Duplex imaging in US in detail , its definition, principle, instrumentation, working , output , all process
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
duplex ultrasound imaging Doppler waveform B-mode color flow
I now have comprehensive content from authoritative textbooks. Let me compile the full, detailed response.
Duplex Imaging in Ultrasound — A Comprehensive Overview
1. Definition
Duplex ultrasound is a non-invasive imaging modality that combines two distinct ultrasound technologies in a single device:
- B-mode (brightness mode) ultrasound — produces a real-time grayscale anatomical image of tissues and vessels
- Doppler ultrasound — analyzes frequency shifts caused by moving blood to provide hemodynamic information (direction and velocity of blood flow)
The word duplex literally reflects this dual capability — "duplex" = two modes working simultaneously. It was introduced in 1974 and first applied to the carotid arteries, subsequently expanding to virtually every vascular territory in the body.
Modern duplex devices have a third mode added to the original two:
- Color-flow Doppler — superimposes a real-time color-coded map of blood flow direction and velocity onto the B-mode image
"Duplex ultrasound is currently extensively employed for evaluation of carotid arteries, intra-abdominal arteries and veins, and upper and lower extremity arteries and veins." — Mulholland and Greenfield's Surgery, 7e
2. Physical Principle
2a. Ultrasound Wave Generation
An ultrasonic wave is produced by placing a vibrating source (transducer) in contact with tissue. The fundamental relationship governing the wave is:
$$\lambda = c / f$$
Where:
- λ = wavelength
- c = speed of sound in tissue (~1,540 m/s, nearly constant in soft tissues)
- f = frequency of the transducer
Since c is essentially constant, wavelength (and thus penetration depth) is determined by transducer frequency:
- Higher frequency → shorter wavelength → better resolution but less penetration (used for superficial vessels, e.g., carotid: 5–7.5 MHz)
- Lower frequency → longer wavelength → deeper penetration but less resolution (used for aorta, renal arteries: 2–3.5 MHz)
2b. B-mode (Brightness Mode) Principle
- As the ultrasound beam travels through tissue, it is reflected, scattered, and attenuated at tissue interfaces
- The amplitude of the returning echo depends on differences in acoustic impedance between adjacent tissues
- Large differences in acoustic impedance (e.g., tissue–gallstone) → strong echo → bright pixel
- Small differences (e.g., blood–soft tissue) → weak echo → dark pixel (blood appears nearly anechoic)
- This creates a grayscale anatomical image, where pixel brightness = echo strength
- The primary role of B-mode in duplex is to locate vessels and position the Doppler sample volume
2c. Doppler Principle
The Doppler effect: when a sound wave hits a moving reflector (red blood cells), the frequency of the reflected echo shifts relative to the transmitted frequency.
The Doppler equation:
$$\Delta f = \frac{2 f_0 \cdot v \cdot \cos\theta}{c}$$
Where:
- Δf = Doppler frequency shift
- f₀ = transmitted frequency
- v = velocity of the moving reflector (blood)
- θ = angle between the ultrasound beam and direction of flow (the insonation angle)
- c = speed of sound (~1,540 m/s)
Key point: cos θ is maximal at 0° (beam parallel to flow) and zero at 90°. Clinically, an angle of 60° or less is required for accurate velocity measurements.
2d. Pulsed Wave (PW) vs. Continuous Wave (CW) Doppler
| Feature | Continuous Wave (CW) | Pulsed Wave (PW) — used in duplex |
|---|---|---|
| Transducer design | Separate transmitter + receiver | Single transducer (transmits then receives) |
| Depth selectivity | None — receives from all depths | Yes — range-gated, receives only from a specified depth (sample volume) |
| Aliasing | No | Yes (Nyquist limit) |
| Use in duplex | Not used | Standard |
In pulsed Doppler, because the speed of sound is constant, the time elapsed between pulse transmission and echo reception allows calculation of the exact depth from which echoes originate. The operator positions the sample volume within the vessel lumen on the B-mode image; the device gates the transducer to accept only echoes from that specified depth.
