Enumerate the causes of traumatic facial palsy and discuss its management in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
facial nerve anatomy segments temporal bone
Searching Images
temporal bone fracture facial nerve injury CT scan
Loading Image
Loading Image
Loading Image
Now I have comprehensive material. Let me compile the full 50-mark answer.
TRAUMATIC FACIAL PALSY — Causes & Management
(50 Marks | RGUHS Standard)
Sources: Cummings Otolaryngology HNS 6e, Scott-Brown's Otorhinolaryngology 8e, KJ Lee's Essential Otolaryngology, Dhingra's Diseases of ENT, Hazarika's Textbook of ENT, Stell & Maran, Zakir Hussain ENT
PART I: INTRODUCTION
Facial nerve palsy (FNP) refers to weakness or paralysis of the muscles of facial expression due to involvement of the 7th cranial nerve. Among all causes of FNP, traumatic aetiology is second only to Bell's palsy and carries the most significant medico-legal and surgical implications.
Grading of facial palsy — House-Brackmann Scale (universally used):
| Grade | Description | Function |
|---|---|---|
| I | Normal | 100% |
| II | Mild dysfunction | Slight weakness, complete eye closure |
| III | Moderate dysfunction | Obvious weakness, complete eye closure with effort |
| IV | Moderately severe | Incomplete eye closure, asymmetry at rest |
| V | Severe dysfunction | Barely perceptible motion |
| VI | Total paralysis | No movement |
PART II: SURGICAL ANATOMY OF THE FACIAL NERVE
Understanding traumatic FNP requires precise knowledge of the nerve's course through the temporal bone, as different injury sites produce different clinical patterns.
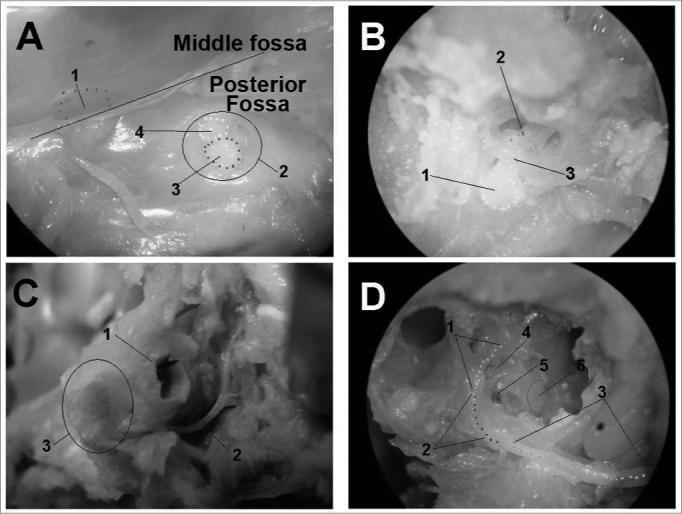
Segments of the Facial Nerve (Intratemporal)
BRAINSTEM (Pons — motor nucleus)
↓
CISTERNAL SEGMENT (in posterior fossa)
↓
MEATAL SEGMENT (Internal Auditory Canal — ~8 mm)
↓
LABYRINTHINE SEGMENT (3–4 mm — NARROWEST, most vulnerable)
↓ Geniculate ganglion (gives off Greater Petrosal Nerve → parasympathetics)
TYMPANIC / HORIZONTAL SEGMENT (8–11 mm — medial wall of middle ear)
↓ Stapedius nerve
MASTOID / VERTICAL SEGMENT (10–14 mm — descends in posterior mastoid)
↓ Chorda tympani (taste, submandibular/sublingual glands)
STYLOMASTOID FORAMEN (exits skull base)
↓
EXTRATEMPORAL (parotid gland → pes anserinus → 5 peripheral branches)
┌──────────────────────────────────────┐
Temporal Zygomatic Buccal Marginal Cervical
Key anatomical facts (Cummings):
- The labyrinthine segment has the smallest cross-sectional diameter and the narrowest bony canal — hence most susceptible to oedema and compression
