Tympanoplasty in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
tympanoplasty surgical technique graft placement diagram
Reading File
Searching Images
Wullstein classification tympanoplasty types ossiculoplasty
Note on image generation: Thegenerate_imagetool has reached its monthly plan limit. The flowcharts below are rendered as detailed ASCII/text diagrams. Please upgrade your subscription plan for image generation, or contact support if you believe this is an error.
TYMPANOPLASTY
A Comprehensive 50-Mark Answer
Sources: Cummings Otolaryngology (6th ed.), K.J. Lee's Essential Otolaryngology, Scott-Brown's Otorhinolaryngology, Dhingra's Diseases of Ear Nose & Throat, Stell & Maran's Head and Neck Surgery, Hazarika's Textbook of ENT & Head-Neck Surgery, Zakir Hussain's ENT
1. DEFINITION
Tympanoplasty is a surgical procedure performed to:
- Eradicate infection and middle ear pathology
- Reconstruct the tympanic membrane (TM)
- Reestablish a durable connection between the TM and the inner ear
- Restore hearing by rebuilding the middle ear transformer mechanism
The term was coined by Wullstein (1952) and Zöllner (1955), who independently described techniques for middle ear reconstruction.
2. HISTORICAL BACKGROUND
| Year | Contributor | Contribution |
|---|---|---|
| 1952 | Wullstein | Introduced classification of tympanoplasty (Types I–V) |
| 1955 | Zöllner | Described ossicular chain reconstruction |
| 1956 | House | Introduced operating microscope |
| 1960 | Shea | Stapedectomy technique |
| 1961 | Storrs | Introduced temporalis fascia as graft |
| 1990s | Tos, Duckert | Cartilage tympanoplasty popularized |
| 2010s | Tarabichi | Endoscopic ear surgery advances |
3. ANATOMY RELEVANT TO TYMPANOPLASTY
Tympanic Membrane Layers:
- Outer epithelial layer — stratified squamous epithelium (migrates centrifugally)
- Middle fibrous layer — radial and circular fibres (pars tensa); absent in pars flaccida
- Inner mucosal layer — ciliated columnar epithelium
Ossicular Chain:
- Malleus (handle/manubrium attached to TM)
- Incus (lenticular process articulates with stapes)
- Stapes (footplate in oval window)
Middle Ear Transformer Mechanism:
The middle ear amplifies sound via:
- Hydraulic ratio (TM: oval window = 17:1) — most important
- Curved membrane effect (2:1 ratio)
- Ossicular lever ratio (1.3:1)
Total gain ≈ 17 × 2 × 1.3 = ~44:1 ≈ 25–30 dB — Cummings Otolaryngology
4. WULLSTEIN'S CLASSIFICATION OF TYMPANOPLASTY
(Wullstein, 1952 — cited in Dhingra, Cummings, Zakir Hussain)
┌─────────────────────────────────────────────────────────────────────────┐
│ WULLSTEIN'S CLASSIFICATION │
├──────────┬───────────────────────────────────────────────────────────────┤
│ TYPE I │ Myringoplasty only. Ossicular chain intact and mobile. │
│ │ Graft placed to close TM perforation. │
├──────────┼───────────────────────────────────────────────────────────────┤
│ TYPE II │ TM graft onto malleus/incus after incus erosion. │
│ │ Graft rests on remaining long process of incus or malleus. │
├──────────┼───────────────────────────────────────────────────────────────┤
│ TYPE III│ Myringostapediopexy. │
│ │ TM graft placed directly on stapes head │
│ │ (incus and malleus absent). MOST COMMON in practice. │
├──────────┼───────────────────────────────────────────────────────────────┤
│ TYPE IV │ TM graft placed over an intact mobile footplate. │
│ │ Round window protected. Only footplate remains. │
├──────────┼───────────────────────────────────────────────────────────────┤
│ TYPE V │ Fenestration of horizontal semicircular canal. │
│ │ Used when footplate is fixed. (Largely obsolete) │
└──────────┴───────────────────────────────────────────────────────────────┘
"The basic principles behind this classification still hold true today, but the practice of tympanoplasty has been modified by advances in the fields of optics, microsurgical instrumentation, middle ear prostheses, and surgical techniques." — Cummings Otolaryngology
5. INDICATIONS AND CONTRAINDICATIONS
INDICATIONS:
- Chronic suppurative otitis media (CSOM) — tubotympanic (safe) type
- Traumatic perforation of TM (after 3–6 months observation)
- Dry central perforation with conductive hearing loss
- Atelectatic ear (collapsed TM) with hearing loss
