Sailogram and sialendoscopy. Ms ent University exam pattern for 10 marks each. With relevant diagrams.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive material from Cummings Otolaryngology for both topics with all key images. Let me compose the full exam-pattern answers.
SIALOGRAPHY (SIALOGRAM)
10-Mark University Exam Answer - MS ENT
Definition
Sialography is a radiological technique used to visualize the ductal system of the major salivary glands (parotid and submandibular) by injecting radiopaque contrast material into the duct opening. It provides the best detail of the intraglandular ductal architecture and is particularly useful for obstructive and inflammatory duct pathology.
Anatomy Relevant to Sialography
| Duct | Length | Caliber | Orientation |
|---|---|---|---|
| Stensen (Parotid) | 6-7 cm | 1-2 mm | Horizontally oriented |
| Wharton (Submandibular) | ~5 cm | 1-3 mm | Angles downward 45° to sagittal/axial planes; courses around mylohyoid |
The Wharton duct papilla is smaller, more difficult to cannulate, and the duct itself is easier to perforate. The submandibular duct is longer, more tortuous, and runs against gravity - factors that predispose it to salivary stasis and stone formation.
Indications
- Sialolithiasis (salivary calculi/stones)
- Ductal stenosis - localized narrowing of the duct
- Chronic sialadenitis - to assess ductal irregularities and strictures
- Sjogren syndrome - to detect punctate/globular contrast pooling (sialectasia)
- Salivary fistula - to delineate fistulous tract
- Pre-/post-irradiation assessment - xerostomia evaluation
- Recurrent parotitis - recurrent juvenile parotitis
Contraindications
- Acute sialadenitis - may exacerbate infection or cause ascending infection (most important)
- Iodine contrast allergy
- Stones in the oral portion of the Wharton duct - risk of stone impaction
- Active infection in the gland
Equipment
- Blunt-tipped sialographic cannula with attached tubing
- Lacrimal dilators (for dilating the papilla if needed)
- Water-soluble contrast agent: diatrizoate meglumine (iodinated, water-soluble - no adverse effects if duct perforation occurs)
- Fluoroscopy unit
- Secretagogue: lemon juice (to stimulate salivary flow for post-evacuation films)
Technique
Step 1 - Patient preparation: The mucosa around the papilla is dried.
Step 2 - Stimulation of salivary flow: The gland is massaged or a secretagogue (lemon juice) is applied to identify the duct orifice.
Step 3 - Cannulation: A blunt-tipped sialographic cannula is introduced into the duct papilla. Lacrimal dilators may be needed to enlarge the papilla opening.
Step 4 - Contrast injection:
- Stensen duct: approximately 1 mL of contrast
- Wharton duct: approximately 0.5 mL of contrast
- Injected slowly under fluoroscopic guidance to avoid overfilling and perforation
Step 5 - Imaging: Images taken in anteroposterior, lateral, and oblique projections to optimize ductal visualization.
Step 6 - Emptying/evacuation phase: The patient is given sialagogue (lemon juice); films taken to assess ductal drainage and clearance.
Step 7 (Optional): Post-sialographic CT for precise localization of abnormalities within the gland.
Contrast Agents
- Water-soluble agents (diatrizoate meglumine): Preferred. Cause no adverse effects even if duct perforation occurs.
- Oil-based agents (Lipiodol): Historical use; now rarely used due to risk of lipid granuloma if extravasated.
Normal Sialographic Appearances
- Smooth, regular duct with gradual tapering of intraglandular branches ("bare tree in winter" appearance)
- No filling defects, no strictures, no pooling of contrast
Pathological Findings
| Condition | Sialographic Appearance |
|---|---|
| Sialolithiasis | Filling defect within duct; proximal ductal dilatation |
| Ductal stricture | Focal narrowing with pre-stenotic dilatation |
| Chronic sialadenitis | Multifocal wall irregularities, "sausage-link" duct |
| Sjogren syndrome | Punctate, globular, cavitary or destructive pattern of contrast pooling (sialectasia) |
| Salivary fistula | Contrast extravasation through fistulous tract |
MR Sialography
First reported in 1996. Uses a heavily T2-weighted sequence to depict ductal system. Saliva itself acts as the endogenous contrast medium (no injection required - non-invasive).