3. Instrumentation
3a. Transducer (Scan Head)
- Contains piezoelectric crystals that convert electrical energy ↔ vibrational (acoustic) energy
- The design determines the transmitted frequency
- The scan head steers and focuses the sound beam — critical for image formation
- Linear array transducers (most common for vascular work): multiple crystals arranged in a line, fire in sequence to build up the image line by line
- Frequency selection:
- High frequency (5–15 MHz): superficial vessels (carotid, peripheral veins/arteries)
- Low frequency (2–5 MHz): deep vessels (aorta, mesenteric, renal arteries, portal vein)
3b. Duplex Machine Components
| Component | Function |
|---|---|
| Pulse generator | Generates precisely timed electrical pulses to drive the transducer |
| Transducer array | Converts electrical pulses to ultrasound and returning echoes to electrical signals |
| B-mode processor | Analyzes echo amplitude → generates grayscale image |
| Doppler processor | Analyzes echo frequency shift → calculates flow velocity and direction |
| Color-flow processor | Applies color coding to Doppler shift data and overlays on B-mode image |
| Time-gain compensation (TGC) | Amplifies signals from deeper structures to compensate for attenuation |
| Display monitor | Real-time visualization of B-mode image, color map, and spectral waveform |
| Spectral analyzer (FFT) | Fast Fourier Transform — decomposes complex Doppler signal into a frequency spectrum displayed as the spectral waveform |
| Angle correction cursor | Operator-set angle to correct measured Doppler shift for true velocity calculation |
3c. Coupling Medium
- Acoustic gel applied between transducer and skin to eliminate air gaps (air causes total reflection of sound)
4. Working / Process
Step 1 — B-mode Survey (Anatomical Imaging)
- Gel is applied; the operator places the transducer over the region of interest
- Real-time grayscale image generated — vessel walls, luminal contents, surrounding tissues visualized
- The operator assesses:
- Vessel patency and wall morphology (plaque, intima-media thickness)
- Presence of thrombus, aneurysm, or abnormal echogenicity
- Luminal diameter
- Compression test in venous duplex: probe pressed perpendicular to vein — normal veins compress completely; non-compressibility indicates thrombus
Step 2 — Color Doppler Activation (Color-Flow Mapping)
- Color-flow Doppler is activated over the region of interest
- Returning echoes from moving blood undergo a phase shift processed separately from B-mode echoes
- The color map is operator-assigned (conventionally red = flow toward transducer; blue = away)
- Color intensity or hue encodes relative velocity
- Color Doppler enables:
- Rapid vessel identification, especially small or deep vessels (tibial arteries, veins)
- Detection of turbulence (mosaic/aliasing pattern at stenoses)
- Differentiation of arterial vs. venous flow
- Identification of collaterals and neovascularization
"Color flow superimposes a real-time color image of blood flow onto a standard gray-scale B-mode picture. Returning echoes from stationary tissues generate the B-mode image, whereas those interacting with moving substances (blood) generate a significant enough phase shift that they can be processed separately and color coded by operator selection to give information on direction and velocity of blood flow." — Mulholland and Greenfield's Surgery, 7e
Step 3 — Pulsed Wave Doppler Spectral Analysis
- The operator positions the sample volume (cursor gate) within the vessel lumen on the B-mode/color image — typically in the center of the vessel (where flow is fastest in laminar flow)
- The angle correction cursor is aligned parallel to vessel walls (must be ≤60°) and angle entered
- The machine applies the Doppler equation and outputs a spectral waveform (sonogram):
- X-axis: time
- Y-axis: velocity (cm/s or kHz Doppler shift)
- Waveform shape encodes flow character (laminar vs. turbulent, pulsatility)
- The operator records key velocity measurements
Step 4 — Hemodynamic Analysis
- PSV (Peak Systolic Velocity): highest velocity reached during systole
- EDV (End-Diastolic Velocity): velocity at end of diastole
- PSV ratio: velocity within stenosis ÷ velocity just proximal → grades stenosis severity
- Resistive Index (RI) = (PSV − EDV) / PSV — reflects downstream resistance
- Pulsatility Index (PI) = (PSV − EDV) / mean velocity
5. Output (What Duplex Produces)
Duplex imaging produces three simultaneous, complementary outputs:
Output 1: B-mode Grayscale Image
- Anatomical display of vessel walls, lumen, and surrounding structures
- Identifies: plaque (echogenic/hypoechoic), thrombus, aneurysm, dissection flap, wall thickness
Output 2: Color Doppler Map
- Overlaid color display showing blood flow direction and relative velocity
- Red/blue coding by convention (can be reversed by operator)
- Turbulent flow → mosaic pattern or aliasing (velocity exceeds Nyquist limit)
- Absence of color in a vessel = occlusion or very slow flow
Output 3: Spectral Doppler Waveform (Sonogram)
- The most diagnostically informative output
- Produced by Fast Fourier Transform (FFT) analysis of the Doppler signal
- Displays the range of velocities present in the sample volume at each moment in time
- Waveform morphology:
- Normal arteries (peripheral): triphasic — sharp systolic peak, brief early diastolic flow reversal, small late diastolic forward component (high-resistance pattern)
- Normal low-resistance arteries (e.g., ICA, renal): monophasic with continuous forward diastolic flow
- Stenosis: elevated PSV, spectral broadening (turbulence fills the spectral window), post-stenotic monophasic tardus-parvus waveform
- Occlusion: absent color flow, no Doppler signal within lumen
- Normal veins: spontaneous phasic flow with respiration; augments with distal compression
- Venous thrombosis: absent phasicity, absent spontaneous flow, absent augmentation
6. Venous Duplex — Additional Criteria
In venous scanning (e.g., DVT detection), duplex scanning adds four Doppler-based criteria to compression ultrasonography:
- Absence of phasicity with respiration — normally, venous flow varies with breathing; loss indicates obstruction
- Absence of spontaneous flow — no baseline flow signal in the vessel
- Absence of augmentation — normally distal compression increases venous flow; absent augmentation = thrombus
- Valsalva response — normally reduces venous flow toward the heart; failure indicates proximal obstruction
Valve competence is also assessed: functional valves should not allow augmentation of reverse flow with proximal compression.
