmoid/posterior fossa ║
╚══════════════════════╩═══════════════════════════════════════╝
PREOPERATIVE EVALUATION
Before ANY vestibular surgery (Cummings):
- Audiometry — establishes hearing level, identifies pathologic ear
- Electronystagmography (ENG)/Videonystagmography (VNG) — caloric testing, identifies side
- Electrocochleography (ECochG) — elevated summating potential/action potential ratio (>0.35) supports hydrops
- MRI of posterior fossa with gadolinium — mandatory to exclude acoustic neuroma, demyelinating disease, brainstem ischemia
- Glycerol dehydration test — improvement in PTA >10 dB or speech discrimination >12% confirms hydrops
- Identification of the offending labyrinth:
- Most reliable: fluctuating/progressive unilateral SNHL
- Reproducible unilateral caloric reduction
- Asymmetric hearing loss = best indicator
"If uncertainty arises regarding the ear causing vertigo, ablative surgery should not be considered." — Cummings Otolaryngology
FLOWCHART: MANAGEMENT ALGORITHM FOR MÉNIÈRE'S DISEASE
MÉNIÈRE'S DISEASE
│
┌─────────▼──────────┐
│ MEDICAL MANAGEMENT│
│ • Low-salt diet │
│ • Diuretics │
│ • Betahistine │
│ • Vestibular │
│ suppressants │
└─────────┬──────────┘
│
┌───────────▼────────────────────┐
│ Controlled? YES → Continue Rx │
└───────────┬────────────────────┘
│ NO (>6–12 months failure)
▼
┌───────────────────────────────┐
│ INTRATYMPANIC GENTAMICIN │
│ (Chemical Labyrinthectomy) │
└───────────┬───────────────────┘
│
┌───────────▼──────────────────┐
│ ASSESS RESIDUAL HEARING │
└──────┬────────────────────┬──┘
│ │
┌──────▼──────┐ ┌──────▼──────┐
│ USEFUL │ │ NO USEFUL │
│ HEARING │ │ HEARING │
│ PRESENT │ │ (PTA>60dB) │
└──────┬──────┘ └──────┬──────┘
│ │
┌─────────────┼──────────┐ ┌─────▼──────────────┐
▼ ▼ ▼ │ LABYRINTHECTOMY │
Endolymphatic Vestibular IT Steroids │ (Transmastoid or │
Sac Surgery Neurectomy (adjunct) │ Translabyrinthine)│
(MFC/retro Cochleosac- └────────────────────┘
labyrinthine) culotomy
Retrosigmoid (elderly)
A. CONSERVATIVE (HEARING-PRESERVING) PROCEDURES
1. ENDOLYMPHATIC SAC SURGERY
Anatomy of the Endolymphatic Sac
- The endolymphatic sac (ES) is a blind-ending epithelial sac located in the posterior cranial fossa, between layers of the dura mater near the sigmoid sinus
- It lies in the Trautmann's triangle (bounded by sigmoid sinus posteriorly, posterior semicircular canal anteriorly, superior petrosal sinus superiorly)
- The endolymphatic duct connects the saccule and utricle to the sac via the vestibular aqueduct
Rationale
The ES is responsible for endolymph resorption. In Ménière's disease, impaired resorption leads to endolymphatic hydrops. Surgery on the ES aims to:
- Decompress the sac (reduce pressure)
- Create a drainage pathway (shunt)
Types of Endolymphatic Sac Procedures
