clinical anatomy pericardiocentesis
Reading File
Finding Sources
Finding Sources
Searching PubMed
pericardiocentesis technique safety
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full clinical anatomy answer.
Pericardiocentesis: Clinical Anatomy
1. Anatomy of the Pericardium
The pericardium is a two-layered fibroelastic sac enclosing the heart and proximal great vessels.
Visceral pericardium (epicardium): A single monolayer of mesothelial cells with underlying collagen and elastin, tightly adherent to the epicardial surface of the heart.
Parietal pericardium: Approximately 2 mm thick, largely acellular, composed of dense collagen and elastin. It has fibrous ligamentous attachments to the diaphragm, sternum, and mediastinal structures.
Pericardial sac (space): Contained between the two layers; normally holds 15-50 mL of serous fluid under slightly negative pressure, which lubricates cardiac motion and acts as a shock absorber.
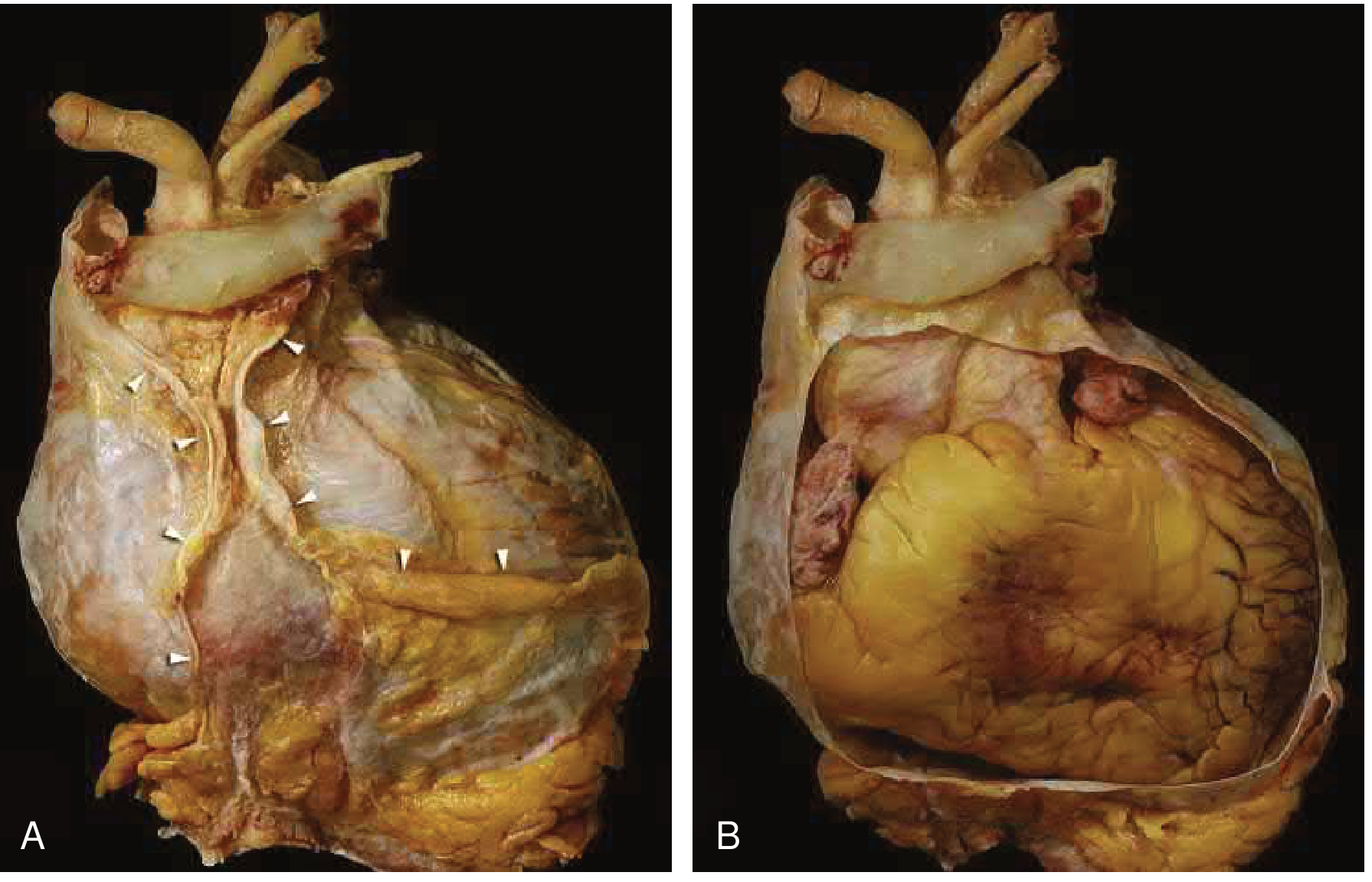
Anterior view (A) of intact parietal pericardium with mediastinal pleural reflections (arrowheads). (B) Pericardium opened, showing the heart and intrapericardial great arteries. - Braunwald's Heart Disease, 15th ed.
