Invasive pulmonary Aspergillosis full details for md exam answer 10 marks from fishman and murray only
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, detailed content from both Fishman's Pulmonary Diseases and Disorders and Murray & Nadel's Textbook of Respiratory Medicine. I have enough to write an excellent 10-mark MD exam answer. Let me compose it now.
Invasive Pulmonary Aspergillosis (IPA)
MD Exam Answer - 10 Marks
(Sources: Fishman's Pulmonary Diseases and Disorders, 5e; Murray & Nadel's Textbook of Respiratory Medicine)
1. Definition and Overview
Invasive Pulmonary Aspergillosis (IPA) is the most severe form of pulmonary aspergillosis, characterized by tissue invasion by Aspergillus hyphae with angioinvasion, necrosis, and potential hematogenous dissemination. It is a leading cause of infectious death in severely immunocompromised patients, with mortality rates of 30-50% in leukemia patients and HSCT recipients. (Fishman's)
2. Epidemiology
- Most common fungal infection in HSCT and solid organ transplant (SOT) recipients - comprising 43% and 59% of all invasive fungal infections (IFIs) respectively, surpassing invasive candidiasis. (Fishman's)
- 12-month cumulative incidence: 1.6% in transplant recipients; overall mortality ~36% at 12 weeks and ~75% at 1 year. (Fishman's)
- Approximately 15-20% of patients with leukemia die of Aspergillus fungal pneumonia. (Fishman's)
- IPA has a bimodal distribution in allogeneic HSCT: early (pre-engraftment neutropenia) and late (post-engraftment, in the setting of GvHD 40-80+ days after engraftment). (Fishman's)
- High-risk groups:
- Prolonged/profound neutropenia due to hematologic malignancy: 5-25% risk
- Allogeneic HSCT recipients: 5-30% risk
- Lung transplant recipients: 17-26% risk
- CGD, AIDS, severe combined immunodeficiency: 25-40% lifetime risk
- Patients on chronic corticosteroids, burn patients
- Emerging new risk groups: ibrutinib (BTK inhibitor) users, patients with SLE/multiple myeloma on high-dose steroids, critically ill ICU patients with COPD/cirrhosis/renal failure/diabetes, patients with severe influenza. (Fishman's, Murray's)
- Nosocomial outbreaks are linked to hospital construction and defects in air-handling systems. (Fishman's)
- Geoclimatic changes with high environmental spore counts (high temperature, low precipitation) are an emerging risk factor. (Fishman's)
3. Causative Organisms
- Aspergillus fumigatus is the most common species.
- Others: A. flavus, A. terreus, A. niger, A. nidulans.
- A. terreus is clinically resistant to amphotericin B.
- Azole-resistant strains of A. fumigatus are an emerging concern, partly due to environmental exposure to agricultural fungicides. (Fishman's)
4. Pathogenesis
Mechanism of infection:
- Inhalation of Aspergillus conidia (primary route); rarely, hematogenous seeding from cutaneous or GI sources. (Fishman's)
- In immunocompetent hosts, alveolar macrophages phagocytose and kill conidia. In the neutropenic host, this defense fails.
- Prior mucosal damage (radiation, chemotherapy, GvHD, viral infection such as RSV/influenza) facilitates attachment of conidia to the respiratory epithelium.
- Acquired iron overload promotes Aspergillus invasive growth and impairs antifungal pathways in phagocytes. (Fishman's)
- Conidia germinate into hyphae, which penetrate the respiratory mucosa and invade pulmonary arterioles and endothelial cells. (Murray's)
Two pathologic patterns (Murray's):
- Angioinvasive IPA: hyphae invade blood vessels → intravascular thrombosis → ischemia → coagulative necrosis and hemorrhagic infarction. Seen predominantly in neutropenia. Hematogenous dissemination occurs in ~1/3 of cases at autopsy, affecting the brain, kidney, liver, heart, and skin.
- Non-angioinvasive IPA: associated with pyogranulomatous inflammation and inflammatory necrosis; more common in non-neutropenic hosts.