a) Endolymphatic Sac Decompression (ESD)
Technique:
- Mastoidectomy — complete simple mastoidectomy performed
- The sigmoid sinus and posterior semicircular canal are skeletonized
- Bone over the posterior fossa dura is removed in Trautmann's triangle
- The endolymphatic sac is identified as a thickened white structure in the posterior fossa dura
- The sac is exposed but the lumen is not opened
- Removal of the bone overlying the sac reduces pressure
Landmarks used to identify ES:
- Bill's island: a knob of bone between the posterior semicircular canal and the sigmoid sinus
- Donaldson's line: a line drawn through the horizontal semicircular canal, parallel to the lateral semicircular canal — the ES lies below this line
b) Endolymphatic Sac Drainage/Shunts
Several types based on drainage site:
- Endolymphatic-mastoid shunt: Sac is opened and a T-tube/silastic tube placed from the sac lumen into the mastoid cavity
- Endolymphatic-subarachnoid shunt: Tube drains into the posterior cranial fossa CSF — higher rates of CSF leak, meningitis; largely abandoned
- Summerskill's procedure (endolymphatic sac incision): Simple incision of the sac
Results (Cummings):
- Vertigo control in 60–80% at 2 years
- Hearing preservation in most
- Controversy: The classic Thomsen et al. double-blind placebo-controlled study (Denmark) showed endolymphatic sac shunt surgery was no better than mastoidectomy alone (placebo effect of surgery), calling the procedure's specific efficacy into question
- Despite controversy, ESD remains widely practiced as it is the least invasive surgical option and has a low complication rate
2. COCHLEOSACCULOTOMY (FICK OPERATION)
Indication: Elderly patients with disabling vertigo, poor hearing (non-serviceable), significant residual vestibular function, and who are poor candidates for general anesthesia — can be performed under local anesthesia
Technique (KJ Lee):
- A pick (Fick's pick) is introduced through the round window membrane into the scala tympani
- The instrument is advanced to perforate the basilar membrane and then the saccular wall (Reissner's membrane area), creating a communication between endolymph and perilymph
- This allows decompression of the endolymphatic space
Results:
- Vertigo control: ~70%
- Risk: further deterioration of already poor hearing
- Crude but effective under local anesthesia in elderly patients
B. ABLATIVE PROCEDURES — LABYRINTHECTOMY
Indication: Patients with:
- Non-serviceable hearing (PTA >60–70 dB or speech discrimination <50%)
- Unilateral MD with intractable vertigo
- Older patients with poor hearing
"Both labyrinthectomy and vestibular nerve section abolish rotary vertigo in >90% of cases." — Harrison's Principles of Internal Medicine
TYPES OF LABYRINTHECTOMY