- The geniculate ganglion is the most common site of injury in temporal bone fractures
- The nerve is dehiscent in up to 55% of normal temporal bones in the tympanic segment — a risk factor for inflammatory palsy and surgical injury
PART III: CAUSES OF TRAUMATIC FACIAL PALSY
CLASSIFICATION
TRAUMATIC FACIAL PALSY
├── A. BLUNT TRAUMA
│ ├── 1. Temporal Bone Fractures
│ │ ├── Longitudinal
│ │ ├── Transverse
│ │ ├── Mixed/Oblique
│ │ └── Otic Capsule Disrupting / Sparing
│ └── 2. Birth Trauma
│
├── B. PENETRATING TRAUMA
│ ├── 3. Gunshot/Blast injuries
│ ├── 4. Stab wounds / sharp facial lacerations
│ └── 5. Foreign body injuries
│
├── C. IATROGENIC TRAUMA
│ ├── 6. Parotid surgery
│ ├── 7. Mastoid & middle ear surgery
│ ├── 8. Skull base surgery
│ ├── 9. Neck dissection
│ ├── 10. Facelift / rhytidectomy
│ └── 11. Dental injections (inferior alveolar nerve block)
│
└── D. BIRTH TRAUMA
└── 12. Forceps delivery
A. TEMPORAL BONE FRACTURES (Most Common Cause)
Temporal bone fractures account for 7% of all skull fractures and facial nerve paralysis occurs in 7% of temporal bone fractures (up to 30% in otic capsule-disrupting fractures). — Cummings
TRADITIONAL CLASSIFICATION
| Feature | Longitudinal | Transverse |
|---|---|---|
| Frequency | 70–80% | 20–30% |
| Mechanism | Lateral blow (temporal/parietal) | Frontal/occipital blow |
| Fracture plane | Parallel to petrous ridge | Perpendicular to petrous ridge |
| FN palsy incidence | 20% | 50% |
| Onset of palsy | Usually delayed (oedema) | Usually immediate (laceration/avulsion) |
| Common FN site | Perigeniculate, tympanic | Labyrinthine, meatal foramen |
| Hearing loss | Conductive (TM, ossicular) | SNHL (cochlear/otic capsule) |
| Battle's sign | Present | Absent |
| Hemotympanum | Present | Less common |
| Vertigo | Mild, transient | Severe, prolonged |
| CSF otorrhea | Common | Less common |
MODERN CLASSIFICATION (Preferred — based on otic capsule involvement)
Otic Capsule Disrupting (OCD) — ~6% of temporal bone fractures
- Associated with facial nerve injury in 30–50% of cases
- SNHL, vestibular dysfunction
- Higher medico-legal significance
Otic Capsule Sparing (OCS) — ~94% of temporal bone fractures
- Facial palsy in 10%
- Conductive hearing loss more common
MECHANISMS OF INJURY IN TEMPORAL BONE FRACTURES
- Direct compression by bone fragment impinging on the nerve
- Intratemporal haematoma causing pressure necrosis
- Entrapment from bony compression in the fallopian canal
- Loss of continuity — complete transection (rare, ~5%)
- Oedema and demyelination — most common; similar histology to Bell's palsy (Grobman et al.)