IPA in sepsis-induced immunosuppression: Critically ill patients develop immune paralysis (cytokine hyporesponsiveness of myeloid cells) following sepsis, creating susceptibility to opportunistic Aspergillus infection without classic neutropenia. (Fishman's)
5. Clinical Presentation
- Classic symptoms: fever (often unresponsive to antibiotics), cough, hemoptysis, pleuritic chest pain, dyspnea. (Murray's)
- Angioinvasive IPA in neutropenia: rapid clinical deterioration over hours to days.
- Disseminated disease may produce symptoms at other sites (CNS - seizures/focal deficits, skin lesions, hepatic/renal involvement).
- Direct extension may involve the chest wall, mediastinum, pericardium, and great vessels. (Murray's)
- IPA mimics thrombotic/embolic diseases such as pulmonary embolism (due to vascular invasion), cerebral vascular accidents, and Budd-Chiari syndrome. (Fishman's)
6. Diagnosis
Early diagnosis is essential - it is associated with improved survival. Diagnosis is challenging due to lack of early symptoms, difficulty obtaining tissue in cytopenic/critically ill patients, and variable sensitivity/specificity of tests. (Murray's)
A. Imaging
- Chest CT is the preferred initial imaging modality - more sensitive than plain X-ray.
- Findings include: nodules, consolidation, cavitation, pleural effusion.
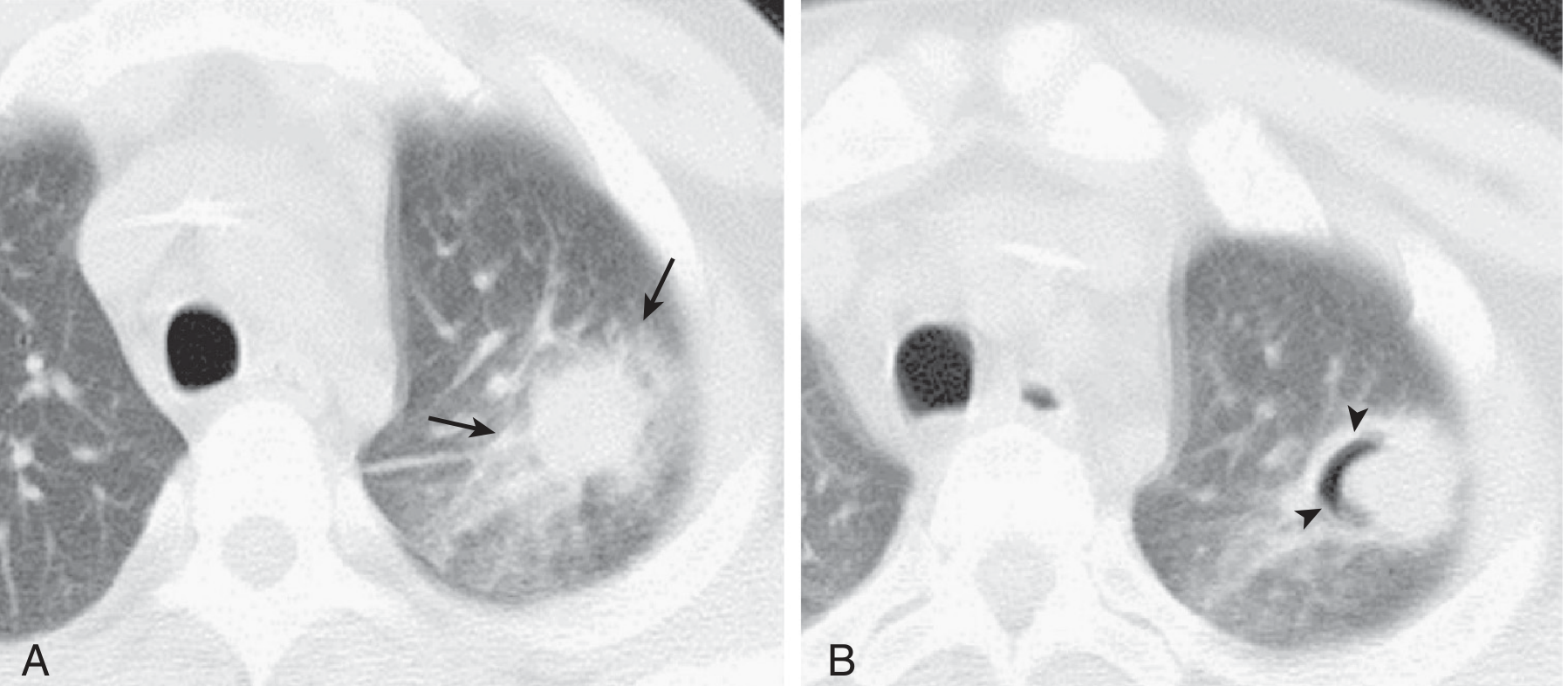
- Halo Sign (early): ground-glass opacity surrounding a pulmonary nodule, due to alveolar hemorrhage around an infarcted area - high specificity for IPA in neutropenic patients; seen early in disease. (Murray's, Fig. 57.4A)
- Air-Crescent Sign (late): crescent of air between necrotic and viable lung tissue - seen late, typically with recovery of neutrophils (neutrophil recovery causes liquefaction of infarcted lung). (Murray's, Fig. 57.4B)
B. Microbiologic Tests
- Direct microscopy of sputum/BAL: lacks sensitivity and specificity; Aspergillus hyphae are septate, branching at 45° angles.