Advantages over conventional sialography:
- Non-invasive - no cannulation required
- No radiation
- Safe in acute sialadenitis (where conventional sialography is contraindicated)
- Safe for patients with iodine allergy
- Excellent for Sjogren syndrome evaluation, ductal stenosis, post-irradiation xerostomia
- Can detect radiolucent stones
Limitation: Difficult to perform in young children; pathological diagnosis can be difficult; ductal metaplasia of sialolithiasis may be misinterpreted as mucoepidermoid carcinoma.
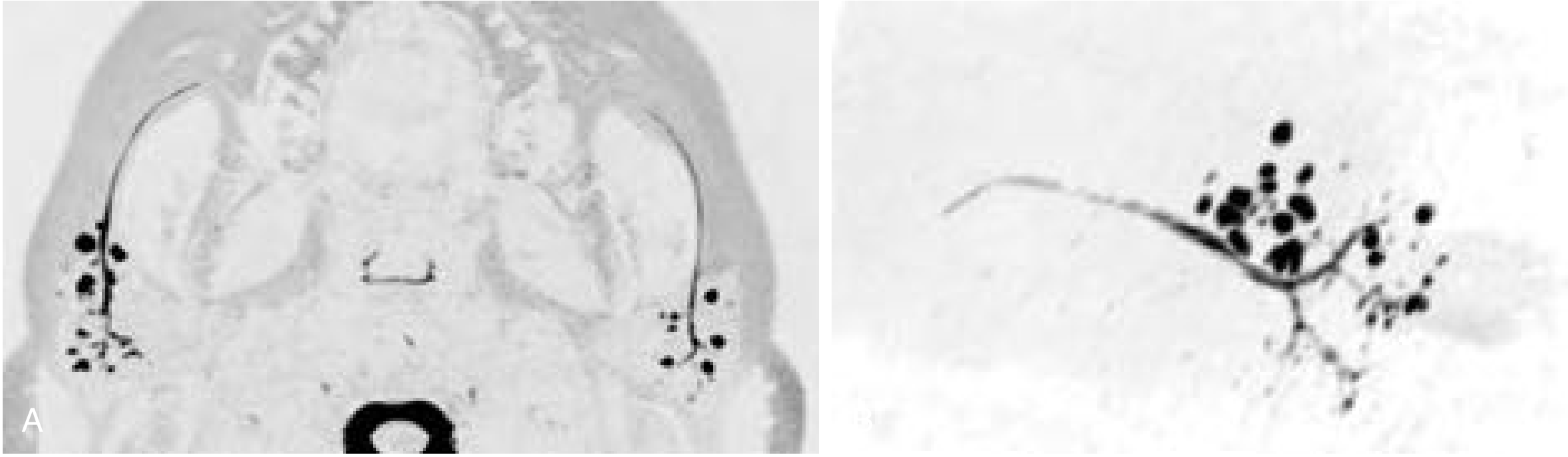
MR sialogram (A) axial source images showing cystic dilation of terminal intraparotid ducts in Sjogren syndrome; (B) 3D reconstruction demonstrating ductal anatomy. - Cummings Otolaryngology
Complications of Sialography
- Local pressure/pain - most common; typically resolves within 24 hours
- Ductal perforation - especially Wharton duct
- Post-sialographic infection - ascending sialadenitis
- Contrast allergy - rare with water-soluble agents
- Stone impaction - if stone is in oral portion of duct
CT Sialography
CT with bony windowing is highly effective for sialolithiasis. Multiple hyperdense stones within the submandibular gland and Wharton duct are visible as bright (hyperdense) foci, with associated gland enlargement.