- Failed previous repair
CONTRAINDICATIONS:
┌────────────────────────────────────────────────────────┐
│ CONTRAINDICATIONS │
├─────────────────────┬──────────────────────────────────┤
│ ABSOLUTE │ RELATIVE │
├─────────────────────┼──────────────────────────────────┤
│ Only hearing ear │ Active ear discharge │
│ (relative) │ (operate after 6-8 wks dry) │
│ Cholesteatoma │ Poor Eustachian tube function │
│ (mastoidectomy │ Children <7 years (ET immature) │
│ first) │ Contralateral ear disease │
│ Active mastoid │ Systemic illness / poor health │
│ disease │ Keloid formers │
└─────────────────────┴──────────────────────────────────┘
— Dhingra's Diseases of ENT, Hazarika
6. PREOPERATIVE ASSESSMENT
Clinical:
- Complete ENT examination
- Otoscopy / otoendoscopy — size/site of perforation, status of ossicles
- Eustachian tube function tests (Valsalva, politzerization, Toynbee test)
- Assess opposite ear
Audiological:
- Pure Tone Audiogram (PTA) — air-bone gap (ABG)
- Impedance audiometry (tympanometry)
- Speech discrimination scores
Radiological:
- HRCT temporal bone (if cholesteatoma suspected, ossicular status uncertain, or revision)
Systemic:
- Routine blood investigations
- Assess fitness for general anaesthesia
7. PREOPERATIVE WORKUP FLOWCHART
PATIENT WITH TM PERFORATION
│
┌────────────────┴────────────────┐
│ │
Dry Ear >6 weeks Wet / discharging
│ │
Audiometry + Treat with topical/
HRCT Temporal Bone systemic antibiotics
│ │
Eustachian Tube Dry ear achieved?
Function Test │
│ ┌────┴────┐
Assess ossicular YES NO
status │ │
│ Proceed to Continue
Counselling + surgery management /
Informed consent consider
│ mastoidectomy
TYMPANOPLASTY
8. GRAFT MATERIALS
(Dhingra, Cummings, Scott-Brown)
8A. Autografts (Preferred):
| Graft | Source | Advantages | Disadvantages |
|---|---|---|---|
| Temporalis fascia | Temporalis muscle | Most common, excellent results | Requires separate incision, can atrophy |
| Tragal perichondrium | Tragal cartilage | No separate incision, good vibratory properties | Limited quantity |
| Conchal perichondrium | Concha of pinna | Good size | Thick |
| Tragal cartilage | Tragus | Rigid, resists retraction, ETD-resistant | Stiffness may affect hearing at high freq. |
| Conchal cartilage | Conchal bowl | Large graft, ideal for total perforations | Curved shape |
| Vein graft | Dorsum of hand | Easy harvest | Poor results, high failure rate |
| Fat graft | Ear lobule | Simple | Only for small pinhole perforations |
| Nasal mucosa | Inferior turbinate | Rich blood supply | Limited use |
8B. Allografts & Xenografts (Historical):
- Human dura mater (Tabb, 1960) — largely abandoned
- Pericardium — occasionally used
- Acellular dermal matrix (AlloDerm) — some centers
"Temporalis fascia and perichondrium are commonly used materials for TM reconstruction. Cartilage may be considered for reinforcement of retraction pockets, atelectatic membranes, and other conditions associated with increased failure rates of traditional techniques." — Cummings Otolaryngology
9. SURGICAL APPROACHES
9A. Transcanal (Endomeatal) Approach:
- Through external auditory meatus
- Best for: small/medium posterior perforations with wide meatus
- Advantage: no external incision, fast recovery
9B. Permeatal (Endaural) Approach:
- Incision through external meatus and between tragus/helix
- Best for: moderate perforations, moderate meatus size
- Rosen incision: 6 o'clock to 12 o'clock within the canal
9C. Postauricular (Retroauricular) Approach:
- Incision behind the ear in the postauricular sulcus
- Best for: total/large perforations, narrow meatus, combined mastoidectomy
- Provides best access and widest field
- Most common approach for formal tympanoplasty
APPROACHES TO TYMPANOPLASTY
┌─────────────────────────────────┐
│ SURGICAL APPROACH │
└──────────┬──────────────────────┘
│
┌────────────┼────────────┐
│ │ │
Transcanal Endaural Postauricular
(Permeatal) (Permeatal (Retroauricular)
extended)
│ │ │
Small/medium Medium Large/total
post. perf. perf. perforations
Wide canal Mod. canal ± Mastoidectomy
No incision Small ext. Best access
incision Most common
10. TECHNIQUES OF TYMPANOPLASTY
MYRINGOPLASTY (Type I Tympanoplasty):
The repair of TM alone without middle ear exploration when ossicular chain is intact.