- Culture (BAL, sputum, tissue): grows within 48-72 hours; but in up to 70% of tissues with septate hyphae, culture is negative. (Murray's)
- Histopathology: H&E, PAS, and Gomori's methenamine silver (GMS) staining - demonstrates characteristic septate, acutely branching hyphae invading tissue. Required for "proven" diagnosis.
C. Serologic/Antigen Tests
Galactomannan (GM) assay:
- GM is a heteropolysaccharide component of the Aspergillus cell wall, released during hyphal growth.
- FDA-approved Platelia Aspergillus EIA detects GM in serum and BAL; positive cutoff = ODI ≥ 0.5. (Murray's)
- Meta-analysis (27 studies): sensitivity 71%, specificity 89% for serum GM in immunocompromised hosts. (Murray's)
- Better in hematologic malignancy (sens 70%, spec 92%) and HCT (sens 82%, spec 86%) than in SOT (sens only 22%).
- BAL GM: sensitivity ~87% (meta-analysis of 30 studies, cutoff ODI 0.5); particularly useful in non-neutropenic hosts who may lack positive serum GM. (Murray's)
- False positives: cross-reactivity with other fungi (Fusarium, Histoplasma, Penicillium), IV immunoglobulin, certain antibiotics (piperacillin-tazobactam), nutritional supplements.
- False negatives: concomitant antifungal therapy reduces sensitivity.
- Serial GM monitoring may predict clinical outcomes (magnitude and trend).
Beta-D-Glucan (BDG) assay:
- Cell wall component of most fungi (not Mucorales or Cryptococcus).
- Less specific for Aspergillus; not recommended by ISHLT in cardiothoracic transplant populations due to high false-positive rates. (Murray's)
D. Molecular Tests (PCR)
- Real-time PCR: high negative predictive value; sensitivity 58%, specificity 96.2% when two consecutive positive results required. (Murray's)
- No FDA-approved Aspergillus NAT currently exists; standardization efforts ongoing via the European Aspergillus PCR Initiative (EAPCRI).
- Combined serum GM + Aspergillus PCR monitoring is associated with earlier diagnosis. (Murray's)
- BAL PCR should be interpreted in combination with other tests (radiology, culture).
E. Lateral Flow Assays (LFAs)
- Point-of-care testing detecting antigens secreted during Aspergillus growth; applicable to urine, serum, BAL. Promising but not yet standard. (Murray's)
F. Diagnostic Criteria - MSG/EORTC Definitions
| Category | Criteria |
|---|---|
| Proven IPA | Microscopic evidence of Aspergillus tissue invasion OR positive culture from normally sterile site |
| Probable IPA | At-risk host + corroborating CT findings + direct or indirect mycologic evidence (positive GM, culture, or histology from BAL/sputum) |
| Possible IPA | At-risk host + clinical/radiologic evidence, but no mycologic confirmation |
(Murray's)
7. Treatment
A. Primary Antifungal Therapy
Voriconazole is the drug of choice for IPA based on:
- A landmark randomized controlled trial showing significantly better response rates and overall survival with voriconazole compared to conventional amphotericin B deoxycholate (AMB-d). (Murray's, Fishman's - IDSA and ATS guidelines)
- Route: IV initially in critically ill patients, then oral step-down once stabilized.