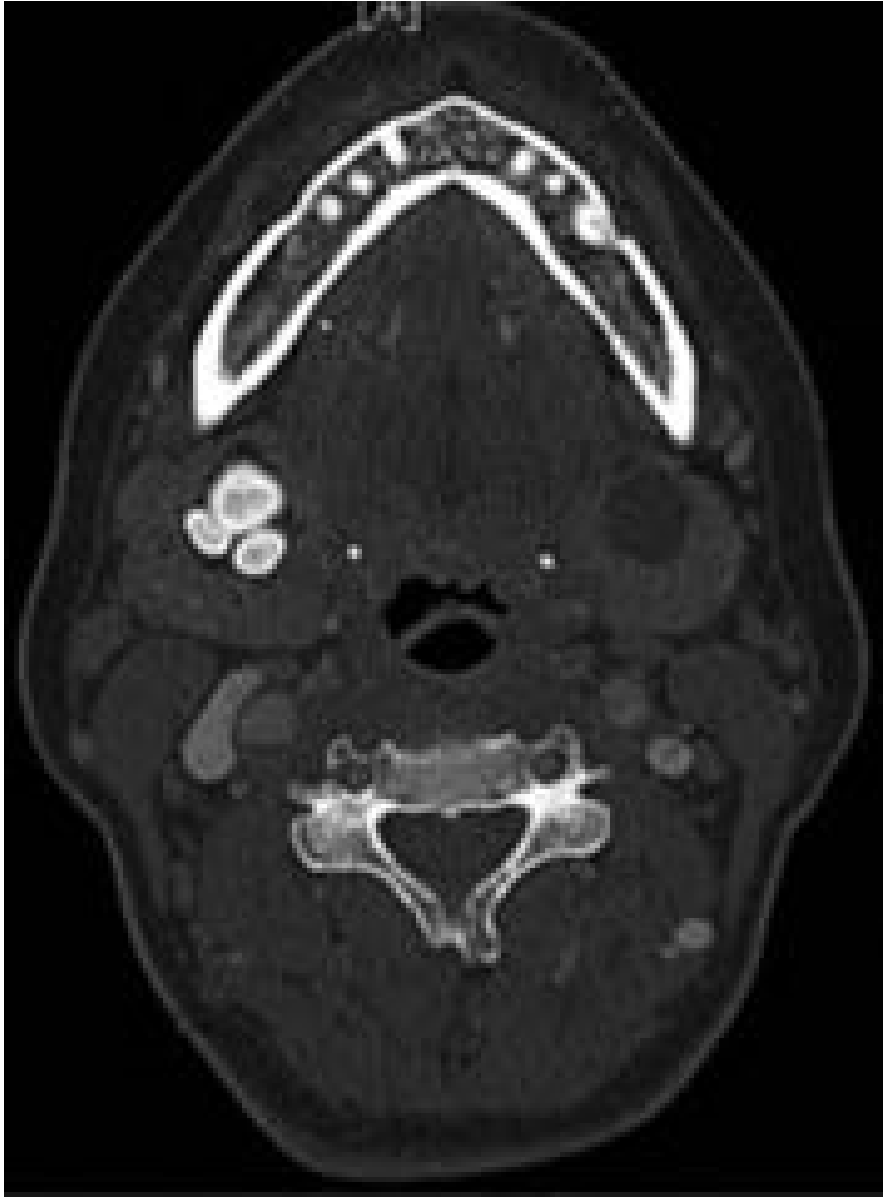
CT (bony window) showing multiple hyperdense sialoliths in the right submandibular gland - Cummings Otolaryngology
Digital Subtraction Sialography
- Lessens interference from surrounding bony structures
- Detects radiolucent stones with sensitivity of 95-100%
- Reserved for complex cases
Summary - Role in Current Practice
Conventional sialography has been largely replaced by CT and MRI for most salivary gland pathology. However, it remains the gold standard for depicting fine intraglandular ductal branches. CT/ultrasound are first-line for sialolithiasis. MR sialography, digital sialography, and 3D reconstruction for virtual sialendoscopy are reserved for complex cases.
SIALENDOSCOPY
10-Mark University Exam Answer - MS ENT
Definition
Sialendoscopy is a minimally invasive endoscopic technique used for the diagnosis and treatment of obstructive and inflammatory salivary gland disorders. It allows direct visualization of the ductal system using miniature semirigid or rigid endoscopes introduced through the natural ductal papilla. It represents a paradigm shift from extirpative to gland-preserving surgery.
Historical Background
Sialendoscopy was first introduced in the early 1990s. Advances in miniaturized fiber-optics and instrumentation have allowed endoscopes as small as 0.8 mm to be used safely in adults and children alike.
Indications
- Sialolithiasis (salivary duct stones) - most common adult indication
- Juvenile recurrent parotitis (JRP) - most common pediatric indication (68.9% of pediatric cases)
- Chronic sialadenitis - obstructive or inflammatory
- Ductal stenosis (congenital or acquired)
- Sjogren syndrome - ductal assessment and intraductal steroid instillation
- Salivary gland swelling of unclear etiology after failed imaging
- Localization of stones undetected by other imaging modalities
Contraindications
- Active acute sialadenitis with significant floor-of-mouth induration
- Very distal duct stones (accessible by simple transoral milking)
- Patients unable to cooperate (relative - can use general anesthesia)
Instrumentation
Types of Sialendoscopes
1. Diagnostic endoscopes: Equipped with fiber-optic light, image transmission, and irrigation channel. Do NOT allow intraductal instrumentation.