- Devascularisation — disruption of vasa nervorum
- Traction injury — at the geniculate ganglion, caused by counter-distraction of anterior and posterior temporal bone fragments
Most vulnerable site: Labyrinthine segment → Geniculate ganglion — due to:
- Narrowest cross-sectional diameter in the fallopian canal
- Lacks fibrous supporting tissue
- Traction stress between Greater Petrosal Nerve and geniculate ganglion
B. PENETRATING INJURIES
Gunshot wounds to the temporal bone:
- Most severe form of facial nerve injury
- Causes loss of continuity in majority
- Complex trajectory; bone is often comminuted
- Requires surgical exploration in nearly all complete palsies
Stab wounds / facial lacerations:
- Extratemporal facial nerve branches
- Any branch peripheral to the parotid may be divided
- Posterior to a vertical line through the lateral canthus — branches large enough to repair primarily
Foreign bodies:
- Blast injuries with penetrating shrapnel
- Industrial accidents
C. IATROGENIC INJURY
1. Parotid Surgery
- Most feared complication of parotidectomy
- Temporary palsy — 15–20% of superficial parotidectomies; resolves in weeks to months
- Permanent palsy — 1–2%
- Marginal mandibular and frontal branches most at risk
- Causes: excessive retraction, thermal injury from electrocautery, devascularisation, inadvertent division
2. Middle Ear & Mastoid Surgery
- Risk highest during:
- Canal wall down mastoidectomy (posterior genu)
- Stapedectomy (horizontal segment dehiscence)
- Tympanoplasty
- Cholesteatoma — may erode fallopian canal, making nerve vulnerable
- Prompt recognition: if discovered intraoperatively → decompress and administer steroids
3. Skull Base Surgery
- Acoustic neuroma (vestibular schwannoma) resection — FN is at greatest risk
- Jugular foramen tumour surgery
- Middle and posterior cranial fossa approaches
4. Neck Dissection
- Marginal mandibular branch at risk during ligation of facial vein
- Retromandibular vein is a surgical landmark
5. Facelift (Rhytidectomy)
- Temporal and zygomatic branches at risk in SMAS plane dissection
- Frontal branch — at risk crossing zygomatic arch
6. Dental Injections
- Inferior alveolar nerve block — accidental injection into parotid
- Causes temporary (1–3 hours) ipsilateral facial weakness
- No treatment needed
D. BIRTH TRAUMA
- Forceps delivery → compression of facial nerve at stylomastoid foramen (nerve superficial in neonates, no mastoid tip protection)
- Incidence: ~0.25% of forceps deliveries
- Usually incomplete palsy; nearly always recovers spontaneously
- Must be distinguished from Möbius syndrome (congenital bilateral FN agenesis/aplasia)
PART IV: CLINICAL EVALUATION
History
- Onset: Immediate vs. Delayed
- Immediate → direct structural injury (nerve transection/compression by bony fragment)
