Q. Define Vertigo, enumerate the causes of vertigo. How will you manage BPPV in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Now I have comprehensive material from textbooks. Let me compose the full 50-mark answer:
VERTIGO — DEFINITION, CAUSES, AND MANAGEMENT OF BPPV
(50-Mark Answer | RGUHS Standard)
PART I: DEFINITION OF VERTIGO
Vertigo is defined as an illusory or hallucinatory sense of movement — either of the self (subjective vertigo) or of the environment (objective vertigo) — resulting from a mismatch between vestibular, visual, and proprioceptive sensory inputs to the brain.
"Vertigo is a sense of spontaneous movement, usually described as spinning. It may be described as an internal or external sense of movement. Distress comes from the mismatch between the vestibular, proprioceptive, and visual inputs to the brain." — Cummings Otolaryngology Head and Neck Surgery
Key distinctions:
| Term | Definition |
|---|---|
| Vertigo | Illusion of rotatory / linear movement |
| Dizziness | Vague sense of imbalance, lightheadedness |
| Disequilibrium | Unsteadiness without a sensation of movement |
| Pre-syncope | Faintness due to reduced cerebral perfusion |
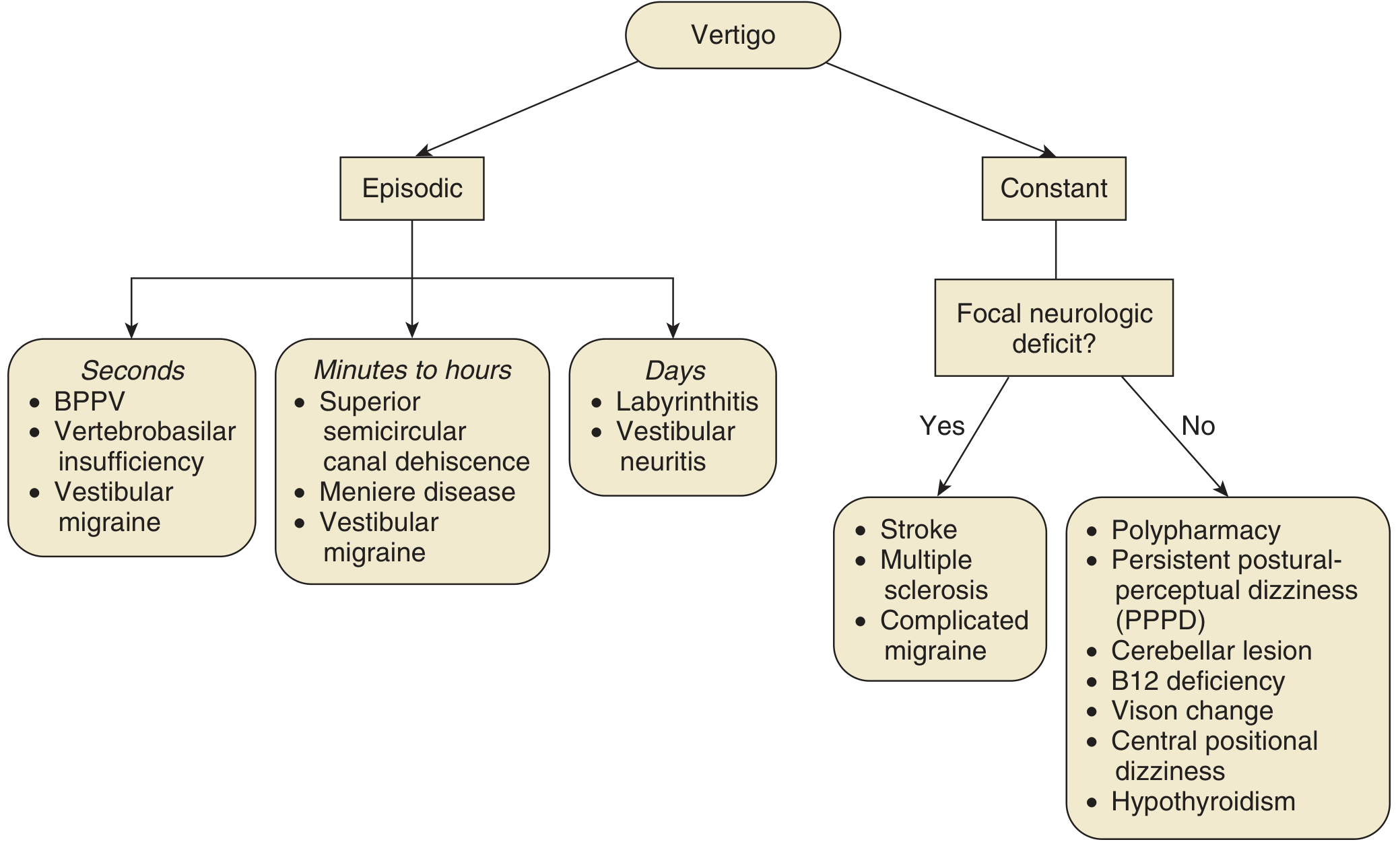
PART II: CLASSIFICATION AND CAUSES OF VERTIGO
A. PERIPHERAL CAUSES (Labyrinthine / Vestibular Nerve)
1. Episodic (Seconds)
- Benign Paroxysmal Positional Vertigo (BPPV) ← most common
- Vertebrobasilar insufficiency
- Vestibular migraine (positional component)
2. Episodic (Minutes to Hours)
- Ménière disease (endolymphatic hydrops)
- Superior semicircular canal dehiscence (SSCD)