2. Therapeutic endoscopes: Two types:
- Compact (single-unit): Fiber light + fiber image transmission + working channel + irrigation channel in one unit. Cannot be disassembled.
- Modular (semirigid): Optical fibers in a probe introduced into sheaths of various sizes; gap between probe and sheath = irrigation channel.
Karl Storz Erlangen Mini-Sialendoscope Sizes
| Size | Components |
|---|---|
| 0.8 mm | Lens + irrigation channel only |
| 1.1 mm | Lens + irrigation + working channel |
| 1.6 mm | Lens + irrigation + working channel (may be too large for some children) |
The working channel allows introduction of:
- Microdrill and holmium laser fiber (fragment large stones)
- Balloon dilator (ductal stenosis)
- Wire basket (stone fragment extraction)
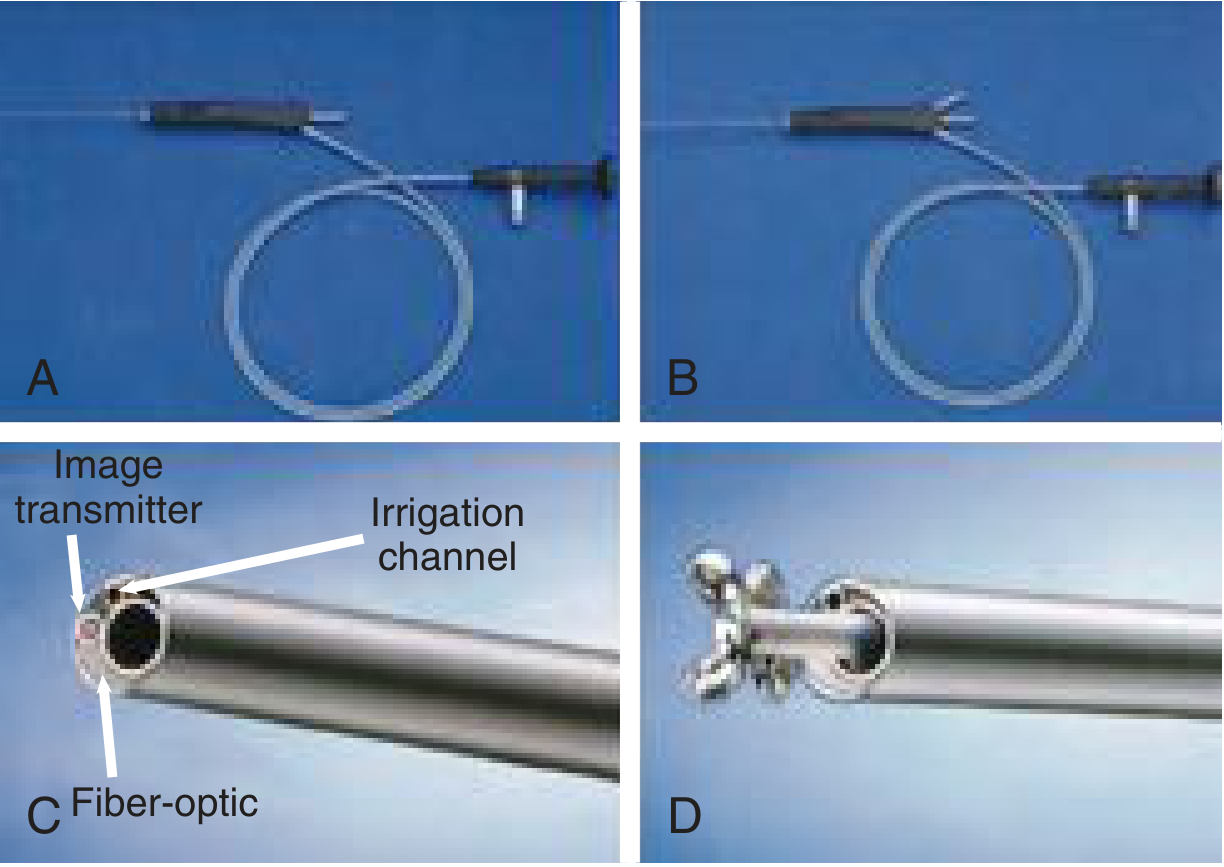
Modular sialendoscope: (A) single-channel, (B) dual-channel, (C) cross-section showing image transmitter, irrigation channel, fiber-optic; (D) wire basket instrument - Cummings Otolaryngology
Anesthesia
- Children < 8 years: General anesthesia
- Children > 8 years (cooperative) and adults: Can be performed under local anesthesia
- A bite block is placed on the contralateral side
Operative Technique (Step-by-Step)
Step 1 - Identification of duct papilla:
The papilla of the Stensen duct (parotid) or Wharton duct (submandibular) is identified. The gland is massaged to produce saliva to identify the opening.
