LEEP procedure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the Loop Electrosurgical Excision Procedure (LEEP):
LEEP (Loop Electrosurgical Excision Procedure)
Also known as LLETZ (Large Loop Excision of the Transformation Zone) or simply "loop excision."
Overview
LEEP uses thin wire loop electrodes carrying high-frequency electrical current to excise the entire cervical transformation zone (TZ). It is currently the most widely used treatment for biopsy-confirmed CIN 2 and CIN 3.
Advantages over other treatment methods:
- Tissue specimen available for pathologic review (unlike cryotherapy or ablation)
- Performed in an outpatient/office setting under local anesthesia
- Lower cost than cold-knife conization or laser surgery
- Single-visit "see-and-treat" option possible
- Low complication rate
Indications
- Biopsy-confirmed CIN 2 or CIN 3
- Certain cases of CIN 1 persisting >2 years
- Unsatisfactory colposcopy with suspected high-grade lesion
- Positive endocervical curettage (ECC)
- Discordance between Pap smear, colposcopy, and biopsy findings
Contraindications
| Absolute | Relative |
|---|---|
| Active pelvic infection | Pregnancy (LEEP can be performed with precautions) |
| Desire to preserve fertility (consider conservative management) | Postmenopause |
| Lesion not fully visualized |
Equipment
- Electrosurgical generator with a smoke evacuator (e.g., Utah Medical, CooperSurgical, Ellman Surgitron)
- Loop electrodes: 2.0 × 0.8 cm (standard exocervical), 1 × 1 cm or square (endocervical)
- Ball electrode for hemostasis
- Non-conductive, vented vaginal speculum (required — prevents arcing)
- Dispersive grounding pad
- Local anesthetic (typically 1–2% lidocaine with epinephrine 1:100,000 injected into the cervical stroma)
- Lugol's solution and/or acetic acid (5%) for lesion delineation
- Monsel's paste (ferric subsulfate) for hemostasis
Procedure
