ACLS guide line
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
ACLS algorithm cardiac arrest shockable non-shockable rhythm
Reading File
Loading Image
Here is a comprehensive ACLS (Advanced Cardiac Life Support) overview based on current guidelines, drawn from multiple authoritative textbooks:
ACLS Guidelines Overview
What is ACLS?
Advanced Cardiac Life Support extends Basic Life Support (BLS) by adding:
- Advanced airway management
- IV/IO vascular access
- Vasopressor and antiarrhythmic medications
- Advanced physiologic monitoring (ET CO₂, arterial BP, oximetry, ultrasound)
- Rhythm diagnosis and targeted treatment
The Core Framework: Shockable vs. Non-Shockable Rhythms
ACLS management branches based on the presenting rhythm:
| Shockable | Non-Shockable |
|---|---|
| Ventricular Fibrillation (VF) | Asystole |
| Pulseless Ventricular Tachycardia (pVT) | Pulseless Electrical Activity (PEA) |
Shockable Rhythm Algorithm (VF / Pulseless VT)
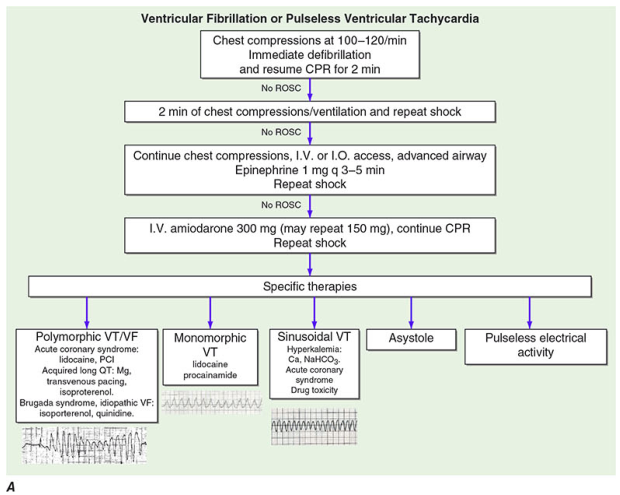
- Chest compressions 100–120/min → Immediate defibrillation → Resume CPR 2 min
- If no ROSC → 2 min CPR + repeat shock
- If no ROSC → IV/IO access + advanced airway + Epinephrine 1 mg q3–5 min + repeat shock
- If no ROSC → IV Amiodarone 300 mg (may repeat 150 mg) + continue CPR + repeat shock
- Specific therapies based on rhythm subtype (see below)
Specific therapies by rhythm:
- Polymorphic VT/VF: lidocaine, PCI (if ACS); long QT → Mg, transvenous pacing, isoproterenol; Brugada/idiopathic VF → isoproterenol, quinidine
- Monomorphic VT: lidocaine, procainamide
- Sinusoidal VT (hyperkalemia): Ca²⁺, NaHCO₃; if ACS or drug toxicity — specific reversal
- Asystole / PEA: Address reversible causes (H's & T's)
Airway Management
- Both bag-mask ventilation (BMV) and advanced airway (ETI or supraglottic airway/SGA) are acceptable per 2019 AHA/ACC guidelines
- BMV: ~600 mL per breath over 1 second with tight face seal
- Advanced airway: 1 breath every 6 compressions (10/min)
- SGA is preferred over ETI when operator experience is limited or ETI success is expected to be low
- A large RCT (n=2040) showed no survival difference between BMV and ETI
Medications
| Drug | Dose | Indication |
|---|---|---|
| Epinephrine | 1 mg IV/IO q 3–5 min | All cardiac arrest rhythms |
| Amiodarone | 300 mg IV, then 150 mg | VF/pVT refractory to defibrillation |
| Lidocaine | Alternative to amiodarone | VF/pVT |
| Magnesium sulfate | 1–2 g IV | Torsades de pointes / hypomagnesemia |
| Atropine | 0.5–1 mg IV | Symptomatic bradycardia |
| Vasopressin | 40 units IV | Alternative vasopressor (less commonly used now) |
Epinephrine note: A trial of 8,014 patients showed slightly higher 30-day survival with epinephrine vs. placebo (3.2% vs 2.4%, P=0.02), but no difference in favorable neurologic outcome (2.2% vs 1.9%). — Fuster and Hurst's The Heart, 15th Ed.
Monitoring During ACLS
| Monitor | Value | Significance |
|---|---|---|
| End-tidal CO₂ (ETCO₂) | 15–20 mmHg during CPR | Normal = 35–45 mmHg |
| ETCO₂ at ROSC | Jumps to >35 mmHg | Reliable indicator of ROSC |
| ETCO₂ <10 mmHg after >20 min | Poor prognostic marker | May indicate futility |
Reversible Causes — The "H's and T's"
| H's | T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo/Hyperkalemia | Thrombosis (pulmonary — PE) |
| Hypothermia | Thrombosis (coronary — ACS) |
Echocardiography can rapidly identify tamponade, massive MI, and other structural causes during ACLS.
Special Situations
Patients with Pacemakers / AICDs
- CPR can be performed in standard fashion
- If AICD shocks are impeding CPR, disable it with a magnet over the device corner
- Place defibrillation pads ≥10 cm from the pulse generator
- Use anteroposterior pad placement to minimize energy shunting
- After ROSC, interrogate the device promptly — Roberts and Hedges' Clinical Procedures in Emergency Medicine
LVAD Patients
- Ensure LVAD is connected, battery charged, and audible hum is present
- Peripheral pulses may be absent at baseline — complicate arrest assessment
- Follow standard ACLS algorithms if arrest confirmed
Pediatric Considerations
- Cardiac arrest in children is usually secondary to respiratory arrest (not primary cardiac)
- VF/pVT is less common in children (3–17% vs. majority in adults)
- Defibrillation dose: 2 J/kg initial, increasing to 4 J/kg if needed
- Common terminal rhythms in children: PEA, bradycardia, asystole
When to Stop ACLS
ETCO₂ <10 mmHg after >20 minutes of resuscitation with an advanced airway in place is a validated marker of futility and may support discontinuation of efforts. — Fuster and Hurst's The Heart, 15th Ed.
Sources: Fuster and Hurst's The Heart (15th Ed.) | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Harrison's Principles of Internal Medicine (21st Ed.) | Miller's Anesthesia (10th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.