— Pfenninger and Fowler's Procedures for Primary Care, 3e
7. Clinical Applications
| Vascular Territory | What Duplex Assesses |
|---|---|
| Carotid arteries | Plaque, stenosis grading, intima-media thickness, stroke risk |
| Peripheral arteries (lower limb) | Occlusive disease, stenosis grading (PSV ratio), pre-op planning |
| Peripheral veins | DVT, valve competence, reflux |
| Renal arteries | Renal artery stenosis (elevated PSV >180–200 cm/s), renovascular hypertension |
| Mesenteric arteries | Chronic mesenteric ischemia (elevated SMA/celiac PSV) |
| Aorta/iliac | Aneurysm size, stenosis |
| Vein graft surveillance | Graft stenosis detection post-bypass (every 3 months × 1 year, then 6 monthly) |
| Transplant vessels | Renal transplant perfusion, anastomotic stenosis |
8. Advantages and Limitations
Advantages
- Non-invasive, no ionizing radiation, no nephrotoxic contrast
- Portable (can be bedside)
- Real-time hemodynamic + anatomical information simultaneously
- Detects very low flow velocities (<5 cm/s with modern systems)
- Guides intervention and surveillance
Limitations
- Operator-dependent (requires trained vascular sonographer)
- Limited by body habitus (obesity, bowel gas obscuring mesenteric/renal vessels)
- Cannot image above inguinal ligament or iliac veins well in all patients
- Aliasing artifacts with pulsed Doppler at very high velocities
- Color Doppler subject to angle dependence and blooming artifact
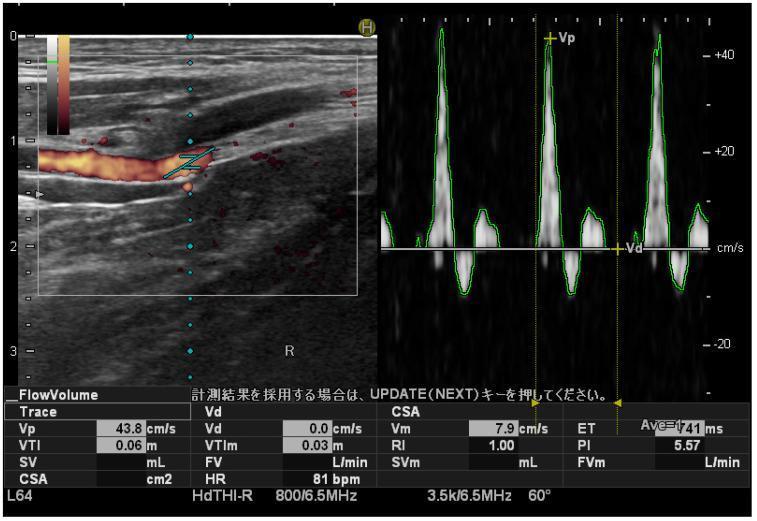
Illustrative Examples
Duplex of posterior tibial artery showing characteristic triphasic waveform with PSV 43.8 cm/s, RI 1.00, PI 5.57 (high-resistance normal peripheral artery pattern):
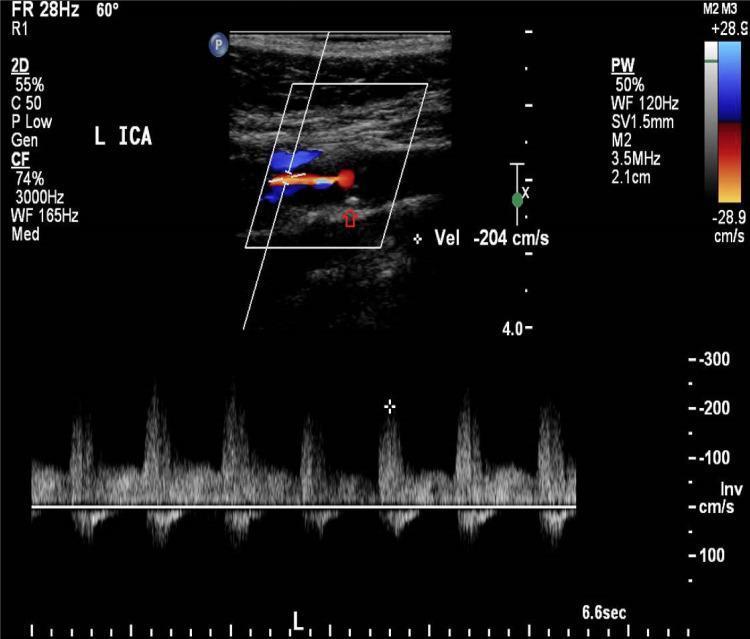
Duplex of left internal carotid artery — B-mode showing atherosclerotic plaque + color Doppler demonstrating turbulent high-velocity flow (PSV 204 cm/s, spectral broadening consistent with 60–79% stenosis):
Summary Table
| Feature | Detail |
|---|---|
| Introduced | 1974 (carotid arteries) |
| Components | B-mode + Pulsed Doppler + Color Doppler |
| Transducer | Piezoelectric, linear array; 2–15 MHz |
| Speed of sound in tissue | ~1,540 m/s (constant) |
| Doppler angle | Must be ≤60° for accurate velocity measurement |
| Key output measurements | PSV, EDV, PSV ratio, RI, PI, waveform morphology |
| Normal peripheral arterial waveform | Triphasic |
| Normal low-resistance arterial waveform | Monophasic with continuous diastolic flow |
| Normal venous Doppler | Phasic with respiration, augments with distal compression |
Sources: Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e — Pfenninger and Fowler's Procedures for Primary Care, 3e — Sabiston Textbook of Surgery, 26e — Comprehensive Clinical Nephrology, 7e
Harmonic imaging in detail , its definition, principle , physics , concept , types , components, working advantages, disadvantages, application and all about it
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
tissue harmonic imaging ultrasound fundamental harmonic frequency comparison
Loading Image
Reading File