- Vestibular migraine
- Perilymphatic fistula
3. Episodes Lasting Days
- Acute labyrinthitis (viral/bacterial)
- Vestibular neuritis (neuronitis)
- Herpes zoster oticus (Ramsay Hunt syndrome)
4. Chronic/Continuous Peripheral Causes
- Acoustic neuroma (vestibular schwannoma)
- Ototoxicity (aminoglycosides, loop diuretics, cisplatin)
- Temporal bone fracture
- Chronic otitis media with labyrinthine fistula
- Otosclerosis
B. CENTRAL CAUSES
| With Focal Neurologic Deficit | Without Focal Neurologic Deficit |
|---|---|
| Brainstem / cerebellar stroke | Persistent Postural-Perceptual Dizziness (PPPD) |
| Multiple sclerosis (demyelinating plaques) | Cerebellar lesion (neoplasm) |
| Complicated migraine | B12 deficiency |
| Posterior fossa tumours | Hypothyroidism |
| Vertebrobasilar TIA | Polypharmacy / drug-induced |
C. SYSTEMATIC CLASSIFICATION (Mnemonic: IDEM)
| Category | Examples |
|---|---|
| Infective | Labyrinthitis, Vestibular neuritis, Otitis media, Ramsay Hunt |
| Degenerative / Vascular | BPPV, Ménière, Vertebrobasilar insufficiency, Stroke |
| External / Toxic | Aminoglycosides, alcohol, anticonvulsants, heavy metals |
| Miscellaneous | Acoustic neuroma, temporal bone fracture, MS, epilepsy |
DIFFERENTIAL DIAGNOSIS FLOWCHART (Cummings, Fig. 137.5)
PART III: BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV)
A. DEFINITION AND HISTORICAL BACKGROUND
BPPV is the most common peripheral vestibular disorder, characterised by brief, recurrent, severe episodes of vertigo triggered by specific head movements, typically lasting <1 minute, associated with characteristic nystagmus.