A. UNDERLAY (MEDIAL) TECHNIQUE (Austin, Tos — cited in Scott-Brown)
Steps:
- Postauricular/endaural incision
- Elevation of tympanomeatal flap
- Freshening of perforation edges (rim of perforation de-epithelialized with pick)
- Elevation of middle ear mucosal flap
- Graft placed medial to TM remnant and medial to malleus handle
- Supported by Gelfoam in middle ear
- Flap repositioned
Advantages:
- Physiological (graft is deep)
- Better anterior visualisation
- Less risk of blunting
- Widely applicable
Disadvantages:
- Graft may tent around malleus → poor anterior healing
- Difficult in total perforations without malleus
B. OVERLAY (LATERAL) TECHNIQUE (Hermann — cited in Cummings)
Steps:
- Strip epithelium from TM remnant and lateral canal wall (canalplasty often needed)
- Squamous epithelium completely removed from TM remnant and annulus
- Graft placed lateral to fibrous annulus and TM remnant, but medial to malleus handle
- Graft underlies the dissected epithelium
Advantages:
- Excellent for total perforations and revision cases
- Promotes good vascular ingrowth
- Useful for secondary cholesteatoma of TM
Disadvantages:
- Technically demanding
- Risk of anterior blunting (flap meets canal wall)
- Risk of lateralization of TM
- Risk of skin inclusion (residual cholesteatoma)
UNDERLAY vs OVERLAY — DIAGRAMMATIC COMPARISON
UNDERLAY TECHNIQUE:
┌──────────────────────────────────┐
│ EAC │
│ ────────────────── │
│ | TM remnant | │
│ ────────────────── │
│ [GRAFT] ←── placed here │
│ medial to TM remnant │
│ medial to malleus handle │
│ Middle Ear Space │
│ [Gelfoam support] │
└──────────────────────────────────┘
OVERLAY TECHNIQUE:
┌──────────────────────────────────┐
│ EAC │
│ [GRAFT] ←── placed here │
│ lateral to annulus │
│ ────────────────── │
│ | TM remnant | │
│ ────────────────── │
│ Middle Ear Space │
└──────────────────────────────────┘
C. CARTILAGE TYMPANOPLASTY (Tos, Duckert — cited in Cummings)
Indicated when:
- Eustachian tube dysfunction (chronic)
- Revision tympanoplasty
- Perforation >50% of TM
- Atelectatic ear / retraction pockets
- Bilateral perforations
- Active discharge at time of surgery
- Reconstruction after cholesteatoma
- Anticipated ossiculoplasty (second stage)
Types of cartilage grafts:
- Composite cartilage/perichondrium graft — eccentric disk of cartilage with attached perichondrium; placed in underlay fashion
- Shield technique — cartilage disk with slot for malleus handle; perichondrium drapes over
- Palisade technique — thin cartilage slices placed parallel to malleus handle
"Variations of cartilage tympanoplasty have been reported to have high morphologic success rates (graft integration, intact TM) similar to or better than fascia tympanoplasty." — Cummings Otolaryngology
11. DETAILED SURGICAL STEPS (POSTAURICULAR UNDERLAY)
(Dhingra, Hazarika, Zakir Hussain)
SURGICAL STEPS — POSTAURICULAR UNDERLAY TYMPANOPLASTY
Step 1: PATIENT POSITIONING
└── Supine, head turned, operated ear up
Local infiltration (1:200,000 adrenaline) ± GA
Step 2: GRAFT HARVESTING
└── Postauricular incision → harvest temporalis fascia
Thin it out, dry on Teflon block
Step 3: POSTAURICULAR INCISION
└── 1 cm behind postauricular sulcus
Expose posterior EAC
Step 4: TYMPANOMEATAL FLAP
└── Canal incisions at 12 o'clock and 6 o'clock
Elevate flap anteriorly
Step 5: EXPOSURE OF MIDDLE EAR
└── Elevate annulus from sulcus
Enter middle ear at posteroinferior quadrant
Inspect ossicular chain & ET
Step 6: PREPARATION OF PERFORATION
└── Freshen edges of perforation
Remove 1mm rim of epithelium circumferentially
(using fine pick / crescent knife)
Elevate flap of epithelium from TM surface
Step 7: GRAFT PLACEMENT
└── Pass graft medial to malleus handle
Support anteriorly with Gelfoam
Ensure no fold-over / tenting
Graft should extend beyond perforation by 2mm all around
Step 8: REPOSITIONING FLAP
└── Tympanomeatal flap laid back over graft
Gelfoam packs laterally
Step 9: WOUND CLOSURE
└── Canal pack with soaked ribbon gauze
Postauricular wound closed in layers
12. OSSICULOPLASTY
(Cummings, Scott-Brown)
Ossiculoplasty is reconstruction of the ossicular chain to restore sound transmission.