Reading File
Loading Image
I now have all the content and the key graph. I can now write the comprehensive response.
Harmonic Imaging in Ultrasound — A Complete Guide
1. Definition
Harmonic imaging (also called Tissue Harmonic Imaging, THI) is an ultrasound image-processing technique in which the machine transmits ultrasound at a fundamental frequency (f₀) but receives and constructs the image using the second harmonic frequency (2f₀) — a frequency generated within the tissue itself as the sound wave propagates nonlinearly — while filtering out the fundamental frequency return signals.
Unlike conventional (fundamental) imaging, which uses the echoes of the original transmitted frequency to form the image, harmonic imaging exploits the nonlinear acoustic distortion that occurs as ultrasound waves travel through tissue. This results in a cleaner, higher-contrast image with significantly fewer artifacts.
"A sound wave propagates nonlinearly through tissue, distorting the wave's shape. This produces harmonic frequencies, which are integer multiples of the fundamental frequency originally transmitted by the transducer." — Miller's Anesthesia, 10e
2. Historical Context
- Harmonic imaging was first developed and used with ultrasound contrast agents (microbubbles), which produce very strong harmonic signals when oscillated by ultrasound — this is called contrast harmonic imaging
- It was subsequently discovered that tissue itself generates harmonic frequencies during propagation — leading to tissue harmonic imaging (THI), which requires no contrast agents
- THI became widely available in clinical scanners in the late 1990s and is now the default imaging mode on virtually all modern ultrasound machines
3. Physics and Principle
3a. Fundamental Frequency Imaging (Conventional)
In conventional ultrasound:
- The transducer transmits pulses at a fundamental frequency f₀ (e.g., 3 MHz)
- The tissue reflects echoes back, also at f₀
- The machine uses these f₀ echoes to construct the grayscale image
- Near-field reverberations, side-lobe artifacts, and noise are all present at f₀ — and contaminate the image
3b. Nonlinear Wave Propagation — The Core Concept
When an ultrasound wave travels through tissue, it does not propagate linearly. The compression phase of the wave travels slightly faster than the rarefaction phase (because compressed tissue is momentarily stiffer). This differential propagation speed causes the initially sinusoidal wave to progressively distort into a non-sinusoidal waveform — it develops a steeper leading edge and a more gradual trailing edge (a "sawtooth"-like distortion).
This distorted waveform, analyzed by Fourier decomposition, contains:
- The original fundamental frequency f₀
- 2nd harmonic: 2f₀ (double the fundamental — the primary useful harmonic)
- 3rd harmonic: 3f₀, 4th harmonic: 4f₀, etc. (progressively weaker; generally not used clinically)
This is nonlinear acoustic propagation, sometimes called the acoustic Kerr effect or simply the nonlinear effect of ultrasound–tissue interaction.