a) Transcanal (Oval Window) Labyrinthectomy
- Performed through the external auditory canal
- Stapes removed, perilymph aspirated
- Neuroepithelium of the semicircular canals and saccule curetted out
- Simpler but limited access
b) Transmastoid Labyrinthectomy
Technique:
- Complete mastoidectomy performed
- Incus removed for improved access
- All three semicircular canals are opened and the membranous labyrinth drilled out
- Utricle and saccule are removed
- Vestibular end organs are completely ablated
- Cochlea may be preserved (cochlea is not drilled)
- Fat obliteration of the cavity optional
Advantages:
- Better access than transcanal
- Can be combined with cochlear implantation (simultaneous labyrinthectomy + CI)
- Lower morbidity than translabyrinthine approach
c) Translabyrinthine Labyrinthectomy
- Used primarily when an acoustic neuroma co-exists
- Provides wide posterior fossa access
- Complete labyrinth sacrificed including cochlea and vestibule
- Used rarely for MD alone; more for vestibular schwannoma
Results of Labyrinthectomy:
- Vertigo control: 95–98% (best control of all surgical options)
- Hearing: sacrificed completely
- Facial nerve: at risk if anatomy is distorted (must be identified)
- Requires central vestibular compensation postoperatively — rehabilitation needed
C. VESTIBULAR NEURECTOMY (VESTIBULAR NERVE SECTION)
The gold standard hearing-preserving ablative procedure for Ménière's disease
Rationale: Selective section of the superior and inferior vestibular nerves while preserving the cochlear nerve → eliminates vestibular input from the pathologic ear while preserving hearing
Indication:
- Intractable MD with serviceable hearing (PTA <50 dB, speech discrimination >50%)
- Failed endolymphatic sac surgery
- Failed intratympanic gentamicin
- Bilateral vestibular dysfunction excluded
Surgical Approaches to Vestibular Neurectomy
a) Retrolabyrinthine Vestibular Neurectomy
- Developed by Silverstein and Norrell
- Mastoidectomy → bone posterior to posterior semicircular canal removed → posterior fossa dura opened posterior to the labyrinth
- Vestibular nerve section performed in the posterior cranial fossa just medial to the internal auditory canal (IAC)
- Cochlear and facial nerves identified and preserved
- Advantage: Less cerebellar retraction, lower CSF leak risk
- Disadvantage: Restricted access, challenging visualization of nerve branches
b) Middle Cranial Fossa (Middle Fossa) Vestibular Neurectomy
- Developed by House; indicated especially for selective superior vestibular neurectomy
- Temporal craniotomy above the zygomatic arch → extradural elevation of temporal lobe
- IAC identified from above
- Superior vestibular nerve selectively sectioned (posterior ampullary nerve and main superior division)