Key anatomical reflections:
- The visceral-parietal reflection occurs a few centimeters proximal to the cavoatrial junctions, so portions of the SVC and IVC lie within the pericardial sac
- Posterior to the LA, the reflection creates the oblique sinus - the LA is largely extra-pericardial
- The transverse sinus lies between the aorta/pulmonary trunk anteriorly and the pulmonary veins/atria posteriorly
- Proximal segments of the aorta and pulmonary trunk are intrapericardial
Mechanical properties: At low volumes, the pericardium is compliant (flat pressure-volume curve). Once the reserve volume is exceeded, it becomes abruptly stiff. This is the anatomical basis for why tamponade is so hemodynamically catastrophic once the critical volume threshold is crossed.
2. Physiology of Tamponade - The Pressure-Volume Relationship
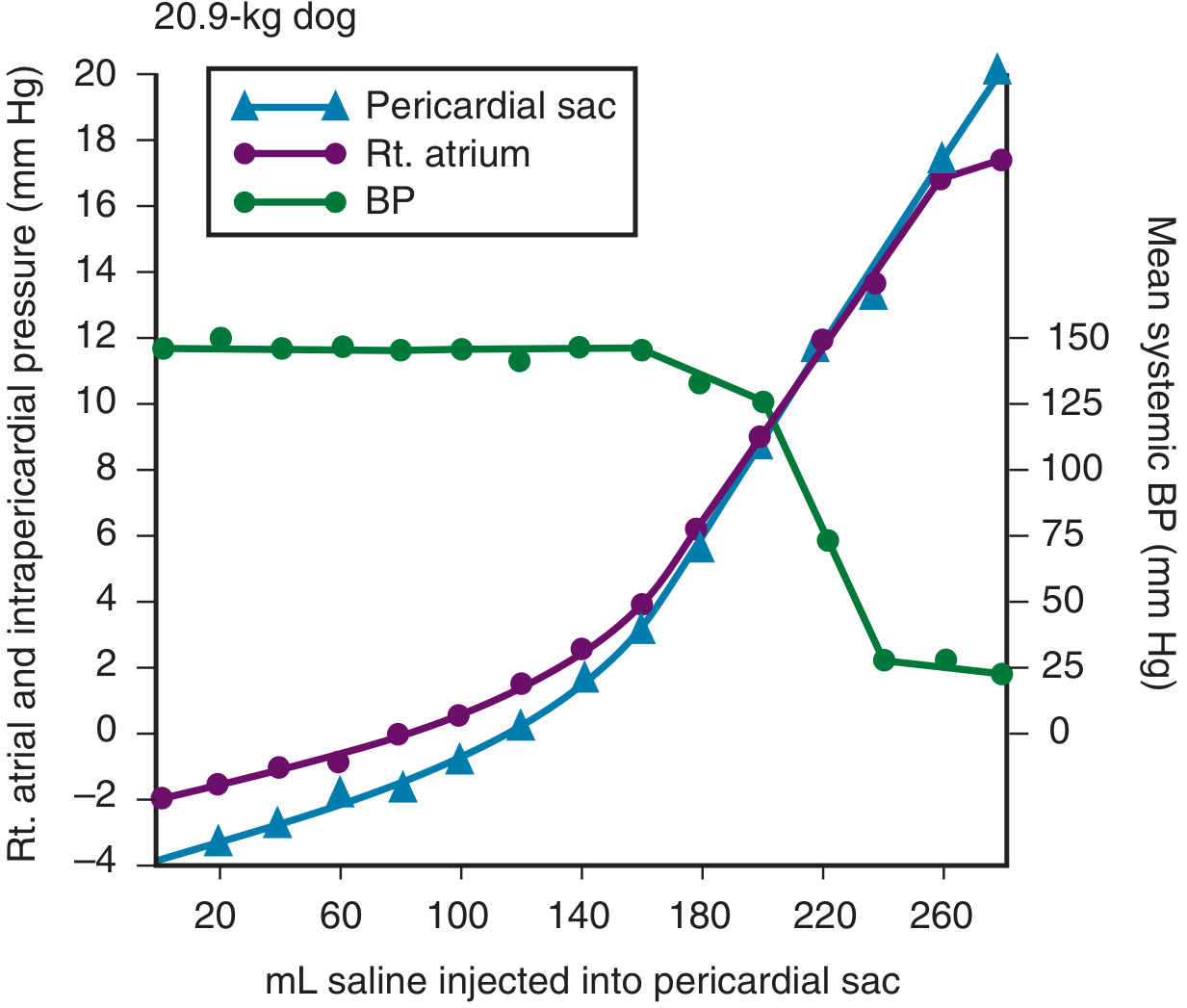
Right atrial pressure and intrapericardial pressure rise steeply once ~200 mL is reached, while BP collapses. Small increments of fluid beyond this point cause large hemodynamic deterioration. Critically, removing even a small volume (20-30 mL) can produce dramatic hemodynamic benefit. - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Acute vs. chronic effusions:
- Acute accumulation: The pericardium can accommodate ~80-120 mL before pressure rises steeply. Beyond ~200 mL, adding as little as 20-40 mL can double intrapericardial pressure
- Chronic accumulation: The pericardium adapts over weeks by stretching, allowing several liters with minimal hemodynamic compromise
- Tamponade typically occurs at intrapericardial pressure of 15-20 mmHg
3. Beck's Triad and Grading
The classic triad (Grade III): hypotension, elevated JVP (JVD), muffled heart sounds
| Grade | Pericardial Volume | MAP | CVP | HR | Beck's Triad |
|---|---|---|---|---|---|
| I | <200 mL | Normal | ↑ | ↑ | Absent |
| II | ≥200 mL | Normal or ↓ | ↑ (≤12 cmH₂O) | ↑ | May be present |
| III | >200 mL | ↓↓ | ↑↑ (30-40 cmH₂O) | ↑ | Usually present |
Additional signs: pulsus paradoxus (>10 mmHg drop in SBP on inspiration, >20 mmHg in moderate-severe tamponade), Kussmaul's sign (paradoxical JVD increase on inspiration).
4. Indications and Contraindications
Indications:
- Therapeutic: Cardiac tamponade with hemodynamic compromise, shock, PEA arrest
- Diagnostic: Determining cause of a pericardial effusion when fluid analysis will alter management; large asymptomatic effusions at risk of progression
Absolute contraindications: None when tamponade is causing hemodynamic instability or arrest.
Relative contraindications:
- Aortic dissection (source of hemopericardium - drainage is dangerous)
- Myocardial rupture (emergent surgery preferred)