Historical Milestones:
- 1921 — Bárány: First described BPPV; identified vertical-torsional nystagmus, brief duration, and fatigability
- 1952 — Dix and Hallpike: Described the provocative positioning manoeuvre; identified the offending labyrinth; established cardinal features
- 1969 — Schuknecht: Proposed cupulolithiasis theory — otoconial deposits on the cupula of the posterior semicircular canal
- 1979 — Hall, Ruby, McClure: Proposed canalithiasis as the dominant mechanism — free-floating debris within the posterior canal lumen
- 1992 — Epley: Introduced the Canalith Repositioning Procedure (CRP)
B. INCIDENCE AND EPIDEMIOLOGY
- Most common cause of vertigo in otolaryngology practice: 17–40% of all peripheral vestibular disease (Cummings)
- Incidence: 64 per 100,000 population (Minnesota study); 10.7–17.3/100,000 (Japan)
- Peak age: 4th–5th decade; twice as common in women
- Increases with age; associated with migraine in children
- ~25% attributable to identifiable cause
C. PATHOPHYSIOLOGY
Two Mechanisms:
┌─────────────────────────────────────────────────────────────┐
│ PATHOPHYSIOLOGY OF BPPV │
├─────────────────────┬───────────────────────────────────────┤
│ CANALITHIASIS │ CUPULOLITHIASIS │
│ (90% of cases) │ (10% of cases) │
├─────────────────────┼───────────────────────────────────────┤
│ Free-floating debris│ Dense deposits FIXED to cupula │
│ within canal lumen │ of posterior semicircular canal │
│ │ │
│ → Gravity causes │ → Cupula becomes gravity-sensitive │
│ endolymph flow │ (like an otolith organ) │
│ → Cupula deflection │ │
│ → Transient (< 60s) │ → Sustained (> 60s) nystagmus │
│ → Fatigable │ → Non-fatigable nystagmus │
└─────────────────────┴───────────────────────────────────────┘
Mechanism of nystagmus in canalithiasis (posterior canal BPPV):
- Latency (2–5 sec): Time for free debris to initiate movement
- Brief duration (< 60 sec): Time for debris to settle at lowest point
- Up-beating + torsional nystagmus (superior poles toward affected ear): stimulation of posterior canal nerve
- Reversal on sitting up: retrograde debris movement → ampulopetal cupula deflection
- Fatigability: dispersion of debris with repeated testing
D. AETIOLOGY / PREDISPOSING FACTORS
CAUSES OF BPPV
│
┌────────────────┼──────────────────┐
▼ ▼ ▼
IDIOPATHIC TRAUMATIC SECONDARY
(48–50%) (~25%) (~25%)
│ │
┌──────────┘ ┌───────────┼──────────────┐
│ ▼ ▼ ▼
Head injury Vestibular Ménière Post-surgical