Patient Preparation
- Place patient in dorsal lithotomy position.
- Insert the non-conductive speculum — standard metal specula are not used because they may conduct current.
- Apply 5% acetic acid and/or Lugol's iodine to delineate the lesion and TZ.
- Infiltrate the cervical stroma at 3, 6, 9, and 12 o'clock with local anesthetic containing epinephrine (vasoconstrictive effect reduces bleeding).
- Attach the grounding pad to the patient's thigh.
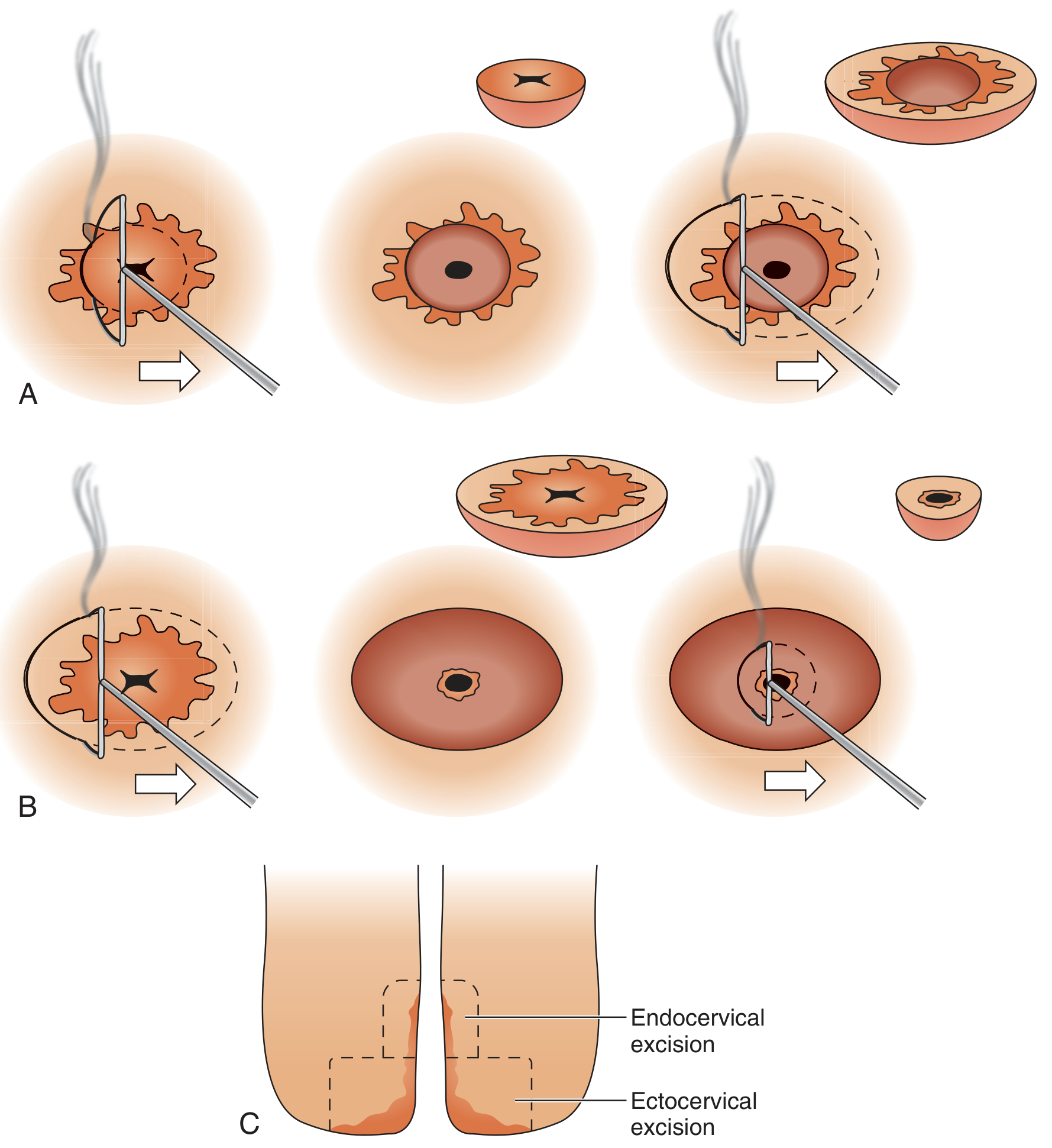
Routine LEEP (Exocervical Lesions)
- Using a 2.0 × 0.8 cm loop electrode, enter the cervix 3–5 mm outside the lateral margin of the TZ.
- Activate current and pass the loop smoothly through the cervix with steady, even pressure — move too slowly and thermal artifact increases; too fast and incomplete excision results.
- The loop is brought out on the contralateral side, removing the entire TZ and CIN lesion in a single pass.
- Submit the specimen in formalin.
- Apply Monsel's paste or use the ball electrode for hemostasis.
For large lesions not removable in a single pass: excise the central portion first, then excise remaining tissue with additional passes, or ablate the periphery with ball electrode coagulation.
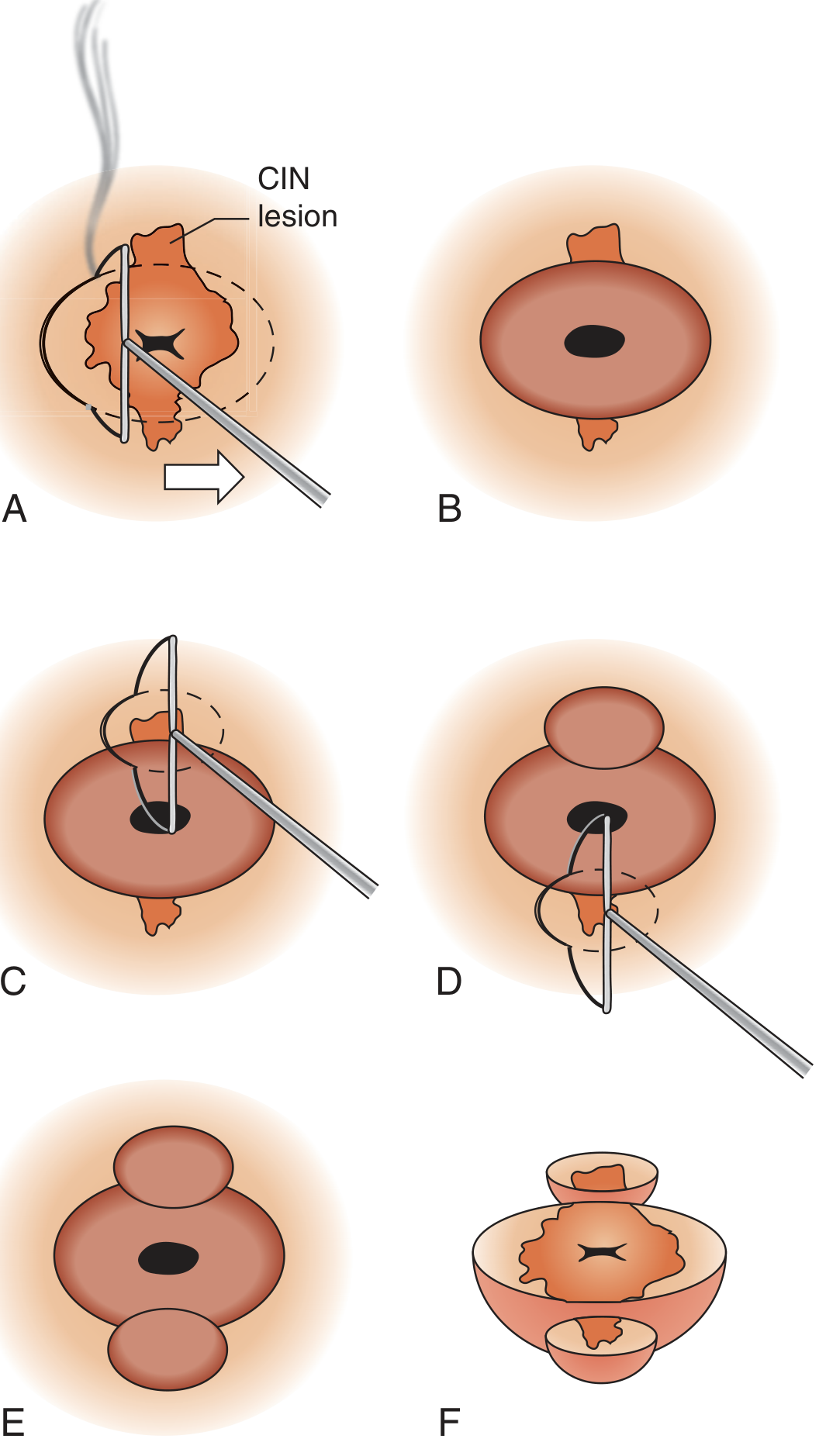
LEEP Conization (Endocervical Extension — "Cowboy-Hat" Technique)
Used when CIN extends into the endocervical canal. A two-electrode approach produces a cowboy-hat shaped excision.
Method 1 (endocervical first):
- Excise the endocervical portion using a 1 × 1 cm endocervical electrode.
- Then excise the exocervical portion with the standard 2.0 × 0.8 cm loop.
Method 2 (exocervical first):
- Excise the large ectocervical portion first.
- Follow with the smaller endocervical electrode.
Caution: Do not excise the endocervical canal deeper than 1.5 cm — increased risk of significant bleeding and cervical stenosis.