Prostheses:
| Type | Abbreviation | Description | Use |
|---|---|---|---|
| Partial Ossicular Replacement Prosthesis | PORP | TM → stapes head | Malleus/incus absent, stapes present |
| Total Ossicular Replacement Prosthesis | TORP | TM → footplate | All ossicles absent, only footplate present |
| Autograft ossicle | — | Reshaped patient's own incus/malleus | Type II/III reconstruction |
Materials for prostheses:
- Titanium — gold standard; good results, low extrusion, easy to use
- Hydroxyapatite — biocompatible, osseoinductive
- Teflon/Plastipore — older, higher extrusion
- Gold — good but expensive
"Good hearing results, low extrusion rates, and ease of use have led to widespread application of titanium implants." — Cummings Otolaryngology
Ossiculoplasty Types (Wullstein):
OSSICULAR STATUS RECONSTRUCTION TYPE
─────────────────────────────────────────────────────────
All ossicles intact → TM repair only → Type I
Incus eroded → TM on malleus/incus → Type II
Malleus + incus gone → TM on stapes head → Type III (PORP)
Stapes superstructure → TM on footplate → Type IV (TORP)
absent, footplate
mobile
Footplate fixed → Fenestration SCC → Type V (obsolete)
13. EUSTACHIAN TUBE CONSIDERATIONS
(Stell & Maran, Hazarika, Dhingra)
The most important prognostic factor for tympanoplasty success.
- A patent, functional ET is essential — acts as pressure equaliser
- ET dysfunction → negative ME pressure → graft retraction → failure
- Tests of ET function: Valsalva, Politzerization, Toynbee test, tympanometry (Type C curve), sonotubometry
ET Dysfunction Management:
- Adenoidectomy in children
- Treat nasal allergies/sinusitis
- If ET is compromised → use cartilage graft (more retraction-resistant)
- Balloon Eustachian Tuboplasty (BET) — recent advance
14. TYMPANOPLASTY WITH MASTOIDECTOMY
(Scott-Brown, Cummings)
When is mastoidectomy combined?
- CSOM with cholesteatoma (modified radical mastoidectomy / canal wall up)
- CSOM with unsafe features (mastoid disease)
- Previous failed tympanoplasty with granulations
- Active mucosal disease extending to mastoid
Types:
- Combined approach tympanoplasty (CAT): Canal wall up + tympanoplasty — staged (1st: mastoidectomy; 2nd: ossiculoplasty after 6–12 months)
- Modified radical mastoidectomy + tympanoplasty: Canal wall down (open cavity)
15. DECISION ALGORITHM / FLOWCHART
CHRONIC EAR DISEASE — SURGICAL DECISION MAKING
OTOSCOPY + HRCT + AUDIOMETRY
│
┌──────────────┴──────────────┐
│ │
SAFE TYPE UNSAFE TYPE
(Tubotympanic) (Atticoantral/
Central perforation Cholesteatoma)
│ │
Dry >6 weeks? MASTOIDECTOMY
│ (Modified Radical /
┌────┴────┐ Canal Wall Up)
YES NO │
│ │ Ossicular chain
Audiometry Medical Rx status at surgery
│ │ │
ABG >15dB Dry achieved? ┌──────┴──────┐
│ Intact Eroded
TYMPANOPLASTY │ │
│ Stage 1: Stage 1:
┌───┴───────────┐ Tympanoplasty Mastoidectomy
│ │ │ Stage 2:
Ossicles Ossicles Stage 2: Ossiculoplasty
intact eroded Ossiculoplasty
│ │ (6-12 months)
Type I Type II/III
Myringoplasty + Ossiculoplasty
16. GRAFT HARVESTING — TEMPORALIS FASCIA
(Dhingra, Hazarika)
Steps:
- Postauricular incision extended superiorly
- Skin incised to temporalis fascia
- Window of fascia (2 × 3 cm) harvested with scissors
- Connective tissue stripped off