- Coagulopathy / thrombocytopenia (platelet count <50 x 10⁹/L: use imaging guidance and non-subcostal window)
- Loculated posterior effusions not accessible percutaneously
- Traumatic hemopericardium (thoracotomy preferred due to 20-40% false-negative rate and tendency to clot)
- Prosthetic heart valves, pacemakers/devices
5. Access Routes and Anatomy of Each Approach
Subxiphoid (Subcostal) Approach - Most Common
Anatomical rationale: The angle between the xiphoid process and the left costal margin (left xiphocostal angle) provides a narrow corridor that avoids the pleural recesses and the cardiac notch of the lung. The needle passes posterior to the costal margin and anterior to the diaphragm.
Needle insertion:
- Skin entry at the left xiphocostal angle, approximately 1-2 cm inferior to the costal margin and just to the left of the xiphoid
- Needle directed at approximately 30-45° to the skin, aimed toward the left shoulder (or left nipple in men)
- The needle passes behind the sternum, below the left costal cartilage, through the diaphragm, and enters the pericardial sac at its inferior aspect
- At 30° angulation, the path goes posterior to the costal margin, avoiding the pleural sinus
Structures at risk:
- Left lobe of the liver (injury risk if needle angled too inferiorly or to the right)
- Internal mammary artery (runs 3-5 cm lateral to the sternal edge - stay medial)
- Intercostal neurovascular bundle (avoid by approaching from below the rib)
- Coronary arteries (especially the right coronary artery in its inferior course)
- Right ventricle (anterior wall most vulnerable - the thinnest chamber)
- Stomach (if needle directed too laterally)
Apical Approach (Echo-Guided)
- Entry at the cardiac apex (5th-6th intercostal space, anterior axillary line)
- Needle angled medially toward the pericardial space, allowing direct ultrasound visualization
- Risk: intercostal vessels (always advance above the superior rib edge), coronary arteries
Parasternal Approach
- Entry at the 4th or 5th intercostal space, left parasternal region, 1-2 cm lateral to sternal edge
- Avoids internal mammary artery (which runs 3-5 cm from the sternum)
- Used less commonly; good for anterior-predominant effusions
6. ECG Guidance (Blind Technique)
The V-lead (precordial alligator clip) technique attaches the ECG lead to the base of the needle:
- ST elevation or current of injury pattern = needle has contacted the ventricular myocardium - withdraw
- PR depression = contact with atrial myocardium - withdraw
- Normal tracing while aspirating fluid = needle in the pericardial space
This technique has largely been replaced by ultrasound guidance, but remains important in crash/arrest scenarios.