- Delayed → oedema/haematoma with evolving neurapraxia; better prognosis
- Mechanism and severity of trauma
- LOC, associated neurological deficit
- Previous medications (paralytic agents may mask early assessment)
Physical Examination
- Full HB grading
- Eye closure, brow movement, nasolabial fold, corner of mouth
- Associated features: hemotympanum, CSF otorrhea (otorrhagia), Battle's sign, raccoon eyes
- Tuning fork tests, otoscopy
- Check for nystagmus (labyrinthine involvement)
- Note: "Differentiation of delayed onset from delayed diagnosis is crucial" — Cummings
Topognostic Tests (Localisation of Lesion Site)
(Now largely replaced by electrical testing and HRCT)
| Test | Nerve Function Assessed | Level |
|---|---|---|
| Schirmer's test | Lacrimation (Greater Petrosal N.) | Above geniculate ganglion |
| Taste (electrogustometry) | Chorda tympani | Above nerve to stapedius |
| Stapedial reflex | Nerve to stapedius | Above chorda tympani |
| Salivary flow test | Chorda tympani | Above chorda tympani |
PART V: INVESTIGATIONS
A. Electrodiagnostic Tests
1. Electroneuronography (ENoG) — MOST IMPORTANT
- Stimulates facial nerve at stylomastoid foramen; records compound muscle action potential (CMAP)
- Compares amplitude of affected vs. normal side
- >90% degeneration within 6 days = criterion for surgery (Fisch's criterion)
- Most useful Days 3–21 after injury (wallerian degeneration needs 72 hours)
- Not valid in long-standing paralysis
2. Electromyography (EMG)
- Detects voluntary motor unit potentials (MUPs) — indicates viable axons
- Fibrillation potentials = denervation (appear 10–14 days after injury)
- Polyphasic reinnervation potentials = recovery (appear before clinical improvement)
- Useful for: long-standing paralysis, monitoring recovery
3. Maximum Stimulation Test (MST) / Nerve Excitability Test (NET)
- Older, less quantitative
- NET: Minimum current required for visible muscle twitch
- Difference >3.5 mA suggests significant degeneration
- MST: Maximum current stimulation — no visible response = poor prognosis
B. Imaging
High-Resolution CT (HRCT) of Temporal Bone — GOLD STANDARD
- Axial and coronal cuts at 0.5 mm slices
- Identifies:
- Fracture lines through fallopian canal
- Widening/narrowing of the canal
- Displaced bone fragments
- Otic capsule involvement
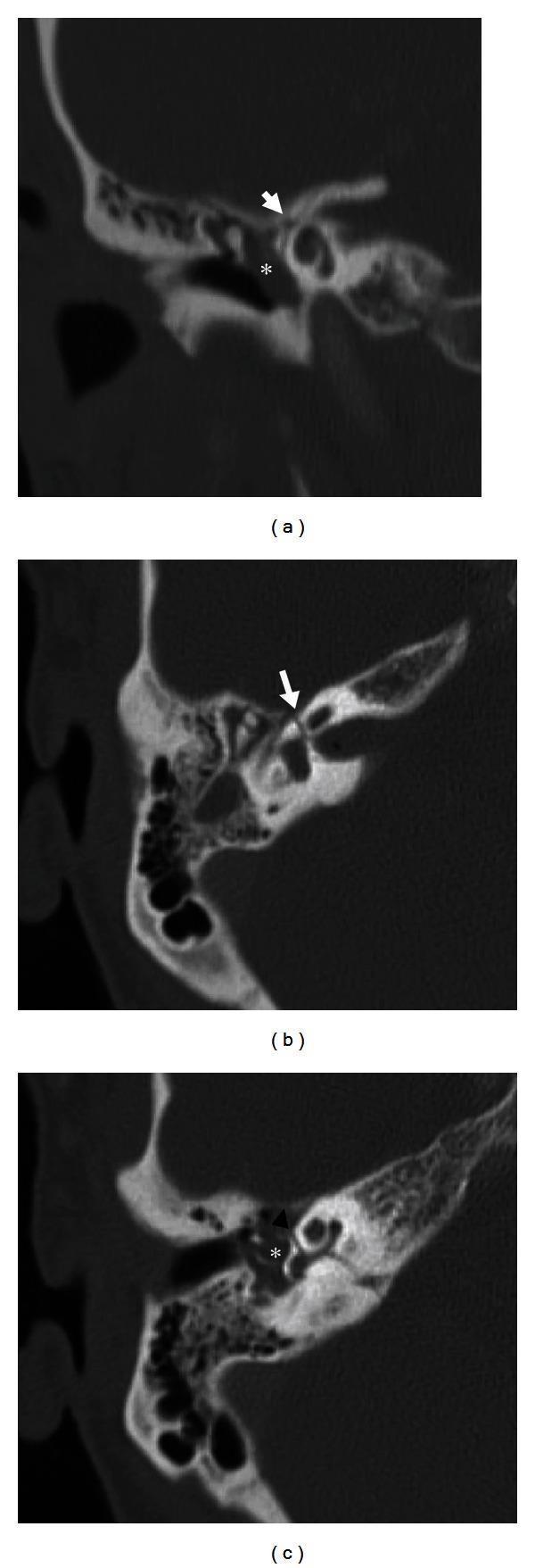
Fig: Multiplanar HRCT showing transverse temporal bone fracture. Arrows indicate fracture lines intersecting the labyrinthine segment of the facial nerve canal; asterisks indicate hemotympanum.
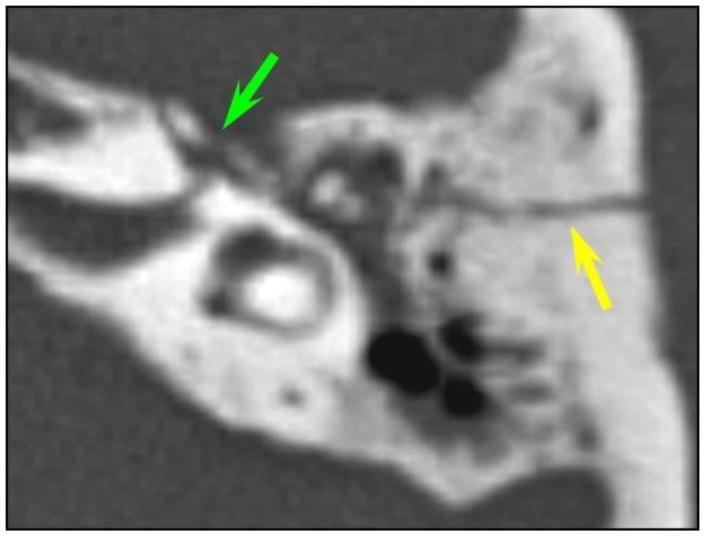
Fig: Axial HRCT — longitudinal fracture line (yellow arrow) with bone fragments at geniculate ganglion fossa (green arrow), the most common site of facial nerve injury in temporal bone trauma.
