Latest ACL guide
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content to compile the ACL guide. Here's the complete summary:
ACL (Anterior Cruciate Ligament) — Clinical Guide
Anatomy
The ACL consists of two fiber bundles named by their tibial insertions:
| Bundle | Length | Taut in |
|---|---|---|
| Anteromedial (AM) | ~38 mm | Flexion |
| Posterolateral (PL) | ~20 mm | Extension |
The femoral origin lies in the posterior lateral intercondylar fossa. The AM bundle's origin borders superiorly on the intercondylar line; the PL bundle courses along the bone-cartilage border. Together, the two bundles provide anterior stability and rotational stability through the full arc of knee motion.
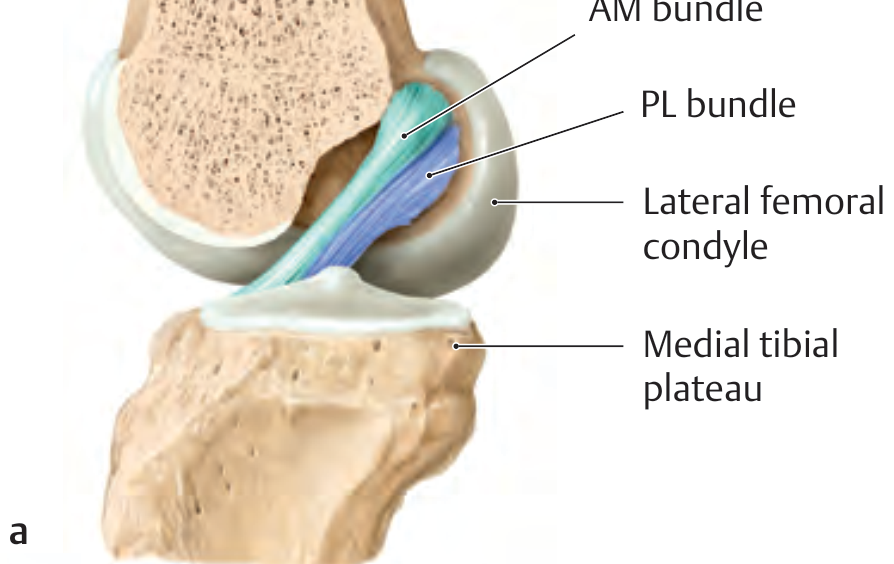
ACL anatomy showing AM and PL bundles and their femoral/tibial footprints — General Anatomy and Musculoskeletal System (THIEME Atlas)
Mechanism of Injury
- Usually noncontact: deceleration, hyperextension, or marked internal rotation of the tibia on the femur
- Classic presentation: audible "pop" (considered pathognomonic), rapid hemarthrosis (swelling within hours), and a sense of instability
- The combination of this mechanism + traumatic effusion is highly suggestive of ACL disruption
Diagnosis
Clinical Tests
| Test | Sensitivity | Specificity | Technique |
|---|---|---|---|
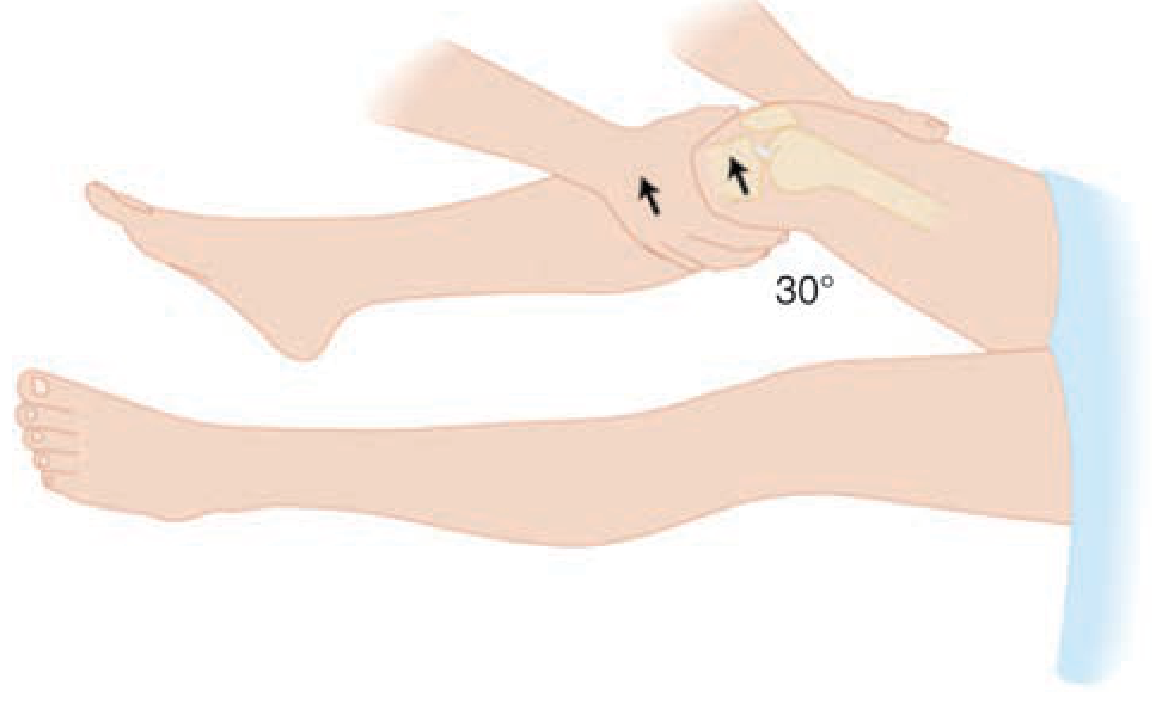