- Advantage: Excellent exposure of superior vestibular nerve; cochlear nerve easily identified and preserved
- Disadvantage: Risk of temporal lobe retraction injury, epidural hematoma; technically demanding; not suitable for elderly/poor surgical candidates
c) Retrosigmoid (Posterior Fossa) Vestibular Neurectomy
- Retrosigmoid/suboccipital craniectomy → posterior cranial fossa
- Internal auditory canal drilled open from posterior
- Vestibular nerve branches sectioned under direct vision
- Advantage: Wide exposure, good visualization of all nerve divisions, suitable for all age groups
- Disadvantage: Higher rate of postoperative headache; cerebellar retraction needed; CSF leak risk
Nerve Identification During Neurectomy
In the IAC (from superior to inferior):
┌─────────────────────────────────┐
│ Superior Vestibular Nerve │ ← SECTION
│ (Facial nerve anterior to it) │
├─────────────────────────────────┤
│ Inferior Vestibular Nerve │ ← SECTION
├─────────────────────────────────┤
│ Cochlear Nerve │ ← PRESERVE
├─────────────────────────────────┤
│ Facial Nerve (anterior-superior)│ ← PRESERVE
└─────────────────────────────────┘
Bill's bar separates facial nerve
from superior vestibular nerve
Results of Vestibular Neurectomy (Cummings):
- Vertigo control: 90–95%
- Hearing preservation: 60–85% depending on approach
- Facial nerve injury: <1–2% in experienced hands
- CSF leak: 2–5%
D. INTRATYMPANIC AMINOGLYCOSIDE ABLATION (CHEMICAL LABYRINTHECTOMY)
While not strictly "open surgery," this is a procedural ablative therapy important for RGUHS exams:
-
Intratympanic gentamicin (IT Gentamicin):
- Gentamicin is specifically vestibulotoxic at low doses (spares cochlear hair cells at lower concentrations vs. streptomycin which is more cochleotoxic)
- Administered via myringotomy and injection into the middle ear, diffuses through the round window
- Multiple dosing protocols: weekly injections (titration protocol) vs. fixed-dose
- Vertigo control: 80–90%; risk of additional SNHL: 10–30% (dose-dependent)
- Currently considered first-line ablative therapy before open surgical ablation (Cummings)
-
Intratympanic streptomycin: More cochleotoxic; used historically for bilateral MD
E. INTRATYMPANIC STEROIDS (NON-ABLATIVE)
- Dexamethasone or methylprednisolone injected intratympanically
- Mechanism: anti-inflammatory, mineralocorticoid effects on Na⁺-K⁺ channels in endolymph homeostasis
- Itoh & Sakata (1987): first IT steroid protocol — 4–5 weekly 2 mg dexamethasone injections → vertigo relief in 80%, tinnitus reduction in 74%
- Advantage: No ablative risk, reversible
- Limitation: No effect on hearing; efficacy uncertain in RCTs
COMPARATIVE SUMMARY TABLE
| Procedure | Hearing | Vertigo Control | Approach | Indication |
|---|---|---|---|---|