Accuracy of HRCT (Yan et al.):
- Most accurate at: geniculate ganglion and labyrinthine segment
- Underestimates: mastoid and pyramid segment injuries
- Most intraoperative findings show nerve oedema, not transection
MRI
- Gadolinium-enhanced MRI: enhancement of facial nerve = oedema/inflammation
- Role: when HRCT inconclusive; to evaluate intracranial extension or soft tissue injury
- Not first-line in acute trauma
PART VI: MANAGEMENT
MANAGEMENT FLOWCHART
TRAUMATIC FACIAL PALSY DIAGNOSED
|
▼
ASSESS ONSET OF PARALYSIS
|
┌─────┴───────┐
IMMEDIATE DELAYED
onset onset
| |
▼ ▼
HIGH-RESOLUTION CT CONSERVATIVE
TEMPORAL BONE (steroids +
+ ENoG eye care)
| |
Fracture No | Spontaneous
through fracture Worsening? recovery?
FN canal on CT (ENoG >90% → OBSERVE
| | in 6 days) & MONITOR
| ▼ | with EMG
| Conservative YES
| Management |
| ▼
└────────────→ SURGICAL EXPLORATION
|
┌────────────┼─────────────────┐
▼ ▼ ▼
Nerve intact Nerve compressed Nerve
(oedema only) by bone/haematoma DIVIDED
| | |
Decompress Remove bony ┌───┴────┐
fallopian fragments + <3cm gap >3cm gap
canal decompress | |
| | Primary end- Cable graft
▼ ▼ to-end repair (sural n./
CLOSE DECOMPRESS (epineural) GAN/ANSA)
A. NON-OPERATIVE (CONSERVATIVE) MANAGEMENT
Indications:
- Delayed-onset facial palsy (most recover spontaneously)
- Incomplete paralysis (any grade) — virtually always recovers
- Immediate-onset palsy with <90% degeneration on ENoG
- Patient unfit for surgery
McKennan & Chole (Am J Otol 1992): Excellent recovery in delayed-onset paralysis managed non-surgically. — Cummings
Maiman et al. (J Trauma 1985): Of 45 patients managed non-operatively, 44 had satisfactory recovery and 65% had complete recovery.
Conservative Management Protocol
1. Systemic Corticosteroids
- Reduce intratemporal oedema
- Prednisolone 1 mg/kg/day (max 60 mg) × 7–10 days, then taper
- Initiated as soon as safely possible
- Contraindicated if severe head injury / raised ICP
2. Eye Care (CRITICAL — prevents exposure keratopathy)
- Artificial tear drops — every 2 hours when awake
- Lubricating eye ointment at night
- Protective spectacles / moisture chamber glasses
- Taping the eye shut at night (micropore / Tegaderm)
- If grade V–VI: temporary tarsoraphy or gold weight implant (upper eyelid)
3. Physiotherapy / Facial Exercises
- Biofeedback-assisted facial retraining
- Neuromuscular re-education
- Massage of facial muscles
- Begin once reinnervation potentials appear on EMG
4. Observation and Serial ENoG
- Serial ENoG at 3, 6, and 14 days
- If <90% degeneration at 6 days → continue conservative management
- If >90% degeneration at 6 days → reconsider surgical decompression
B. SURGICAL MANAGEMENT
INDICATIONS FOR SURGERY (Cummings, Fisch criteria)
| Indication | Rationale |
|---|---|
| Immediate-onset complete palsy with HRCT fracture through FN canal | High likelihood of structural injury |
| ENoG >90% degeneration within 6 days of injury | Fisch criterion — predicts poor spontaneous recovery |
| Penetrating injury (gunshot wound, stab) | Direct transection likely |
| No clinical or EMG improvement at 12 months | Long-standing palsy |
| Evidence of nerve transection on HRCT/MRI | Requires cable grafting |
Adegbite et al. (controversial): Outcome predicted by severity of paralysis, not manner of onset. — Cummings
Chang & Cass emphasised that natural history, appropriate timing, and reporting criteria must be considered in judging efficacy of surgical decompression. — Cummings
TIMING OF SURGERY
- For immediate-onset complete palsy: Surgery within 2–3 weeks preferred
- Delaying up to 3 weeks may be advantageous — allows resolution of oedema/haematoma, making surgical field clearer
- For long-standing paralysis: Explore at 12 months if no recovery on EMG
- In penetrating injuries: Explore as soon as medically stable (within days)
SURGICAL APPROACHES
SITE OF INJURY ON HRCT/ENoG
|
┌──────┴───────────────┐
Labyrinthine/ Mastoid/
Geniculate/ Tympanic
Tympanic segment segment
| |
MIDDLE CRANIAL TRANSMASTOID
FOSSA APPROACH ±