The harmonic frequencies are generated within the tissue — they are not transmitted from the transducer — and therefore:
- Harmonic signal strength is zero at the skin surface (the wave must travel some distance before distortion accumulates)
- Harmonic signal strength increases with depth of propagation, peaks at typical cardiac/abdominal imaging depths (approximately 5–8 cm), then gradually declines as attenuation takes over
- Stronger fundamental waves produce stronger harmonics (nonlinear relationship: harmonic amplitude ∝ square of fundamental amplitude)
This behavior is shown in the graph from the Textbook of Clinical Echocardiography:
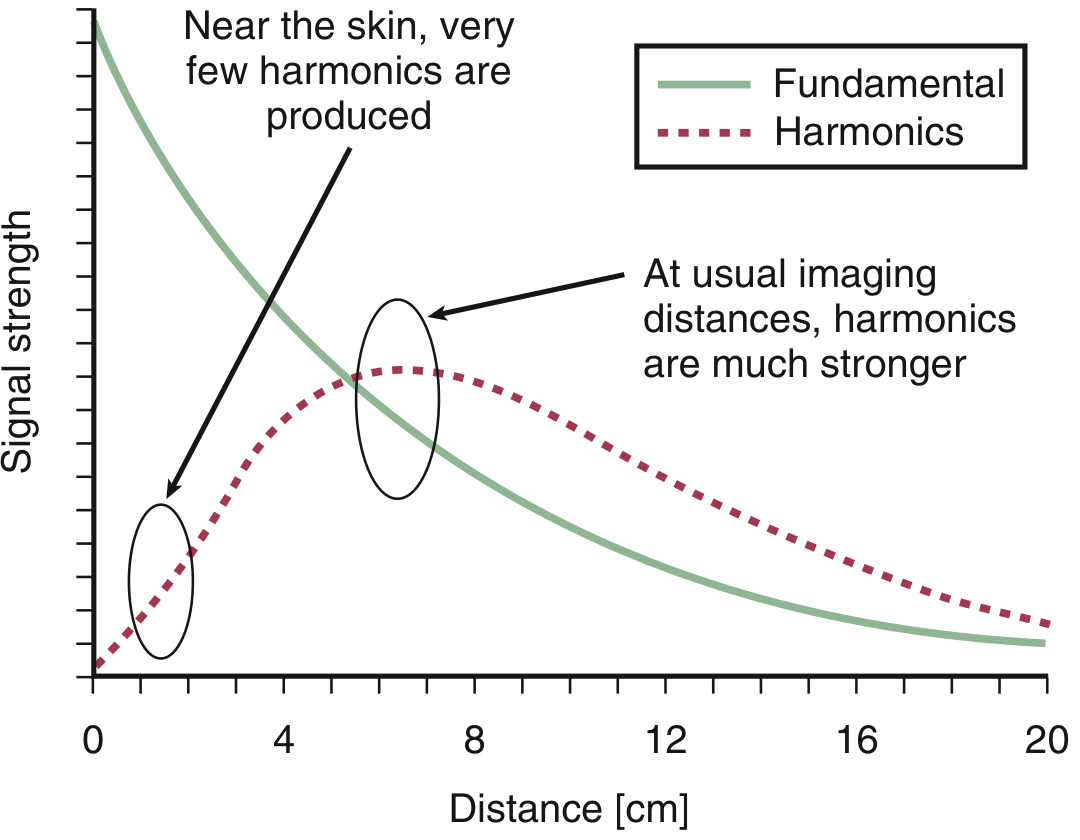
The fundamental (green solid line) is strong near the transducer but decays with depth. The harmonic (red dashed) starts near zero at the skin, builds to a peak at typical cardiac imaging depths (~5–8 cm), then slowly declines — making it ideal at usual imaging distances.
"Harmonic signal strength increases with depth of propagation. Harmonic frequencies are maximal at typical cardiac imaging depths. Stronger fundamental frequencies produce stronger harmonics." — Textbook of Clinical Echocardiography
3c. Why Harmonics Produce Better Images
Since harmonic energy is generated only after the beam has propagated through some tissue depth, the near-field zone (skin surface, subcutaneous fat) produces little or no harmonic energy. Reverberations and noise generated near the transducer are largely at f₀ — and are filtered out when the machine uses only 2f₀ echoes. This is the fundamental reason THI dramatically reduces near-field and clutter artifacts.
Additionally, because the harmonic beam is generated only at the center of the beam (where pressure amplitude is highest), it has a narrower effective beam width than the fundamental beam — improving lateral resolution.