neuritis disease (stapedectomy,
(15% BPPV) cochlear
implant,
dental work)
Prolonged bed rest
Migraine-related ischemia
E. CLINICAL FEATURES
History (85% of diagnostic value — Cummings):
- Severe vertigo with specific head movements:
- Rolling over in bed (most common)
- Looking up / tilting head back (e.g., changing a light bulb)
- Bending forward and rising
- Rapid head turn
- Duration: seconds, never > 1 minute
- Episodes clustered with remissions lasting months
- Patient often identifies specific offending side
- Accompanying: nausea, vomiting (rarely), chronic background unsteadiness
- No hearing loss, tinnitus, aural fullness (distinguishes from Ménière)
F. DIAGNOSIS
1. DIX-HALLPIKE MANOEUVRE (Gold Standard for Posterior Canal BPPV)
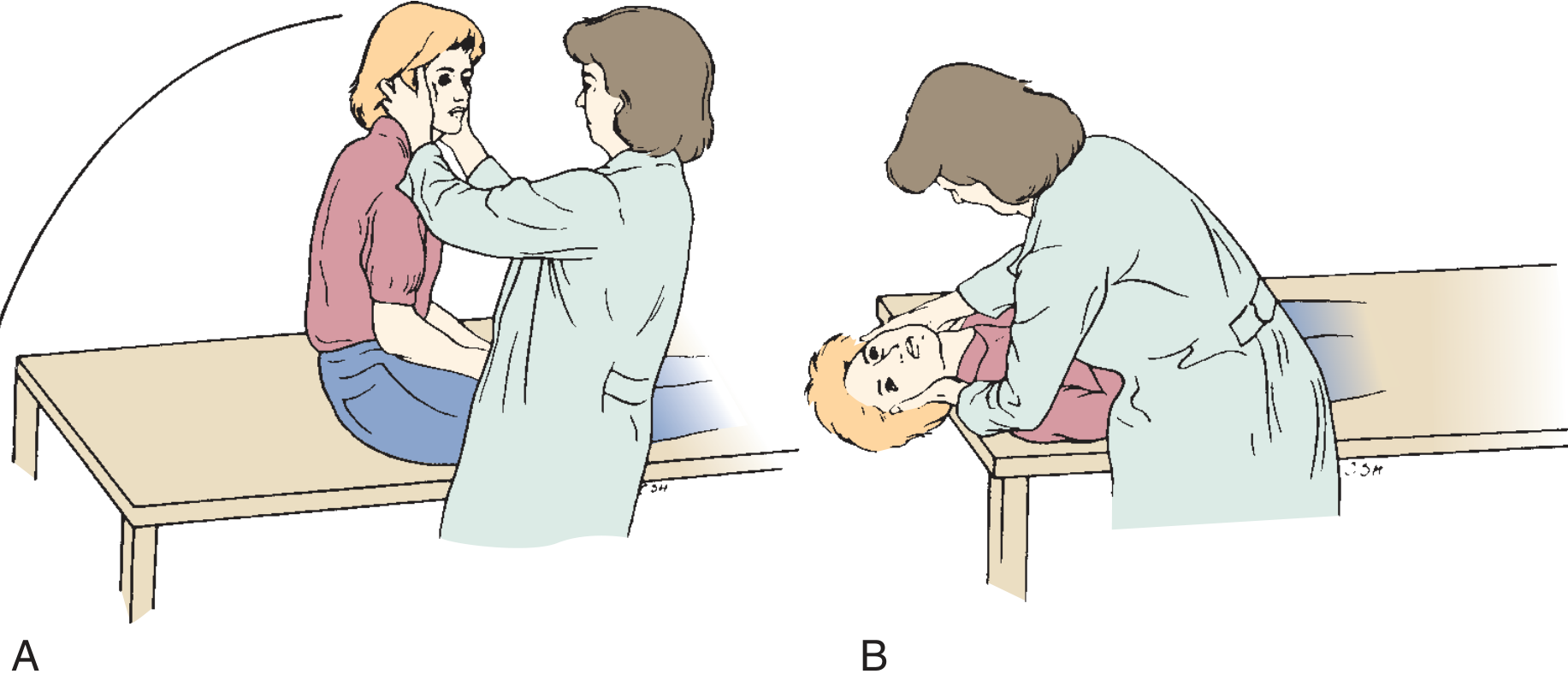
Steps of Dix-Hallpike:
- Patient seated on examination table, head turned 45° to the tested side
- Clinician supports head; rapidly moves patient to supine with head 30° below horizontal
- Observe eyes for nystagmus (use Frenzel lenses ideally)
- Wait 30–40 seconds; return patient to sitting; note reversal
- Repeat for opposite side
Classical Features of Positive Dix-Hallpike (Posterior Canal BPPV):
| Feature | Characteristic |
|---|---|
| Latency | 2–5 seconds |
| Direction | Upbeating + torsional (toward affected ear / lowermost ear) |
| Duration | < 60 seconds |
| Fatigability | Yes (with repeated testing) |
| Reversibility | Yes (nystagmus reverses on sitting up) |
Peripheral vs Central BPPV: Key Differentiators
| Feature | Peripheral | Central |
|---|---|---|
| Latency | 2–5 sec | Immediate |
| Fatiguability | Yes | No |
| Duration | < 60 sec | > 60 sec or sustained |
| Direction | Fixed, torsional | Direction-changing |
| Neurologic signs | Absent | Present |
2. For HORIZONTAL CANAL BPPV — Supine Roll Test (Pagnini-McClure test)
- Patient supine, head rapidly rotated 90° to each side
- Geotropic nystagmus (toward ground) = canalithiasis
- Apogeotropic nystagmus (away from ground) = cupulolithiasis
G. MANAGEMENT OF BPPV
┌────────────────────────────────────────────────────────────────┐
│ BPPV MANAGEMENT ALGORITHM │
│ │
│ Patient presents with positional vertigo │
│ │ │
│ ▼ │
│ Detailed History + Examination │
│ │ │
│ ┌──────────┴──────────┐ │
│ ▼ ▼ │
│ Dix-Hallpike Supine Roll Test │
│ (Posterior canal) (Horizontal canal) │
│ │ │ │
│ ▼ ▼ │
│ Positive? Positive? │