(if hearing POSTERIOR TYMPANOTOMY
preserved)
| |
└──────────┬────────────┘
▼
COMBINED APPROACH
(Middle Cranial Fossa +
Transmastoid/
Translabyrinthine)
— when hearing lost —
A. Transmastoid Approach
- For mastoid segment (vertical) injuries
- Also allows access to tympanic segment via posterior tympanotomy
- Decompresses nerve from second genu to stylomastoid foramen
B. Middle Cranial Fossa (MCF) Approach
- For labyrinthine segment and geniculate ganglion injuries
- Hearing preservation approach
- Technically demanding; requires neurotological expertise
- Risks: temporal lobe retraction, CSF leak, epidural haematoma
C. Translabyrinthine Approach
- When hearing is already destroyed (e.g., transverse fracture with SNHL)
- Excellent access to entire intratemporal segment
- Sacrifices cochlea/vestibule
- Least risk to brain
INTRAOPERATIVE MANAGEMENT
i. Decompression
- For oedema/haematoma without nerve transection
- Remove bone of fallopian canal with diamond burr for 270° circumference
- Slit the epineurium (epineuriotomy) to release intraneural pressure
- "Approach from proximal and distal uninvolved segments toward diseased area" (Cummings)
- Use flat, blunt instruments to dissect granulation tissue from nerve
- Avoid sharp dissection at epineurium unless absolutely necessary
ii. Primary Neurorrhaphy (End-to-End Repair)
- For transected nerve with gap <3 mm (after freshening ends)
- Tension-free anastomosis essential
- Epineural repair — suturing epineurium, 8-0 or 9-0 nylon/prolene
- Best results if performed within 72 hours of injury (acute repair) or after minimal delay
iii. Interposition Cable Graft
- For gaps >3 mm after transection
- Donor nerves:
- Greater Auricular Nerve (GAN) — most commonly used; provides ~7 cm; harvested from neck
- Sural Nerve — provides up to 30–40 cm; used for longer defects
- Ansa cervicalis
- Medial cutaneous nerve of forearm
- Graft is reversed (to avoid axonal escape at branches)
- Anastomosed epineurially at each end
- Expected recovery: HB Grade III in 60–70% of patients
C. MANAGEMENT OF LONG-STANDING/ESTABLISHED PALSY
When nerve degeneration is complete and >12–18 months have elapsed, direct nerve repair is unlikely to succeed. Reanimation procedures are required:
Static Procedures (Immediate symmetry at rest)
- Fascial sling — tensor fascia lata sling to angle of mouth
- Brow lift — frontalis sling or brow suspension
- Gold weight implant (upper eyelid) — for lagophthalmos; 0.6–1.6 g
- Lower eyelid tightening — lateral tarsal strip
- Tarsoraphy — temporary or permanent
Dynamic Procedures (Restore voluntary movement)
-
Nerve substitution (XII–VII anastomosis)
- Hypoglossal–facial nerve anastomosis
- Provides resting tone and bulk to face
- Tongue hemiatrophy is major drawback
- Partial XII–VII: splits hypoglossal nerve — reduces morbidity
-
Cross-facial nerve graft (CFNG)
- Sural nerve graft tunnelled across face
- Takes axons from contralateral healthy VII branches
- Allows spontaneous, emotive facial movement
- Takes 9–12 months for axonal growth; two-stage procedure
-
Microneurovascular free muscle transfer (gold standard for long-standing)
- Gracilis free flap with obturator nerve anastomosed to CFNG or masseter nerve
- Provides true voluntary and spontaneous movement
- Can be powered by masseter nerve (single-stage) or CFNG (two-stage)
-
Temporalis muscle transposition (modified Gillies procedure)
- Temporalis muscle slip rotated and attached to angle of mouth
- Utilises trigeminal (V) nerve input
- Simple, reliable, no microsurgery
- Drawback: requires deliberate jaw-clenching for movement (synkinesis)
-
Masseter–facial nerve anastomosis (V–VII)
- Masseteric branch of V3 anastomosed to main trunk or buccal branch
- Strong reinnervation; minimal donor defect
- Patient learns to clench jaw for facial movement
- Recent advance: Combination of masseteric nerve + CFNG (babysitter procedure)
D. EYE MANAGEMENT IN DETAIL
This is the most urgent aspect of management — corneal exposure leads to irreversible blindness.