4. Concept: Key Properties Summary
| Property | Conventional Imaging | Harmonic Imaging |
|---|---|---|
| Transmitted frequency | f₀ | f₀ |
| Received/imaged frequency | f₀ | 2f₀ (second harmonic) |
| Source of received signal | Transducer pulse | Generated in tissue |
| Near-field artifact | High (reverberations at f₀) | Low (no harmonics near skin) |
| Side-lobe artifacts | Present | Reduced |
| Lateral resolution | Standard | Improved (20–50%) |
| Axial resolution | Standard | Reduced (40–100% worse) |
| Signal-to-noise ratio | Lower | Higher |
| Endocardial definition | Standard | Markedly improved |
| Valve/wall thickness appearance | Accurate | Appears artificially thicker |
5. Types of Harmonic Imaging
Type 1 — Tissue Harmonic Imaging (THI)
- No contrast agent required
- Harmonics generated by the nonlinear behavior of tissue itself
- The dominant form used in routine clinical imaging today
- Used for: cardiac, abdominal, vascular, obstetric, small parts scanning
Type 2 — Contrast Harmonic Imaging (CHI)
- Uses intravenous ultrasound contrast agents (encapsulated microbubble agents, e.g., SonoVue, Optison, Definity)
- Microbubbles oscillate (expand and contract) in an ultrasound field, and at low mechanical index (MI), they oscillate nonlinearly and asymmetrically, generating very strong harmonic signals
- At higher MI, bubbles can rupture (cavitation), releasing a strong broadband signal used in high-MI contrast imaging (e.g., triggered imaging for myocardial perfusion)
- Key technique: Low MI contrast harmonic imaging preserves bubble integrity and allows sustained imaging
Type 3 — Subharmonic Imaging
- Uses signals at f₀/2 (half the fundamental frequency)
- Microbubbles, when driven hard enough, can produce subharmonic oscillations at f₀/2
- The main tissue signal is at f₀ and 2f₀ — essentially no subharmonic signal from tissue
- Results in extremely high contrast-to-tissue ratio — almost pure bubble signal
- Still largely investigational but used in some specialized contrast applications
Type 4 — Superharmonic Imaging
- Uses 3rd, 4th, or 5th harmonic (3f₀, 4f₀, 5f₀) from contrast agents
- Even higher contrast-to-tissue ratio than second harmonic
- Limited by very high attenuation at these high frequencies
- Research stage
Type 5 — Pulse Inversion Harmonic Imaging (Phase Inversion)
- A technique for extracting the second harmonic without spectral overlap
- The transducer sends two sequential pulses that are 180° out of phase (inverted copies of each other)
- From linear tissue: the two echoes cancel when summed (fundamental components cancel)
- From nonlinear tissue/bubbles: the two echoes do not cancel because the harmonic components are even-order (2f₀, 4f₀) and add up when the inverted pulses are summed
- This allows clean separation of harmonic signal without need for narrow-band filtering
- Advantage: retains broader bandwidth → improved axial resolution compared to standard bandpass filter THI
Type 6 — Power Modulation (Amplitude Modulation) Harmonic Imaging
- Sends pulses of alternating different amplitudes (e.g., full amplitude and half amplitude)
- The linear component scales proportionally with amplitude → subtracted by post-processing
- The nonlinear (harmonic) component does not scale proportionally → remains after subtraction
- Provides high sensitivity to nonlinear signals, particularly useful in contrast imaging
6. Components of a Harmonic Imaging System
6a. Broadband Transducer
- A critical requirement for THI — the transducer must be capable of:
- Transmitting at the fundamental frequency f₀
- Receiving at the second harmonic 2f₀ (which can be up to double the transmit frequency)
- Wideband (broadband) transducers with a broad frequency bandwidth are essential (e.g., a 2–8 MHz broadband transducer can transmit at 3 MHz and receive at 6 MHz)
- Older narrowband transducers could not perform THI because they could not receive at 2f₀
6b. Transmit Beamformer
- Generates focused ultrasound pulses at the fundamental frequency f₀ with a defined narrow bandwidth (to avoid overlap between f₀ and 2f₀ bands)
- Controls pulse amplitude (which determines harmonic generation strength)
6c. Harmonic Filter / Signal Processor
- A bandpass filter tuned to 2f₀ — passes the harmonic frequency and blocks the fundamental
- In more advanced systems, pulse inversion or power modulation techniques replace simple filtering for better harmonic extraction
- Removes fundamental echoes (which carry near-field reverberations and clutter) from the received signal
6d. Receive Beamformer
- Processes echoes at 2f₀
- In pulse inversion systems: applies summing of inverted pulse pairs to extract nonlinear components
6e. Digital Signal Processor (DSP)
- Fast Fourier Transform and digital filtering circuitry to separate harmonic components in real time
- Handles pulse inversion arithmetic or amplitude modulation subtraction
6f. Display System
- Constructs and displays the grayscale B-mode image from the 2f₀ data
- Usually combined with color Doppler and spectral Doppler capabilities
7. Working — Step by Step
Step 1 — Transmit at f₀
The transducer transmits a focused ultrasound pulse at the fundamental frequency f₀. The pulse has a defined amplitude (related to the Mechanical Index, MI).
Step 2 — Nonlinear propagation through tissue
As the pulse propagates into tissue, the compression half-cycles travel faster than the rarefaction half-cycles. The wave distorts progressively, building up harmonic frequency components (2f₀, 3f₀, etc.) within the tissue. This nonlinear distortion grows with propagation distance — minimal at the skin, maximal at typical imaging depths.