| Endolymphatic Sac Decompression | Preserved | 60–80% | Mastoid | All stages; first surgical option |
| Endolymphatic Sac Shunt | Preserved | 65–75% | Mastoid | Failed conservative Rx |
| Cochleosacculotomy | Poor (already) | ~70% | Transcanal | Elderly, local anesthesia, poor hearing |
| IT Gentamicin | Usually preserved | 80–90% | Tympanic injection | Before open ablative surgery |
| Transmastoid Labyrinthectomy | Sacrificed | 95–98% | Mastoid | Non-serviceable hearing, intractable vertigo |
| Retrolabyrinthine Neurectomy | Preserved | 90–95% | Mastoid + posterior fossa | Serviceable hearing, failed conservative |
| Middle Fossa Neurectomy | Preserved | 90–95% | Cranial (middle fossa) | Serviceable hearing, younger patients |
| Retrosigmoid Neurectomy | Preserved | 90–95% | Posterior cranial fossa | Serviceable hearing, all age groups |
DECISION-MAKING FLOWCHART (HEARING-BASED)
INTRACTABLE MÉNIÈRE'S DISEASE
(Failed Medical + IT Gentamicin)
│
┌─────────▼──────────┐
│ ASSESS HEARING │
└─────┬──────────┬───┘
│ │
┌─────▼────┐ ┌──▼──────────────┐
│SERVICEABLE│ │NON-SERVICEABLE │
│ HEARING │ │ HEARING │
│PTA <50 dB│ │PTA >60 dB or │
│SD >50% │ │SD <50% │
└─────┬────┘ └──┬──────────────┘
│ │
┌─────▼────┐ ┌──▼──────────────┐
│Endolymph-│ │ LABYRINTHECTOMY │
│atic Sac │ │ (Transmastoid) │
│Surgery │ │ Vertigo control │
│(1st line)│ │ 95–98% │
└─────┬────┘ └─────────────────┘
│
┌─────▼────────────────┐
│ Failed ELS surgery? │
└─────┬────────────────┘
│ YES
┌─────▼────────────────────────────┐
│ VESTIBULAR NEURECTOMY │
│ Choose approach: │
│ • Young/fit → Middle fossa │
│ • General → Retrosigmoid │
│ • Less invasive → Retrolabyrinth │
└──────────────────────────────────┘
ENDOLYMPHATIC SAC — SURGICAL ANATOMY DIAGRAM
TEMPORAL BONE (POSTERIOR VIEW)
Superior Petrosal Sinus ────────────────┐
│
Posterior Semicircular Canal ─┐ │
│ │
TRAUTMANN'S TRIANGLE │ │
(Site of Endolymphatic Sac) │ │
┌──────────────────────┐ │
│ ENDOLYMPHATIC SAC │ │
│ (in dura mater) │ │
└──────────────────────┘ │
│ │
Sigmoid Sinus ────────────────┘─────────┘
Jugular Bulb ────── inferior boundary
DONALDSON'S LINE: parallel to lateral SCC
→ ES lies BELOW this line
BILL'S ISLAND: bony knob between
posterior SCC and sigmoid sinus
→ ES lies MEDIAL to this landmark
MRI IMAGE: Endolymphatic Hydrops — Pre and Post Surgery
MRI of inner ear showing endolymphatic hydrops in Ménière's disease:
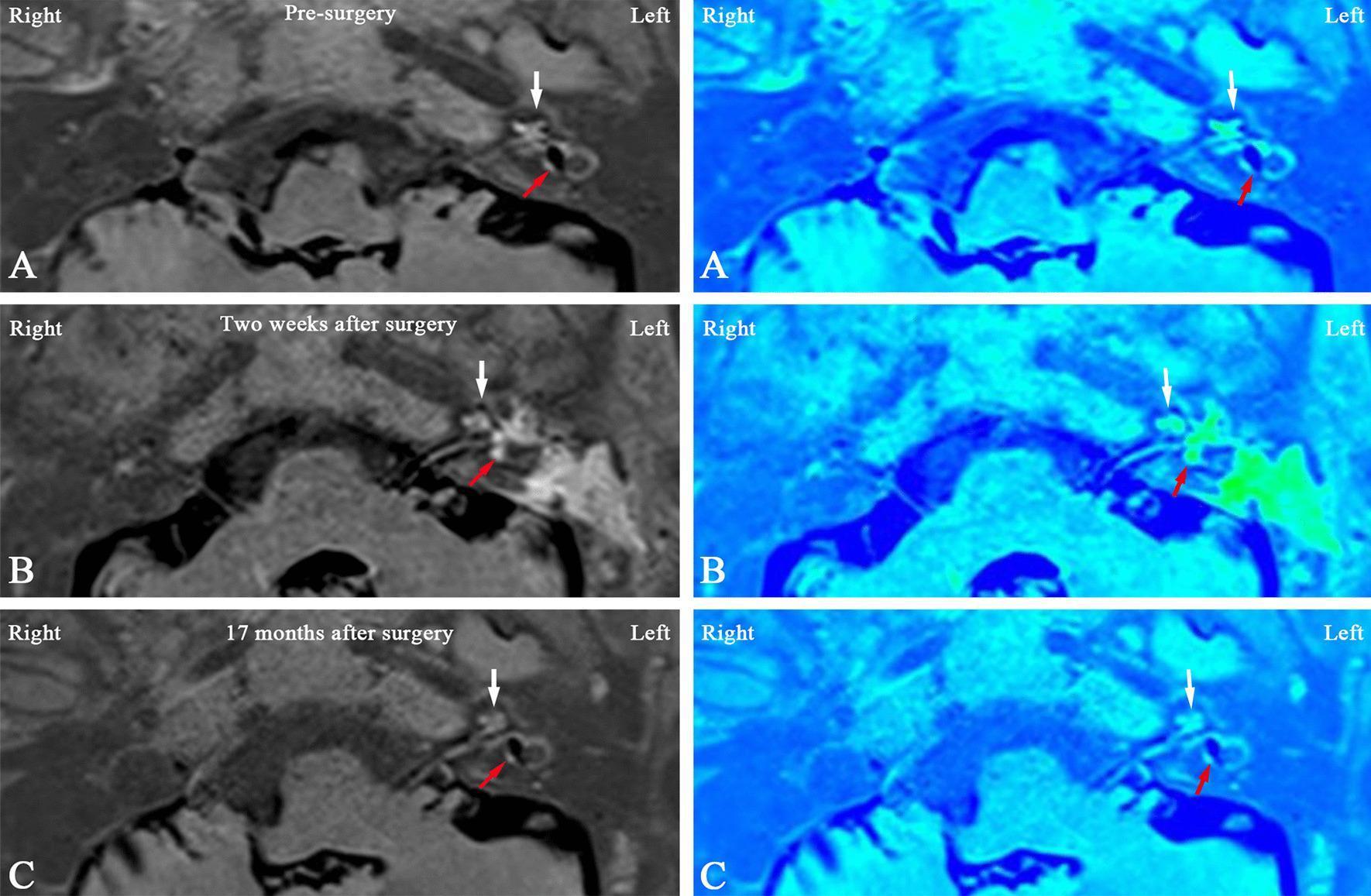
Pre-surgery (A): significant vestibular and cochlear hydrops (expanded blue endolymphatic compartment). Post-surgery at 2 weeks (B): complete reversal of both cochlear and vestibular hydrops. 17-month follow-up (C): stable cochlear hydrops reversal with recurrence of vestibular hydrops — illustrating the dynamic nature of endolymphatic fluid post-surgery.