| Lachman test (most sensitive) | 81% | 81% | Knee at 30° flexion; stabilize femur, anteriorly translate tibia at the tibial tubercle level. Positive = anterior displacement or soft end point |
| Anterior drawer test | 38% | 81% | Hip 45° flexion, knee 90° flexion; pull tibia anteriorly. Positive = >6 mm displacement vs. contralateral knee |
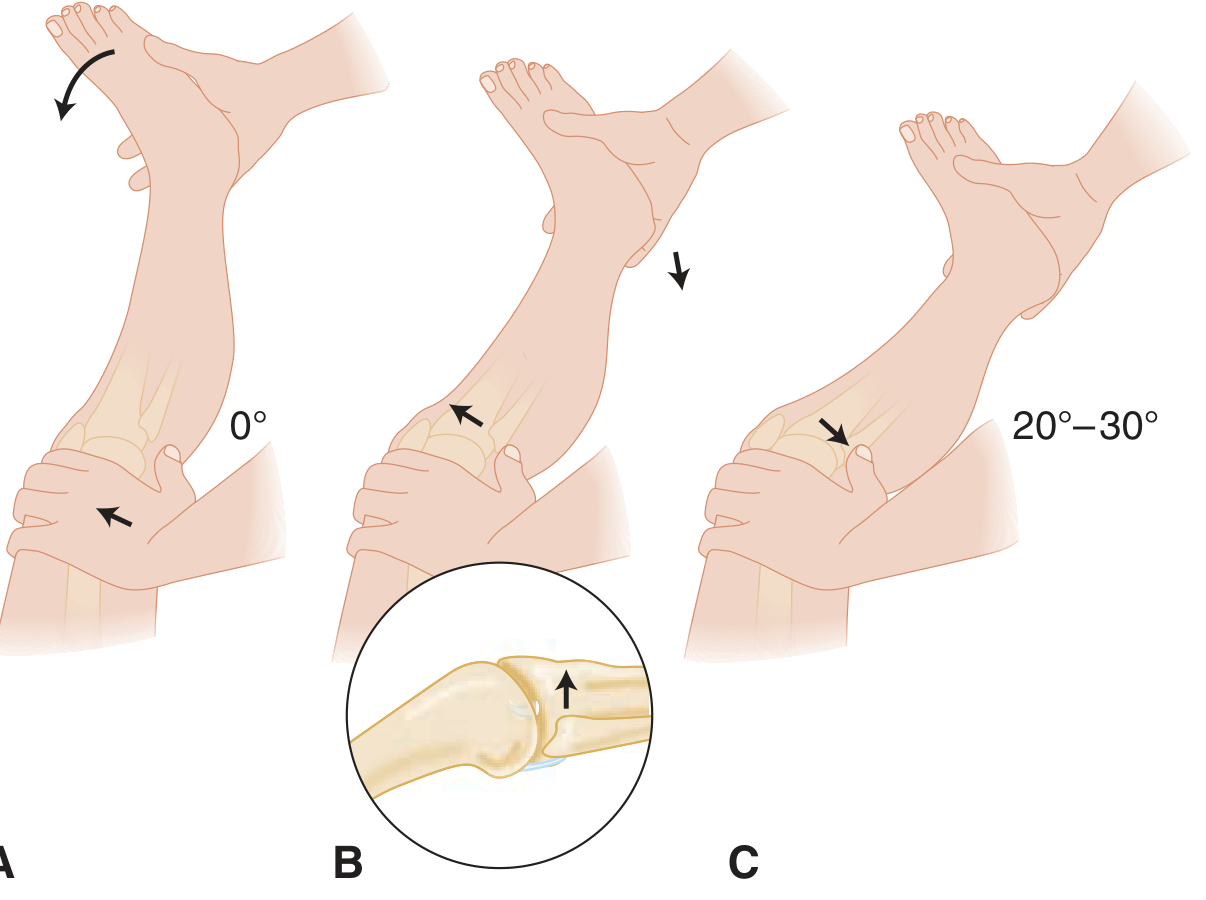
| Pivot shift test | 28% | 81% | Knee in full extension; apply valgus + internal rotation, then flex. Positive = sudden audible/palpable clunk of tibial reduction at ~20–30° flexion |

Pearls:
- Anterior drawer can give a false negative (hamstring guarding) or false positive (PCL tear → tibia starts posteriorly subluxed, giving pseudo-anterior displacement)
- Pivot shift is best assessed under anesthesia in the OR
- Lachman is preferred in the ED; it can identify partial tears
Imaging
- Plain radiographs: usually normal; may show a Segond fracture (avulsion of the lateral tibial plateau — a specific marker for ACL tear) or a tibial spine avulsion (pediatric equivalent)
- MRI: gold standard for confirmation; demonstrates ACL fiber discontinuity, altered signal, bone bruising pattern (lateral femoral condyle + posterolateral tibial plateau)
Management
Acute / ED Management
- Ice, compression, elevation; non-weight-bearing with crutches
- Analgesics / NSAIDs
- Knee immobilizer for comfort
- Urgent orthopedic referral — especially if combined ligament injury, locked knee, or neurovascular compromise
Definitive Treatment
| Patient Group | Approach |
|---|---|
| Active/young patients, pivoting sports | ACL reconstruction (patellar tendon or hamstring autograft preferred) |
| Sedentary/elderly or isolated partial tears | Conservative: physiotherapy, bracing, quadriceps strengthening |
| Combined instability (PCL, MCL, posterolateral corner) | Surgical reconstruction, timing individualized |
Surgical note: Replacement grafts face a major challenge — no human-made material fully replicates the ACL's mechanical properties. Reconstruction options include bone-patellar tendon-bone (BTB), hamstring tendon, and allograft.
Associated Injuries (the "Unhappy Triad")
Valgus force + ACL injury commonly involves:
- Medial collateral ligament (MCL) tear
- Medial meniscus tear
Also watch for peroneal nerve injury with lateral-sided instability.
Key Differentials
- PCL tear: posterior drawer positive, sag sign; mechanism is anterior-to-posterior force on tibia (e.g., dashboard injury)
- Meniscal tear: may coexist; McMurray/Thessaly tests positive
- Tibial spine avulsion: radiographic equivalent of ACL rupture in children/adolescents
Sources: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9e | General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.