Step 2 - Serial dilation:
The papilla and duct orifice are dilated using salivary duct probes and dilators in progressive sizes (tapered metal dilators/lacrimal probes). This is the most critical step to allow endoscope entry without ductal injury.
Step 3 - Introducer sheath placement:
An introducer sheath is placed in the dilated orifice to facilitate scope entry and repeated introduction/withdrawal.
Step 4 - Endoscope introduction:
The sialendoscope (attached to camera and monitor) is introduced via the dilated orifice under continuous saline irrigation to distend the duct and improve visualization.
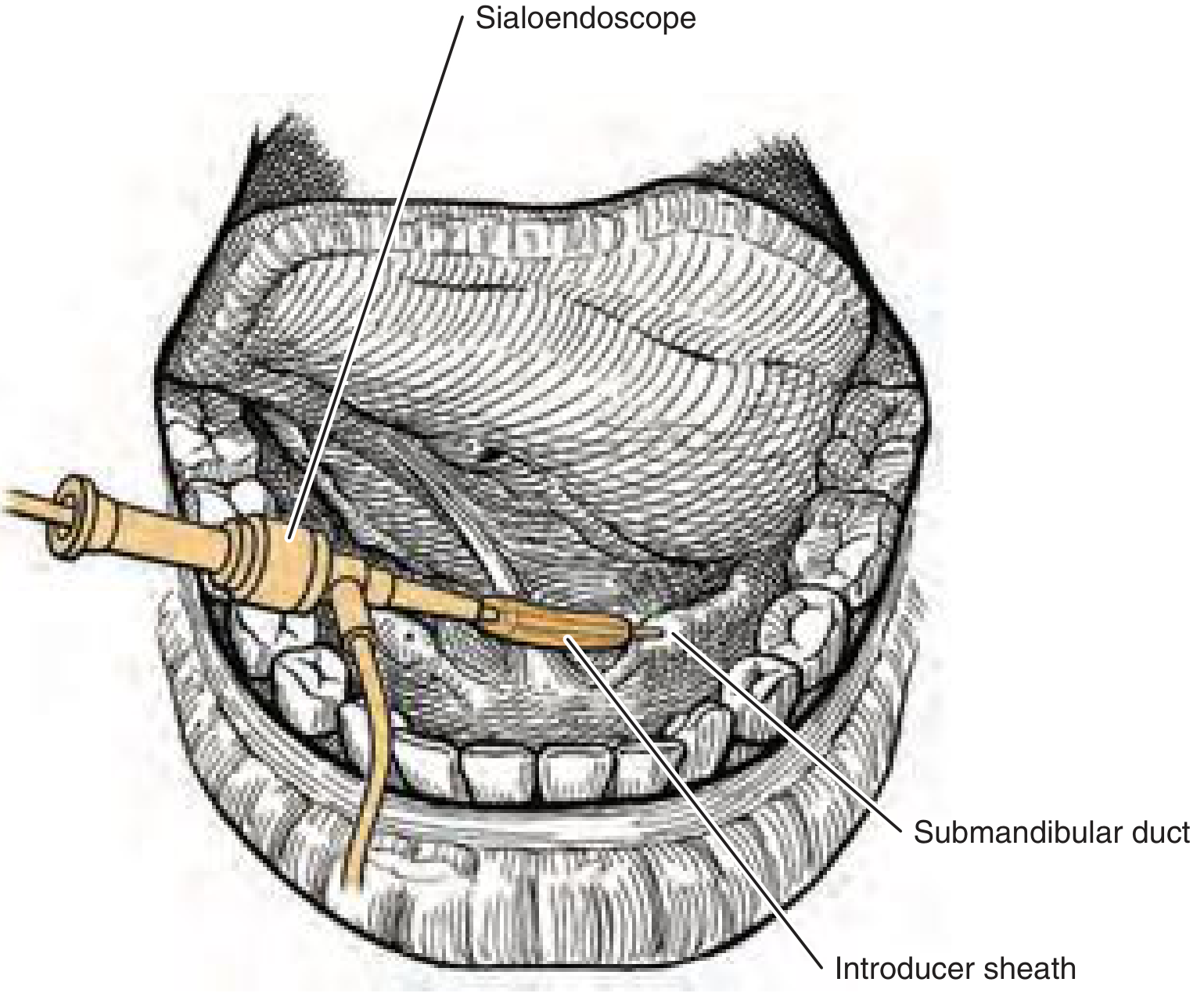
Diagram showing sialendoscope inserted via introducer sheath into the Wharton duct - Cummings Otolaryngology
Step 5 - Ductal exploration:
The scope is advanced to the first branching point and each branch is examined as far as the scope can comfortably pass. The ductal mucosa, any stones, strictures, or inflammatory changes are documented.