- Graft thinned and dried on Teflon block for 10–15 mins (or under microscope lamp)
- Trimmed to appropriate shape
Graft size: Slightly larger than perforation + 2–3 mm margin all around
17. POSTOPERATIVE CARE
(Dhingra, Zakir Hussain, Hazarika)
Immediate:
- Head elevated 30°
- Antiemetics, analgesics
- Prophylactic antibiotics (7 days)
- Avoid nose blowing, sneezing with open mouth
- Canal pack removed at 1–2 weeks
Follow-up Schedule:
- 1 week: wound check
- 3 weeks: remove external packing, check graft
- 6 weeks: audiogram
- 3 months: repeat PTA — assess hearing gain
- 6 months: final assessment
Diet/Activity:
- No strenuous activity for 4 weeks
- No swimming for 3 months
- Avoid flying for 4–6 weeks (ET pressure)
- No hearing aids for 3 months
18. COMPLICATIONS
Intraoperative:
| Complication | Cause | Management |
|---|---|---|
| TM laceration | Over-elevation of flap | Careful technique |
| Ossicular damage | Instrument slip | Repair/replace |
| Chorda tympani injury | Stretched or cut | Accept; taste disturbance resolves |
| Facial nerve injury | Aberrant nerve or over-drilling | Immediate recognition; steroids |
| Perilymph fistula | Instrument touching stapes | Seal with fat graft |
| Bleeding (ECA branches) | Deep incision | Bipolar cautery |
Early Postoperative:
- Haematoma
- Infection/otitis externa
- Graft displacement
- Vertigo (labyrinthitis)
- Facial nerve paresis (due to edema)
Late Postoperative:
┌─────────────────────────────────────────────────────────┐
│ CAUSES OF FAILED TYMPANOPLASTY │
├───────────────────────────┬─────────────────────────────┤
│ TECHNICAL FAILURES │ DISEASE-RELATED FAILURES │
├───────────────────────────┼─────────────────────────────┤
│ Poor graft support │ Persistent ET dysfunction │
│ Anterior blunting │ Active infection at surgery │
│ Graft lateralisation │ Residual cholesteatoma │
│ Skin inclusion │ Ongoing URTI/allergy │
│ Insufficient de- │ Inadequate mastoid disease │
│ epithelialisation │ treatment │
│ Failure medial to malleus │ Poor mucosal healing │
└───────────────────────────┴─────────────────────────────┘
- Anterior blunting (most common failure of lateral technique) — acute angle lost between anterior canal wall and TM
- Graft atrophy/retraction
- Re-perforation
- Residual conductive hearing loss — requires re-exploration
- SNHL — rare, due to inner ear exposure or drilling
19. RESULTS AND PROGNOSIS
(Cummings, Scott-Brown)
Graft Success Rates:
| Condition | Success Rate |
|---|---|
| Dry ear, simple perforation | 85–95% |
| Active discharge at surgery | 60–75% |
| Revision tympanoplasty | 70–80% |
| Cartilage tympanoplasty | 88–95% |
| Anterior/total perforation | 75–85% |
Hearing Results:
- Successful closure of air-bone gap to ≤20 dB in 70–80% of cases
- Type III ossiculoplasty: mean postop ABG 15–25 dB
- Cartilage does not significantly impair high-frequency hearing
Poor Prognosis Factors:
- Wet ear at time of surgery
- Poor ET function
- Total perforation
- Bilateral disease
- Children under 7 years
- Revision surgery
- Cholesteatoma
20. PEDIATRIC TYMPANOPLASTY
(Cummings — "Pediatric Tympanoplasty" section)
"Tympanoplasty in children under 7 years of age is associated with higher failure rates due to immature Eustachian tube function and frequent URTIs."