Endocervical and exocervical specimens must be submitted in separate containers.
Pathologic Assessment
- Specimens should ideally be opened along one side and placed in a holder to fix in proper orientation.
- Thermal artifact at the margins is a known limitation — may make margin assessment difficult.
- An endocervical curettage (ECC) performed after LEEP helps assess residual disease above the excised specimen.
- Report should address: CIN grade, endo- and ecto-cervical margin status.
Complications
| Complication | Notes |
|---|---|
| Intraoperative bleeding | Vasospasm from epinephrine usually limits this; Monsel's paste or ball electrode used |
| Postoperative bleeding | Most common significant complication; occurs in ~2–4%; may require re-treatment or suturing |
| Infection | Uncommon; patients advised to avoid intercourse/tampons for 4 weeks |
| Cervical stenosis | Risk increases with deeper excisions (especially conization); may impair fertility/Pap sampling |
| Incomplete excision | Positive margin does not always indicate treatment failure — many women with positive margins have no residual disease at follow-up |
Obstetric Implications
Women treated with LEEP have an increased risk of preterm birth in subsequent pregnancies. The risk correlates with the depth and volume of tissue removed. This is particularly relevant when LEEP conization is performed. — Creasy & Resnik's Maternal-Fetal Medicine
Follow-Up
- Post-LEEP follow-up typically includes co-testing (HPV + cytology) at 6 months and 12 months.
- Positive margins warrant closer surveillance but not automatic re-treatment.
- Recurrence rate following LEEP for CIN 2/3 is approximately 5–15% depending on margin status and HPV persistence.
— Pfenninger and Fowler's Procedures for Primary Care, 3rd ed., pp. 1039–1047; Berek & Novak's Gynecology; Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.