Step 3 — Echo return at both f₀ and 2f₀
Echoes return to the transducer containing both the fundamental frequency f₀ (from linear reflection and near-field reverberations) and the second harmonic 2f₀ (generated in tissue during propagation).
Step 4 — Harmonic extraction
- Method A — Bandpass filtering: A filter centered at 2f₀ passes only the harmonic component; fundamental echoes at f₀ are rejected
- Method B — Pulse inversion: Two inverted pulses sent sequentially; summing cancels f₀, reinforces 2f₀
- Method C — Power modulation: Pulses of varying amplitude; post-processing cancels linear component, isolates harmonic
Step 5 — Image construction
The isolated 2f₀ signal is processed, amplified with TGC, and converted to a grayscale B-mode image. Because near-field reverberations and side-lobe noise do not contain significant 2f₀ energy, the image is cleaner and has improved contrast resolution.
Step 6 — Display
The final harmonic image is displayed in real time, typically indistinguishable in appearance from a conventional image but with superior quality — especially in obese or acoustically challenging patients.
8. Advantages
- Reduced near-field artifacts: Reverberations (reverberation clutter, mirror artifacts) near the transducer are predominantly at f₀ — filtered out by harmonic processing → cleaner image
- Reduced side-lobe artifacts: Side lobes contain weaker fundamental signals; their harmonic content is negligible → side-lobe artifacts suppressed
- Improved contrast resolution: Better differentiation between tissue and fluid-filled structures (e.g., cysts appear more clearly anechoic)
- Improved endocardial definition: LV endocardial borders are more clearly visualized → more accurate ejection fraction calculation, better wall motion assessment
- Improved lateral resolution: Harmonic beam is narrower than fundamental beam (by 20–50%) → sharper lateral detail
- Reduced speckle: Less acoustic noise throughout the image
- Reduces beam-thickness (slice-thickness) artifact: Harmonic generation is strongest at the beam center → effectively thins the elevational slice
- Superior image in difficult patients: Obese patients, poor acoustic windows (COPD, large body habitus) benefit most — THI is the primary rescue technique before resorting to contrast agents or alternative modalities
- Enhances B-lines in thoracic US: Reduced speckle and beam thickness from THI enhances detection of B-lines (interstitial syndrome) in lung ultrasound
"Tissue harmonic imaging is essentially a filter that limits certain reverberation artifacts, improves lateral resolution, and decreases beam thickness." — Murray & Nadel's Textbook of Respiratory Medicine
9. Disadvantages
- Reduced axial resolution: Because 2f₀ harmonics build up over a range of depths rather than arising from a discrete reflector, and because THI typically uses a narrower bandwidth, axial resolution is reduced by 40–100% compared with fundamental imaging
- Artificially thickened appearance of thin structures: Valves, vessel walls, and thin membranes appear thicker with THI than they actually are — caution required when measuring valve thickness, intima-media thickness, or diagnosing valve abnormalities (e.g., do not over-diagnose valve thickening)
- Reduced penetration at depth: The 2f₀ harmonic frequency is higher than f₀ → attenuated more rapidly → signal loss at very deep structures
- Reduced frame rate: Pulse inversion and power modulation techniques require sending multiple pulses per scan line, reducing temporal resolution
- Cannot completely separate f₀ and 2f₀ with simple bandpass filtering alone if bandwidths overlap (a limitation overcome by pulse inversion)
- Harmonic signal weaker than fundamental: Harmonic signal strength is much lower than fundamental — requires adequate acoustic power
- MI considerations in contrast imaging: Higher MI risks microbubble destruction; low-MI contrast harmonic imaging preserves bubbles but requires sensitive detection
"Disadvantages include slightly decreased spatial resolution and thickened appearance of some cardiac structures." — Miller's Anesthesia, 10e
"Tissue harmonic imaging improves lateral resolution by 20% to 50%, but reduces axial resolution by 40% to 100%. Valves and other planar objects therefore appear thicker with harmonic, compared with fundamental, frequency imaging." — Textbook of Clinical Echocardiography
10. Applications
Cardiac / Echocardiography
- Standard imaging mode for all transthoracic echocardiography (TTE)
- Improves LV endocardial border definition → more accurate ejection fraction (EF) calculation