- Generally deferred until age 7–9 years
- Cartilage grafts preferred in pediatric population
- Combined adenoidectomy may improve ET function
- Success rates similar to adults after age 9
21. ENDOSCOPIC TYMPANOPLASTY (RECENT ADVANCES)
(Tarabichi, Poe, Kozin — Recent Literature)
Advantages:
- No postauricular incision → less morbidity
- Wide-angle panoramic view of middle ear
- Better illumination of anterior recess, sinus tympani
- Shorter operative time
- Reduced hospital stay (day-case surgery)
- Earlier return to work
Disadvantages:
- One-handed surgery (endoscope in one hand)
- Heat generation from endoscope
- Learning curve
- Limited ability to manage bleeding
Transcanal Endoscopic Ear Surgery (TEES):
- Type I–III tympanoplasty achievable endoscopically
- 0° and 30° endoscopes used
- Success rates comparable to microscopic technique
22. RECENT ADVANCES IN TYMPANOPLASTY
(Current Literature 2018–2024)
1. Regenerative Medicine:
- Growth factors (EGF, bFGF) applied to perforation edges to stimulate healing — ongoing clinical trials
- Platelet-rich plasma (PRP) graft overlay — enhances vascularization and graft uptake
- Stem cell-seeded scaffolds — experimental stage
2. New Graft Materials:
- Acellular dermal matrix (AlloDerm) — off-the-shelf, avoids donor site morbidity
- Porcine small intestinal submucosa (Cook Biodesign) — used in revision cases
- Silk fibroin scaffolds — biodegradable, biocompatible; under investigation
3. Balloon Eustachian Tuboplasty (BET):
- Dilation of ET orifice with balloon catheter
- Combined with tympanoplasty in ET dysfunction cases
- Improves success rates in recurrent graft failure
4. Endoscopic-Assisted and Robot-Assisted Surgery:
- Robotic ear surgery systems under development
- Two-handed robotic approach overcomes limitation of single-hand endoscopic surgery
5. Fat Myringoplasty (Office-Based):
- For small (<3 mm) pinhole perforations
- Performed under local anaesthesia in clinic
- Fat harvested from ear lobule
- 80–90% success for appropriate cases