Step 6 - Therapeutic intervention (if needed):
| Stone size/situation | Technique |
|---|---|
| Small mobile stone | Wire basket - ensnare and extract directly |
| Large/impacted stone | Holmium laser or pneumatic lithotripsy to fragment first, then basket retrieval |
| Ductal stenosis | Pneumatic balloon dilation |
| Post-procedure | Salivary stent left in situ for 2-4 weeks to prevent restenosis |
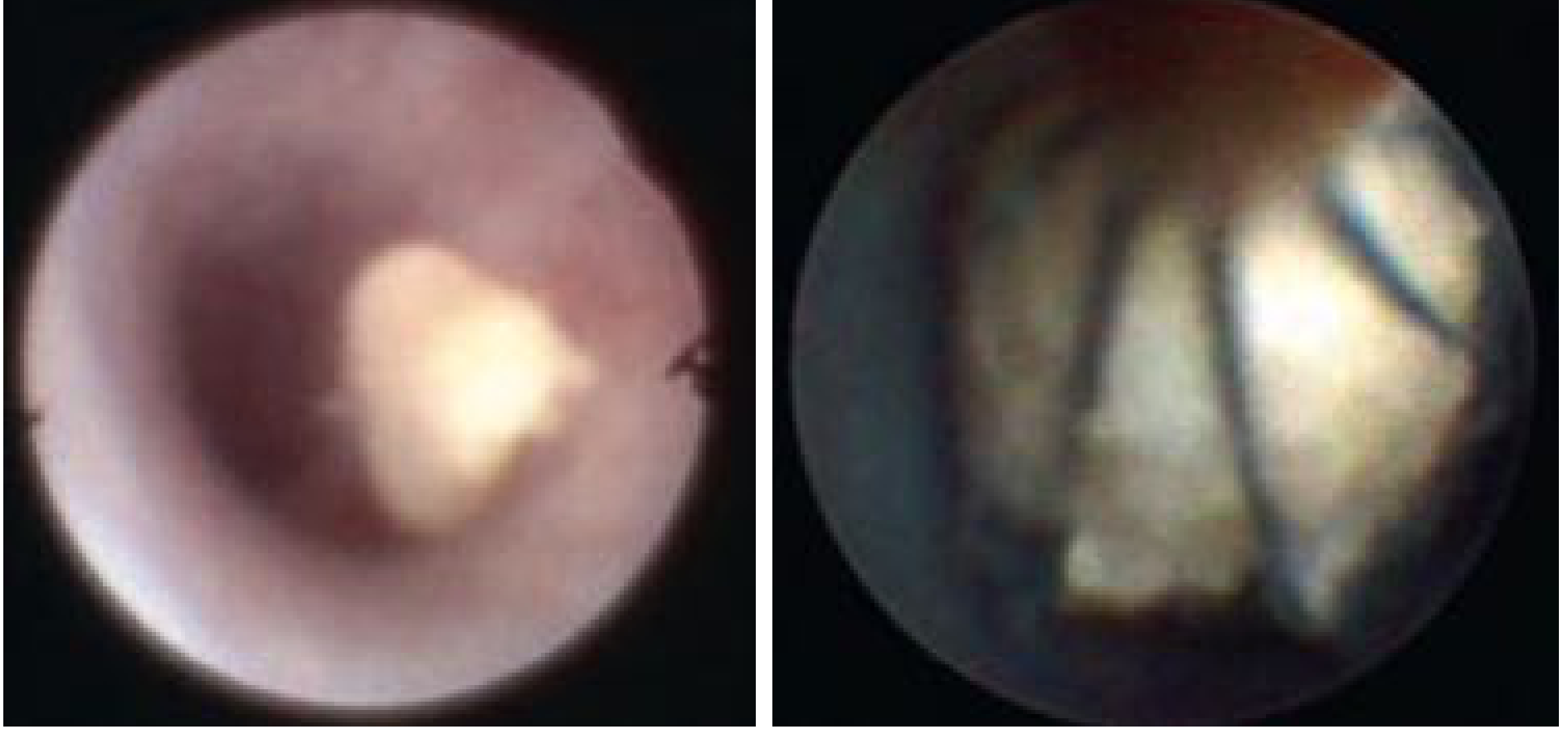
Sialendoscopic view: (left) stone seen within the duct; (right) wire basket ensnaring the stone for removal - Cummings Otolaryngology
Step 7 - Wire basket with extracted stone:

Stone-extractor wire basket containing a submandibular stone removed by sialendoscopy - Cummings Otolaryngology
Combined (Hybrid) Approach
When the stone is:
- Too large for endoscopic removal alone
- Impacted and inaccessible
A combined approach is used:
- The stone is localized endoscopically or by ultrasound
- A small incision is made into the duct (intraoral or external) over the stone under direct or endoscopic vision
- Submandibular stones: Removed via intraoral incision over the floor of mouth
- Parotid (proximal/hilar) stones: May require partial parotidectomy incision and SMAS flap elevation
Success rates with combined techniques: 80-100%
Advantages of Sialendoscopy Over Traditional Surgery
| Feature | Sialendoscopy | Traditional (gland excision) |
|---|---|---|
| Gland preservation | Yes | No (gland removed) |
| Invasiveness | Minimal | Major surgery |
| Anesthesia | Local/GA | GA |
| Risk to facial/lingual nerve | Minimal | Significant |
| Recovery | Rapid | Prolonged |
| Diagnostic + therapeutic | Both in one | Separate |
Specific Applications
Juvenile Recurrent Parotitis (JRP)
Most common pediatric indication (68.9%). Sialendoscopy allows ductal irrigation with saline + corticosteroids and can visualize and dilate any strictures - achieving long-term remission in many children.