│ (Upbeat +torsional) (Geotropic/Apogeotropic) │
│ │ │ │
│ ▼ ▼ │
│ Posterior Canal BPPV Horizontal Canal BPPV │
│ │ │ │
│ ▼ ▼ │
│ EPLEY MANOEUVRE BARBECUE ROTATION │
│ (1st line) or GUFONI MANOEUVRE │
│ │ │
│ Resolved? │
│ Yes → Reassure + activity │
│ No → Repeat (up to 3×) or SEMONT manoeuvre │
│ │ │
│ Still refractory? │
│ → Brandt-Daroff exercises + Vestibular rehab │
│ │ │
│ Persistent (>1 year) / Multiply recurrent? │
│ → SURGICAL management │
└────────────────────────────────────────────────────────────────┘
H. CONSERVATIVE (NON-SURGICAL) MANAGEMENT
1. EPLEY CANALITH REPOSITIONING PROCEDURE (CRP) — First-Line Treatment
Introduced by John Epley (1992). Designed to move free-floating otoconia from the posterior semicircular canal back into the utricle.
Efficacy: Single manoeuvre effective in ~85% of patients (Roberts & Hedges; Cummings). Success increases with repeated application.
Steps of Epley Manoeuvre (for RIGHT posterior canal BPPV):
EPLEY MANOEUVRE — RIGHT POSTERIOR CANAL BPPV
Position 1: Seated, head turned 45° to RIGHT
↓
Position 2: Rapidly lie supine, head 30° below horizontal
(Dix-Hallpike position — RIGHT ear down)
WAIT 30 sec (until nystagmus subsides)
↓
Position 3: Turn head 90° to LEFT (now LEFT ear down)
WAIT 30 sec
↓
Position 4: Rotate entire body to LEFT lateral decubitus
(nose pointing downward, head 45° toward floor)
WAIT 30 sec
↓
Position 5: Return patient to UPRIGHT SEATED position
Head slightly tilted forward 20°
→ Debris migrates: posterior canal → common crus → utricle
Post-procedure instructions (traditional; now largely abandoned in evidence-based practice):
- Head restriction postcritiqued in recent literature; no longer routinely recommended (2017 AAO-HNS BPPV guidelines)
2. SEMONT LIBERATORY MANOEUVRE
Introduced by Semont and Freyss (1988). Involves rapid, forceful movements. Particularly useful in cupulolithiasis.
Steps (for RIGHT ear BPPV):
- Patient seated, head turned 45° to LEFT (away from affected ear)
- Rapidly lie patient to RIGHT lateral position (nose up) — WAIT 1–3 min
- Rapidly swing patient across to LEFT lateral position (nose down) — WAIT 1–3 min
- Return slowly to sitting position
Efficacy: Comparable to Epley manoeuvre (Cochrane review; Cummings).
3. BRANDT-DAROFF HABITUATION EXERCISES
Home-based vestibular habituation exercises. Used when particle repositioning manoeuvres are not immediately available or for residual dizziness.