6. Pharmacological Advances:
- Mitomycin C — used to prevent adhesions post-surgery
- Ciprofloxacin ear drops — drug-eluting packing materials
7. Outcomes Research:
- ICHOM Middle Ear Disease Standard Set — international consensus on outcome measurement
- Patient-reported outcomes (PROS) increasingly incorporated
- Disease-specific QoL tools: COMQ-12, GHSI
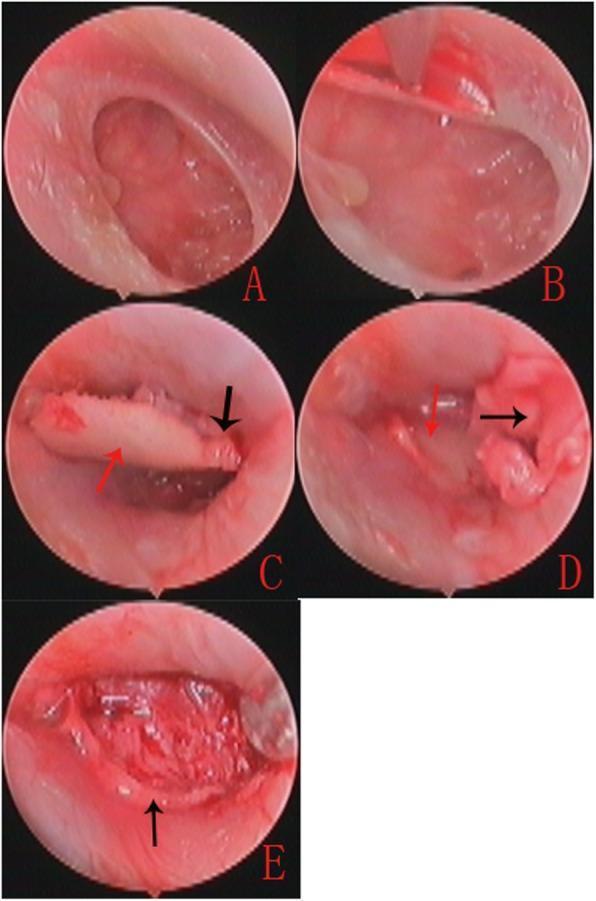
23. INTRAOPERATIVE IMAGES
Image 1: Intraoperative — Bucket Handle Tympanoplasty (Underlay Technique)
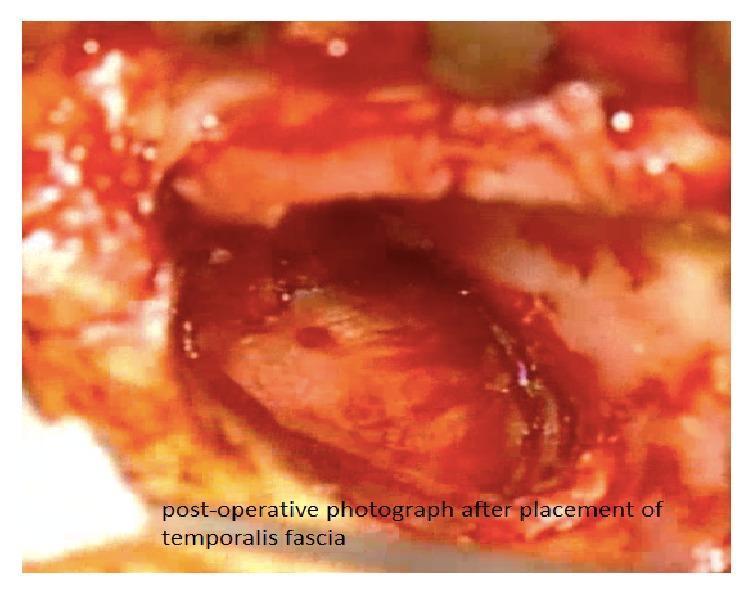
Image 2: Nasal Mucosa Graft — Type I Tympanoplasty
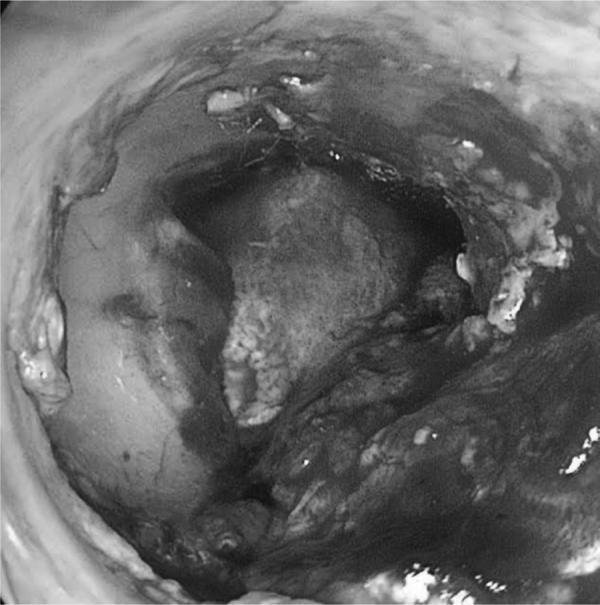
Image 3: Composite Cartilage-Perichondrium Graft — Surgical Sequence
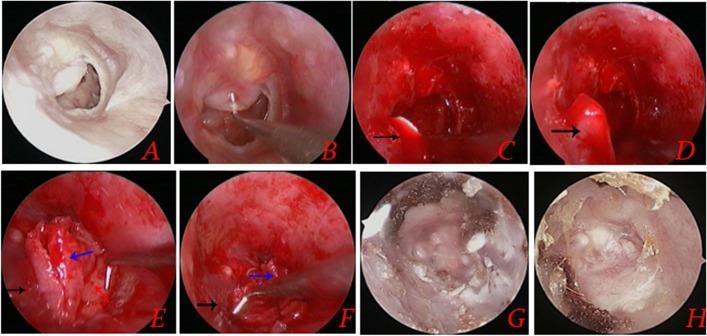
Image 4: Total Ossicular Replacement Prosthesis (TORP) on CT
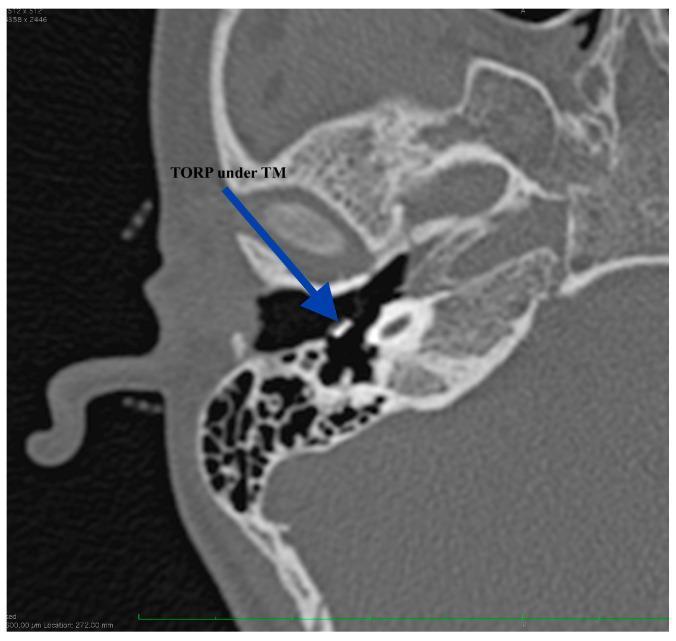
Image 5: Cartilage-Perichondrium Underlay-Overlay Composite Technique
24. SUMMARY FLOWCHART — MANAGEMENT ALGORITHM
TYMPANOPLASTY — COMPLETE MANAGEMENT ALGORITHM
CHRONIC OTITIS MEDIA (Safe Type)
│
┌───────────┴───────────────┐
│ │
WET EAR DRY EAR
│ │
Medical treatment PTA + Tympanometry
4–6 weeks HRCT Temporal Bone
│ │
Dry?──────NO──►Consider Counselling + Consent
│ Mastoid │
YES surgery TYMPANOPLASTY
│
Audiometry
│
ABG <15 dB ──► Observe / no surgery
│
ABG >15 dB ──► TYMPANOPLASTY
│
┌───────────┼───────────┐
│ │ │
Fascia Cartilage Fat graft
(standard) (ETD, large, (small <3mm
revision) pinhole)
│
┌─────────────┼─────────────┐
│ │ │
Underlay Overlay Cartilage
(medial) (lateral) shield/palisade
│
At surgery: Assess ossicular chain
│
├── Intact ──────────────► Type I (Myringoplasty)
├── Incus eroded ─────────► Type II
├── Malleus + incus gone ─► Type III + PORP
└── All ossicles gone ───► Type IV + TORP
│
POSTOP FOLLOW-UP
(PTA at 6 weeks, 3 months)
25. QUICK SUMMARY TABLE
| Parameter | Details |
|---|---|
| Definition | Surgery to close TM perforation + restore middle ear function |
| Coined by | Wullstein & Zöllner (1952–55) |