- Monitoring of drug levels is required due to erratic pharmacodynamics and drug-drug interactions.
Alternative primary agents:
- Isavuconazole: broad spectrum (Candida, Aspergillus, Mucorales); excellent absorption, fewer drug interactions, predictable pharmacokinetics, less need for drug level monitoring. (Fishman's)
- Liposoidal Amphotericin B (L-AMB): used in azole-intolerant patients or where azole resistance is suspected; reduced nephrotoxicity vs. AMB-d.
- Posaconazole: broadest-spectrum azole; used for refractory disease.
B. Combination Therapy
- Not routinely recommended first-line due to insufficient RCT data.
- A large RCT (voriconazole vs. voriconazole + anidulafungin) failed to show significant 6-week mortality benefit with combination therapy overall; however, subgroup analysis showed significantly reduced 6-week mortality in patients with probable IPA diagnosed by radiology + serum/BAL GM - reflecting benefit in earlier disease. (Murray's)
- Current IDSA guidelines: combination therapy (echinocandin + voriconazole) is suggested in severe disease, particularly in hematologic malignancy and prolonged neutropenia. (Murray's)
- Combination therapy is also supported in regions with azole resistance prevalence >10% until susceptibility is confirmed. (Murray's)
- Rationale for combining echinocandins + azoles/polyenes: different sites of action (cell wall vs. cell membrane).
C. Surgical Intervention
Indications include:
- Life-threatening hemoptysis
- Lesions contiguous to great vessels or pericardium
- Invasion of chest wall
- Isolated lesions in patients with impending chemotherapy or HSCT (Murray's)
D. Adjunctive Measures
- Granulocyte colony-stimulating factor (G-CSF) or GM-CSF to restore neutrophil function.
- Interferon-gamma (IFN-γ).
- Granulocyte infusions in refractory neutropenic IPA.
- Reduce/discontinue immunosuppression wherever possible (mindful of IRIS risk). (Murray's)
8. Antifungal Prophylaxis
- Posaconazole is the preferred prophylactic agent in high-risk patients (AML/MDS receiving remission induction chemotherapy, allogeneic HSCT recipients with GvHD).
- Itraconazole and voriconazole are alternatives.
- Surveillance serum GM in high-risk patients allows early diagnosis during prophylaxis. (Fishman's)
9. Prognosis and Outcomes
- Overall mortality ~36% at 12 weeks and ~75% at 1 year in HSCT/SOT recipients. (Fishman's)
- Mortality rates of 30-50% in leukemia and HSCT, and up to 90% in untreated disseminated disease.
- Factors worsening prognosis: delayed diagnosis, persistent neutropenia, inability to reduce immunosuppression, azole-resistant Aspergillus, and CNS dissemination.
- Early HRCT with initiation of antifungal therapy at the first sign of halo sign in neutropenic fever has improved outcomes.
Summary Table
| Feature | Detail |
|---|---|
| Causative agent | A. fumigatus (most common), A. flavus, A. terreus (AmB-resistant) |
| Key risk factor | Neutropenia, HSCT, SOT (lung Tx), CGD, chronic steroids |
| Pathology | Angioinvasion → thrombosis → coagulative necrosis |
| Early CT sign | Halo sign (GGO around nodule) |
| Late CT sign | Air-crescent sign (cavitation) |
| Best serum test | Galactomannan (ODI ≥0.5; sens 71%, spec 89%) |
| Gold standard Dx | Histopathology: septate hyphae on GMS/PAS + culture |
| Drug of choice | Voriconazole (IV → oral step-down) |
| Resistant species | A. terreus (AmB-resistant) |
| Mortality | 30-75%; early Rx improves survival |
References:
- Fishman's Pulmonary Diseases and Disorders, 5th Ed., Chapter 132 (Aspergillosis)
- Murray & Nadel's Textbook of Respiratory Medicine, 7th Ed., Chapter 57 (Pulmonary Aspergillosis)
This is a shared conversation. Sign in to Orris to start your own chat.