LAGOPHTHALMOS ASSESSMENT
|
┌─────┴───────┐
<3mm gap >3mm gap
at gentle or poor Bell's
closure phenomenon
| |
Lubricants Add moisture
q2h chamber + night
taping
|
No improvement /
permanent palsy
|
┌─────┴───────┐
Temporary Permanent
tarsoraphy gold weight
(reversible) implant +
lower lid
tightening
PART VII: ALGORITHM — COMPLETE MANAGEMENT SUMMARY
TRAUMA → FACIAL WEAKNESS DETECTED
↓
IMMEDIATE HISTORY & EXAMINATION
(HB Grade, mechanism, onset timing)
↓
HRCT TEMPORAL BONE (axial + coronal)
↓
┌─────────┴──────────┐
INCOMPLETE COMPLETE PALSY
PALSY (HB V–VI)
| |
Conservative Determine ONSET
(steroids, (Immediate vs Delayed)
eye care) |
| ┌──────┴──────────┐
Monitor IMMEDIATE DELAYED
with ENoG (day 0) (>24 hrs)
| |
ENoG Day 3–6 Conservative
| (steroids, serial
<90% deg. >90% deg. ENoG monitoring)
| | |
Continue SURGERY Worsens to
conservative >90% ENoG?
|
CONSIDER SURGERY
|
┌───────────────┼────────────────┐
Intact Compressed Transected
nerve nerve nerve
(oedema) (fragment/ (<3mm gap vs
haematoma) >3mm gap)
| | |
Decompress Remove fragments Primary repair
fallopian + Decompress vs Cable graft
canal (GAN/Sural)
↓
POST-OP EYE CARE + FACIAL REHABILITATION
PART VIII: RECENT ADVANCES
1. Intraoperative Facial Nerve Monitoring (IONM)
- Continuous EMG monitoring of facial muscles during temporal bone/skull base surgery
- Reduces iatrogenic injury significantly
- Alert surgeon to proximity of the nerve
- Real-time neurotonic discharges indicate mechanical irritation
2. Robot-Assisted Surgery
- Robotic systems (da Vinci) allow precision in parotid surgery, reducing iatrogenic FNP
- Minimally invasive approach to parotid lesions — currently in trials
3. Gabapentin / Pregabalin in Neuropathic Pain
- Post-traumatic synkinesis and aberrant regeneration pain management
- Used alongside botulinum toxin therapy
4. Botulinum Toxin Type A (BTX-A)
- Management of synkinesis after recovery (aberrant reinnervation)
- Also used to balance the contralateral hyperactive face in longstanding palsy
- Injected into hyperactive muscles (orbicularis, mentalis, platysma)
5. Masseteric Nerve (Motor Branch of V3) — "Babysitter Procedure"
- Rapid reinnervation of the facial musculature
- Combining masseteric nerve with cross-facial nerve graft allows both early reinnervation AND spontaneous emotional movement
- Published by Biglioli et al., Terzis & Olivares — becoming gold standard in paralysis >2 years
6. Selective Neurectomy for Synkinesis
- Division of nerve branches causing involuntary movements
- Combined with BTX-A and physical therapy
7. Regenerative Medicine & Nerve Conduits
- Biodegradable nerve conduits (collagen, polyglycolic acid) for nerve gaps
- Growth factor delivery (BDNF, NGF) to enhance axonal regeneration
- Stem cell-seeded scaffolds — experimental
8. 3D Printing in Facial Reanimation
- Custom-fabricated static slings
- Patient-specific implants for facial symmetry
9. Validated Outcome Tools
- eFACE (electronic, clinician-rated)
- FACE-Q (patient-reported outcomes)
- Sunnybrook Facial Grading System — regional scoring with synkinesis assessment
- Replacing the older, less sensitive HB scale in research settings
10. Diffusion Tensor Imaging (DTI-MRI)
- Tractography of the facial nerve in the temporal bone