| Classification | Types I–V (Wullstein) |
| Most common type | Type I (Myringoplasty) |
| Best graft | Temporalis fascia (standard); Cartilage (ETD, revision) |
| Approach | Postauricular (most common); Transcanal (small perforation) |
| Technique | Underlay (standard); Overlay (revision/total); Cartilage (ETD) |
| Key factor for success | Eustachian tube function |
| Success rate | 85–95% (dry ear, simple perforation) |
| Recent advance | Endoscopic ear surgery (TEES), BET, PRP, AlloDerm |
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery, 7th ed. — Chapter 142: Tympanoplasty and Ossiculoplasty (Adams ME, El-Kashlan HK)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed. — Tympanoplasty chapter
- Dhingra PL — Diseases of Ear, Nose and Throat & Head-Neck Surgery, 7th ed.
- Stell & Maran's Head and Neck Surgery, 5th ed.
- Hazarika P — Textbook of ENT & Head-Neck Surgery, Clinical & Practical, 4th ed.
- Zakir Hussain — ENT & Head-Neck Surgery
- K.J. Lee's Essential Otolaryngology, 11th ed. — Tympanoplasty and Mastoidectomy
- Wullstein HL. Theory and Practice of Tympanoplasty. Laryngoscope. 1956;66:1076–93.
- Tarabichi M. Endoscopic transcanal middle ear surgery. Indian J Otolaryngol. 2010;62:6–24.
- Tos M. Cartilage tympanoplasty: description of techniques and results. Otolaryngol Head Neck Surg. 2009.
- Shakeel M et al. Recent advances in tympanoplasty — a systematic review. Clin Otolaryngol. 2021.
- Marchioni D et al. Endoscopic ear surgery: principles, indications, and techniques. Otol Neurotol. 2019.
This answer covers all RGUHS examination requirements for a 50-mark tympanoplasty question: definition, history, anatomy, Wullstein's classification, indications, preoperative assessment, graft materials, surgical approaches, techniques (underlay/overlay/cartilage), ossiculoplasty, ET considerations, complications, results, pediatric aspects, and recent advances including endoscopic ear surgery.
This is a shared conversation. Sign in to Orris to start your own chat.