RECENT ADVANCES (2018–2024)
-
MRI Endolymphatic Hydrops Grading (Intravenous Gadolinium MRI)
- 3D real inversion recovery (3D-real IR) sequences after delayed IV or IT gadolinium
- Allows non-invasive visualization and grading of hydrops (cochlear and vestibular compartments)
- Guides surgical decision-making and monitors post-surgical outcomes
- Vestibular Hydrops Ratio (VHR) measured quantitatively
-
Minimally Invasive Endolymphatic Sac Surgery
- Endoscope-assisted ESD — reduced retraction, better visualization without full mastoidectomy
- Transmastoid approaches refined with image-guided navigation
-
Cochlear Implantation + Simultaneous Labyrinthectomy
- For patients with end-stage bilateral MD or unilateral MD with profound SNHL
- Labyrinthectomy performed simultaneously with CI insertion
- Provides both vestibular control AND auditory rehabilitation in a single procedure (Alarcon et al., 2017)
-
IT Gentamicin — Low-Dose Titration Protocols
- "On-demand" or symptom-triggered protocols
- Single low-dose injections with re-treatment only if vertigo recurs
- Reduces risk of hearing loss (Kaylie et al., 2020)
-
Endolymphatic Sac Electrocautery
- Electrosurgical enhancement of ES decompression using bipolar cautery to create fibrous adhesions
- Preliminary results show improved vertigo control vs. decompression alone
-
Pressure Therapy: Meniett Device
- Non-surgical: applies micropressure pulses via tympanostomy tube
- Thought to facilitate endolymph resorption via pressure transmission
- FDA-approved; used as bridge between medical and surgical therapy
-
Gene Therapy (Experimental)
- Aquaporin-2 and Aquaporin-4 channels regulate endolymph homeostasis
- Gene modulation to normalize fluid transport — animal models promising
- Human trials pending
-
Vestibular Implants (Research Stage)
- Analog of cochlear implant for vestibular system
- Stimulates vestibular nerve electrically after labyrinthectomy
- Potential future application in bilateral MD
COMPLICATIONS OF SURGERY
| Surgery | Specific Complications |
|---|---|
| Endolymphatic Sac Surgery | CSF leak, meningitis, sigmoid sinus injury, failure, sensorineural hearing loss |
| Labyrinthectomy | Facial nerve injury, CSF leak, recurrent vertigo (rare, if neuroepithelium incomplete), perilymph fistula |
| Vestibular Neurectomy | Facial nerve injury (most feared), CSF leak, meningitis, hearing loss, headache (retrosigmoid), temporal lobe contusion (middle fossa) |
| IT Gentamicin | Sensorineural hearing loss (10–30%), incomplete ablation requiring repeat |
IMPORTANT HISTORICAL CONTRIBUTIONS
| Surgeon | Contribution |
|---|---|
| Ménière (1861) | First described the syndrome; attributed it to labyrinthine pathology |
| Portmann (1927) | First endolymphatic sac drainage operation |
| Shambaugh (1966) | Popularized endolymphatic sac decompression |
| House (1962) | Developed middle cranial fossa approach for vestibular neurectomy |
| Silverstein & Norrell | Retrolabyrinthine vestibular neurectomy |
| Fick (1964) | Cochleosacculotomy (Fick operation) |
| Schuknecht | Cody tack procedure; temporal bone studies on hydrops |
| Thomsen et al. | Landmark placebo-controlled trial questioning ELS shunt efficacy |
| Itoh & Sakata (1987) | First IT steroid protocol |
SUMMARY MNEMONICS
Surgical options — "CLEVER":
- C — Cochleosacculotomy (elderly, local anesthesia)
- L — Labyrinthectomy (no useful hearing)
- E — Endolymphatic sac surgery (first line, hearing present)
- V — Vestibular neurectomy (hearing present, failed ELS)
- E — Electrolytic/chemical ablation (IT gentamicin)
- R — Retrolabyrinthine/Retrosigmoid/middle fossa (approaches for neurectomy)
REFERENCES (Textbook Sources)
- Cummings Otolaryngology — Head and Neck Surgery (7th ed., Flint et al.) — Chapters 158 (Intratympanic Drug Therapy) and 165 (Surgical Management of Vestibular Disorders), pp. 3034–3260
- KJ Lee's Essential Otolaryngology (11th ed.) — Ménière Disease, pp. 76–77
- Scott-Brown's Otolaryngology, Head and Neck Surgery — Ménière disease management (standard reference per RGUHS syllabus)
- Dhingra's Diseases of Ear, Nose and Throat — Meniere's disease and surgical management
- Hazarika's Textbook of ENT and Head Neck Surgery — Meniere's disease surgery
- Harrison's Principles of Internal Medicine (22nd ed.) — Sensorineural Hearing Loss and Vertigo chapter: "Surgical therapy of vertigo is reserved for unresponsive cases and includes endolymphatic sac decompression, labyrinthectomy, and vestibular nerve section. Both labyrinthectomy and vestibular nerve section abolish rotary vertigo in >90% of cases."
Note on generate_image: The image generation feature is currently unavailable on your plan (monthly limit reached). The flowcharts and anatomical diagrams above are rendered as detailed ASCII/text diagrams. To upgrade for image generation, please contact support or upgrade your subscription plan.
This is a shared conversation. Sign in to Orris to start your own chat.