- Allows pre-surgical mapping without radiation
- Still investigational; promising for planning decompression
PART IX: PROGNOSIS
| Factor | Good Prognosis | Poor Prognosis |
|---|---|---|
| Onset | Delayed | Immediate |
| Degree | Incomplete | Complete |
| ENoG at 6 days | <90% degeneration | >90% degeneration |
| EMG | Voluntary MUPs present | Fibrillation potentials only |
| CT | No fracture through FN canal | Fracture/fragment in canal |
| Type of fracture | Longitudinal (OCS) | Transverse (OCD) |
| Cause | Blunt (oedema only) | Penetrating (transection) |
| Age | Younger | Older |
Natural history (conservative management):
- Incomplete palsy → virtually 100% complete recovery
- Complete delayed-onset palsy → >90% good recovery (HB I–II)
- Complete immediate-onset palsy → ~50% full recovery without surgery; up to 70% with timely decompression
PART X: KEY REFERENCES
| Author/Book | Contribution |
|---|---|
| Cummings Otolaryngology HNS, 6e | Comprehensive algorithm for traumatic FNP; ENoG criteria; Fisch criterion |
| Scott-Brown's Otorhinolaryngology, 8e | Classification, topognostic tests, management approaches |
| KJ Lee's Essential Otolaryngology | Practical management of post-paralysis FNP |
| Dhingra's Diseases of ENT | Undergraduate-level classification and approach |
| Hazarika's Textbook of ENT | Indian surgical perspective, anatomy emphasis |
| Stell & Maran | Anatomical classification of FNP causes |
| Fisch U (1979) | ENoG criterion (>90% degeneration in 6 days) for surgery |
| McKennan & Chole (1992) | Non-surgical management of temporal bone trauma FNP |
| Maiman et al. (1985) | Non-operative management outcomes |
| Adegbite et al. | Severity, not onset, predicts outcome |
| Chang & Cass | Review of surgical vs expectant management |
| Biglioli et al. | Masseteric nerve babysitter procedure |
| Yan et al. | HRCT accuracy for fallopian canal fracture |
SUMMARY TABLE
| Parameter | Detail |
|---|---|
| Most common cause | Temporal bone fracture (longitudinal) |
| Most vulnerable FN segment | Labyrinthine / Geniculate ganglion |
| Best investigation | HRCT temporal bone + ENoG |
| Surgery criterion (Fisch) | ENoG >90% degeneration within 6 days |
| Approach for labyrinthine injury | Middle cranial fossa |
| Approach for mastoid injury | Transmastoid |
| Best graft for short gap | Greater auricular nerve |
| Best for long-standing palsy | Gracilis free flap + masseteric nerve |
| Most urgent aspect | Eye care (prevent exposure keratopathy) |
| Recent gold standard — late palsy | Masseteric nerve + CFNG (babysitter) |
Note on diagrams: Thegenerate_imagetool has reached its monthly limit on this subscription plan. The detailed ASCII flowcharts, classification tables, and anatomical course diagram above serve as comprehensive substitutes. Please contact support or upgrade your plan to restore AI diagram generation for future questions.
Sources: Cummings Otolaryngology HNS 6e (blocks 31, 32, 38, 39) | KJ Lee's Essential Otolaryngology | Intraoperative surgical anatomy images from PMC Clinical VQA | HRCT temporal bone fracture images from medical literature
This is a shared conversation. Sign in to Orris to start your own chat.