7. Procedure Steps (Seldinger Technique)
- Position: Semi-recumbent at 30-45° (tilts fluid anteriorly toward the subxiphoid approach)
- Prep and drape sterile field; local anesthesia with 1% lidocaine down to pericardium
- Insert 18-gauge spinal needle at left xiphocostal angle, angled 30-45° to skin toward left shoulder, aspirating continuously
- Confirm pericardial entry: fluid aspirates freely; if using ECG monitoring, waveform remains normal; if using ultrasound, agitated saline confirms position
- Introduce J-tipped guidewire through the needle into the pericardial sac
- Remove needle over guidewire, pass dilator, then pigtail catheter (Seldinger technique)
- Aspirate fluid with 60 mL syringe; drain completely or leave pigtail catheter for ongoing drainage
- Send fluid for cell count, cytology, culture, LDH, protein, glucose, pH, specific markers
Distinguishing pericardial from ventricular blood: Pericardial blood (old/serous) often does not clot and has a lower hematocrit. If bright red blood is aspirated, inject contrast under fluoroscopy or agitated saline under echo to confirm position before proceeding.
8. Guidance Modalities
| Modality | Advantages | Limitations |
|---|---|---|
| Blind | Bedside, no equipment needed, fastest in arrest | No position confirmation, subxiphoid only, high complication rate |
| Echocardiography | Portable, real-time, multiple access sites, visualizes chambers | Nondiagnostic windows (pneumopericardium, obesity), posterior loculations |
| Fluoroscopy | Confirms position with contrast, widely available | Not portable, radiation, contrast, subxiphoid only |
| CT-guided | Unlimited access sites, best anatomy | Not bedside, radiation, not for emergencies |
Echocardiography is the current gold standard for elective and semi-urgent pericardiocentesis. The optimal access site is where the effusion is largest and the target heart structure is most distant from the needle path.
9. Complications
Procedure-related:
- Dysrhythmias (most common - vasovagal, VT/VF if myocardium contacted)
- Right ventricular puncture/laceration (most common chamber injured - thin anterior wall)
- Coronary artery laceration or puncture (especially RCA inferiorly)
- Internal mammary artery injury
- Intercostal vessel or nerve injury
- Hemothorax / pneumothorax / pneumopericardium
- Air embolism
- Intra-abdominal injury (liver, stomach)
Post-procedure:
- Fluid reaccumulation (reason to leave indwelling catheter)
- Suppurative pericarditis (septic complication)
- Acute pulmonary edema (re-expansion after tamponade relief - rare)
Success rate with echo guidance: >95%; complication rate significantly lower than blind technique.
10. Diagnostic Value of Pericardial Fluid
| Fluid Characteristic | Significance |
|---|---|
| Low pH (<7.0) | Inflammatory/infectious etiology |
| Exudate (LDH, protein elevated) | Neoplasm, infection, inflammation |
| Cytology positive | Malignant effusion |
| Culture + Gram stain | Bacterial/TB pericarditis |
| Adenosine deaminase elevated | Tuberculosis |
| CEA elevated | Malignancy |
| Hemorrhagic, does not clot | Usually old blood/neoplastic |
| Bright red, clots | Ventricular puncture (withdraw!) |
Overall diagnostic yield from pericardial fluid alone is approximately 24% for determining a specific etiology; pericardial biopsy (via subxiphoid pericardiotomy/window) significantly improves yield.
Sources:
- Braunwald's Heart Disease, 12th ed. - Anatomy and Physiology of the Pericardium
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, 7th ed.
- Fuster and Hurst's The Heart, 15th ed.
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
Recent evidence note: A 2025 systematic review (PMID 40901363) specifically examined pericardiocentesis safety in pulmonary arterial hypertension, confirming the relative contraindication status and highlighting that it remains a significant procedural risk in this population.
This is a shared conversation. Sign in to Orris to start your own chat.