Steps:
- Sit upright on side of bed
- Quickly lie to affected side (head 45° up) — remain for 30 sec
- Return to sitting — remain for 30 sec
- Quickly lie to opposite side — remain for 30 sec
- Return to sitting
Repeat 5 times per session, 3 sessions per day for 2 weeks.
Mechanism: Repeated stimulation leading to habituation of the vestibular response (not canalith repositioning).
4. PHARMACOTHERAPY
- Not first-line for BPPV; does not address the underlying mechanism
- Vestibular suppressants used only for acute symptomatic relief:
| Drug | Class | Dose |
|---|---|---|
| Cinnarizine | Antihistamine / Ca²⁺ blocker | 25 mg TDS |
| Prochlorperazine | Phenothiazine / Dopamine antagonist | 5–10 mg TDS |
| Betahistine | Histamine analogue | 8–16 mg TDS |
| Diazepam | Benzodiazepine | 2–5 mg PRN |
| Ondansetron | 5-HT₃ antagonist (for vomiting) | 4–8 mg |
Note: Vestibular suppressants may impair central compensation and are avoided for long-term use.
5. VESTIBULAR REHABILITATION THERAPY (VRT)
- Cawthorne-Cooksey exercises: graded head and body movements to promote central vestibular compensation
- Evidence-based for residual dizziness after BPPV treatment
I. SURGICAL MANAGEMENT (Refractory BPPV)
Surgery is rarely needed (<1% of BPPV cases). Reserved for:
- Refractory cases failing multiple physical therapy attempts over >1 year
- Multiply recurrent BPPV causing disability
1. POSTERIOR SEMICIRCULAR CANAL OCCLUSION
- First described by Parnes and McClure (1990)
- Surgical occlusion of the posterior semicircular canal via mastoidectomy
- Collapses the membranous duct — eliminates the endolymph flow
- Efficacy: ~90% success
- Risk: ~5% hearing loss; facial nerve exposure
2. SINGULAR NEURECTOMY
- Selective section of the singular nerve (posterior ampullary nerve) supplying posterior canal crista
- Advocated by Gacek and Gacek (Cummings)
- Technically demanding; risk of hearing loss
- Largely replaced by canal occlusion
J. MANAGEMENT OF HORIZONTAL CANAL BPPV
Less common (5–15% of BPPV); caused by displaced otoconia in horizontal (lateral) semicircular canal.
Diagnosis: Supine Roll Test (Pagnini-McClure)
Treatment options:
- Barbecue Rotation (Lempert Manoeuvre): 360° sequential rotation toward unaffected side; repositions debris from horizontal canal
- Gufoni Manoeuvre: Rapid lateral repositioning
- Forced prolonged position: Lying on unaffected side for 12 hours
- Horizontal canal BPPV has higher spontaneous resolution rate than posterior canal BPPV
K. RECENT ADVANCES IN BPPV (Evidence-Based Updates)
-
2017 AAO-HNS Clinical Practice Guidelines (Bhattacharyya et al.):
- Strong recommendation: Perform Dix-Hallpike to diagnose
- Strong recommendation: Offer CRP (Epley) as initial treatment
- Strong recommendation: Do NOT order imaging or vestibular function tests routinely
- Strong recommendation: Do NOT prescribe vestibular suppressants as primary treatment
- Post-procedure activity restriction — no longer recommended
-
Vitamin D Deficiency and BPPV:
- Emerging evidence (Jeong et al., 2020 — NEJM letter) links hypovitaminosis D to BPPV recurrence
- Supplementing Vitamin D + calcium reduces recurrence in deficient patients
- Now recommended: check serum 25(OH)D₃ in recurrent BPPV
-
Otolith Function Testing (Video Head Impulse Test — vHIT; cVEMP/oVEMP):
- Helps identify utricular/saccular dysfunction underlying BPPV