Sjogren Syndrome
Intraductal instillation of corticosteroids via the sialendoscope can reduce glandular inflammation and improve salivary flow.
Pediatric Sialolithiasis (14.7% of pediatric sialendoscopy cases)
Allows gland-preserving stone removal without the morbidity of excisional surgery in children.
Complications
- Ductal perforation - most common (false passage creation during dilation)
- Post-operative edema and transient swelling of the gland
- Restenosis of the duct (prevented by leaving a stent)
- Infection - post-procedure sialadenitis
- Incomplete stone removal - requiring repeat procedure or combined approach
- Avulsion of the papilla - if excessive force used during dilation
Outcomes
- Success rate for stone removal: 80-100% (combined endoscopic + open techniques)
- Gland preservation rate: High; avoids need for submandibulectomy or parotidectomy in most cases
- Sialendoscopy is now considered a potential gold standard for investigation and treatment of many salivary gland pathologies
Key Differences: Sialography vs Sialendoscopy
| Feature | Sialography | Sialendoscopy |
|---|---|---|
| Nature | Radiological (imaging) | Endoscopic (surgical) |
| Purpose | Mainly diagnostic | Diagnostic + therapeutic |
| Invasion | Cannulation + contrast | Scope + instruments |
| View | X-ray silhouette of duct | Direct internal view |
| Stone treatment | No (imaging only) | Yes (basket, laser, lithotripsy) |
| Use in acute sialadenitis | Contraindicated | Relatively contraindicated |
| Contrast allergy risk | Yes (iodine) | None |
| MR variant | MR sialography available | No equivalent |
Sources: Cummings Otolaryngology Head and Neck Surgery, 7th Edition, Chapters 82, 83 and 205
This is a shared conversation. Sign in to Orris to start your own chat.