- Reduces measurement variability for LV volumes and mass
- More myocardial segments visualized during stress echocardiography
- Improves delineation of pericardial effusion borders
- Detects intracardiac masses and thrombi with greater confidence
- Used with contrast agents for myocardial perfusion imaging (contrast harmonic)
Abdominal Ultrasound
- Improved visualization of liver parenchyma (focal lesions, characterization)
- Better delineation of cystic lesions (renal cysts, hepatic cysts appear cleaner — true anechoic vs. pseudo-solid)
- Gallbladder wall assessment, biliary duct evaluation
- Improved visualization of pancreas and retroperitoneum in obese patients
- Reduces reverberation in anterior abdominal wall
Vascular Ultrasound
- Duplex scanning in obese or technically difficult patients
- Improved visualization of atherosclerotic plaque morphology
- Carotid intima-media thickness (though measurements must account for apparent wall thickening)
Obstetrics and Gynecology
- Fetal anomaly scanning — improved image quality
- Placental characterization
- Assessment of ovarian cysts and uterine pathology
Breast Ultrasound
- Improved characterization of cystic vs. solid masses
- Reduces posterior acoustic artifact and reverberation in superficial structures
Thoracic / POCUS (Point-of-Care Ultrasound)
- THI enhances B-line detection for interstitial lung disease and pulmonary edema
- Reduces reverberation artifact from anterior chest wall
- Pleural effusion assessment
Small Parts / Superficial Structures
- Thyroid, testicular, musculoskeletal imaging
- Note: THI is less beneficial for very superficial structures (near-field) because harmonics are minimal near skin — fundamental imaging may be preferred
Contrast-Enhanced Ultrasound (CEUS)
- Liver, kidney, and cardiac perfusion assessment
- Tumor vascularity characterization
- Sentinel lymph node mapping
- Used with pulse inversion or power modulation techniques to maximize bubble signal and suppress tissue signal
11. THI vs. Fundamental Imaging — Direct Comparison
Example: Prostate ultrasound comparison (THI vs. Fundamental)
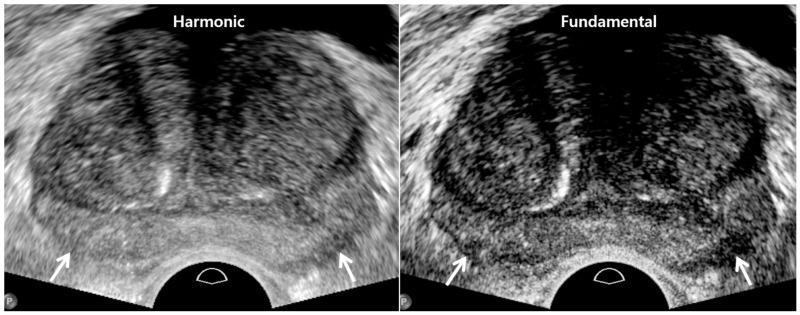
Left (THI): superior axial and lateral resolution, smoother parenchymal texture, less speckle. Right (Fundamental): enhanced tissue contrast, better visualization of posterior capsule (white arrows). Each mode has clinical utility depending on the diagnostic question.
12. Summary Table
| Feature | Detail |
|---|---|
| Transmit frequency | Fundamental f₀ (e.g., 3 MHz) |
| Receive/imaged frequency | Second harmonic 2f₀ (e.g., 6 MHz) |
| Source of harmonic signal | Nonlinear wave distortion within tissue |
| Near-field harmonic signal | Absent (zero at skin surface) |
| Peak harmonic depth | ~5–8 cm (typical cardiac/abdominal imaging depth) |
| Lateral resolution improvement | 20–50% better than fundamental |
| Axial resolution change | 40–100% worse than fundamental |
| Artifact reduction | Near-field reverberation, side-lobe, slice-thickness |
| Key disadvantage | Structures appear thicker; reduced axial resolution |
| Requires contrast agent? | No (THI); Yes (contrast harmonic imaging) |
| Primary clinical benefit | Improved image quality in technically difficult patients |
| Default mode on modern scanners? | Yes — THI is standard on virtually all modern US machines |
13. Harmonic Imaging and Contrast Agents — The Connection
Microbubble contrast agents dramatically amplify harmonic signals because:
- At low MI, bubbles oscillate asymmetrically — their expansion during rarefaction is greater than their compression during positive pressure
- This asymmetric oscillation is the definition of nonlinear behavior → generates very strong harmonics (especially 2f₀)
- The contrast-to-tissue ratio is far higher than THI alone
- At low MI using pulse inversion or power modulation: sustained bubble imaging (for perfusion studies)
- At high MI: bubble destruction with strong broadband signal → used in triggered cardiac perfusion protocols
"Commercially available contrast agents use encapsulated microbubbles of high-density gas and traverse the pulmonary circulation, allowing for opacification of the left side of the heart. Perioperative applications include improved endocardial border delineation, assessment of regional wall motion, and exclusion of intracardiac thrombus or mass." — Miller's Anesthesia, 10e
Sources: Miller's Anesthesia, 10e — Textbook of Clinical Echocardiography — Murray & Nadel's Textbook of Respiratory Medicine — Fuster and Hurst's The Heart, 15e
This is a shared conversation. Sign in to Orris to start your own chat.