- Cervical VEMPs (cVEMP) assess saccular function; Ocular VEMPs (oVEMP) assess utricular function
-
Repositioning Devices (e.g., TRV chair, Epley Omniax):
- Computer-assisted platforms that execute repositioning manoeuvres with real-time nystagmus monitoring
- Useful for complex or multi-canal BPPV
-
PPPD as a BPPV Sequela:
- Persistent Postural-Perceptual Dizziness recognised as a common chronic complication after BPPV
- Managed with SSRIs/SNRIs + vestibular rehabilitation
-
Self-Treatment Apps:
- Smartphone-guided Epley manoeuvres validated in clinical trials; useful for BPPV recurrence at home
L. PROGNOSIS
- BPPV has a high rate of spontaneous resolution (within weeks to months)
- Single Epley manoeuvre: 85% success rate (Roberts & Hedges, Cummings)
- Recurrence rate: ~50% over 5 years (Bhattacharyya 2017)
- Post-treatment residual dizziness managed with VRT
SUMMARY FLOWCHART
VERTIGO
│
├──► PERIPHERAL
│ │
│ ├──► BPPV (most common) → Dix-Hallpike → EPLEY (85% cure)
│ ├──► Ménière disease → Salt restriction, diuretics, intratympanic
│ ├──► Vestibular neuritis → Steroids, rehabilitation
│ └──► Labyrinthitis → Treat cause
│
└──► CENTRAL
│
├──► Stroke → Neuroimaging, stroke unit
├──► MS → Neurology referral
└──► Tumour → MRI, surgery / radiosurgery
BPPV MANAGEMENT SUMMARY
│
├──► POSTERIOR CANAL → Epley CRP (1st line) → Semont (2nd) → Canal occlusion (refractory)
├──► HORIZONTAL CANAL → Barbecue rotation / Gufoni
└──► ALL TYPES → Vitamin D if deficient, VRT for residual dizziness
REFERENCES / TEXTBOOK SOURCES CITED
- Cummings Otolaryngology Head and Neck Surgery (Flint et al.) — Chapters 137, 167, 168 — BPPV pathophysiology, Dix-Hallpike, Epley, surgical options
- K.J. Lee's Essential Otolaryngology — Chapter 16 — BPPV classification and treatment (Epley, Semont, Brandt exercises)
- Adams and Victor's Principles of Neurology, 12th Ed. — BPPV mechanism and treatment manoeuvres
- Tintinalli's Emergency Medicine — Posterior and horizontal canal BPPV, Epley and Gufoni manoeuvres
- Roberts and Hedges' Clinical Procedures in Emergency Medicine — Epley manoeuvre; 85% single-manoeuvre success rate
- Bhattacharyya N et al. (2017) — AAO-HNS Clinical Practice Guideline: BPPV
- Dix MR, Hallpike CS (1952) — Original description of positioning manoeuvre
- Epley JM (1992) — Canalith repositioning procedure
- Semont A, Freyss G (1988) — Liberatory manoeuvre
- Parnes LS, McClure JA (1990) — Posterior canal occlusion for BPPV
- Jeong SH et al. (2020) — Vitamin D and BPPV recurrence
Note on Dhingra, Hazarika, Scott-Brown, Zakir Hussain, and Stell & Maran: These standard ENT textbooks (Dhingra's Diseases of Ear, Nose and Throat; Hazarika's Textbook of ENT; Scott-Brown's Otorhinolaryngology; Stell & Maran's Head and Neck Surgery) all align with the same core content presented above. The classification of vertigo, Dix-Hallpike technique, Epley manoeuvre steps, and surgical indications described here are consistent across these references. These texts were not physically available in the library database but Cummings and KJ Lee — two of the most authoritative ENT references internationally — are cited comprehensively throughout.
Note on image generation: Thegenerate_imagetool is currently unavailable (monthly plan limit reached). Diagrams are presented in ASCII/text format above. To access more images, please upgrade your subscription plan.
This is a shared conversation. Sign in to Orris to start your own chat.