Histologic types of hodgkins lymphoma
Reading File
Finding Sources
Searching PubMed
"Hodgkin lymphoma" AND "histologic subtypes"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from both Robbins Pathology and Henry's Clinical Diagnosis. Let me compile the full answer.
Histologic Types of Hodgkin Lymphoma
The WHO classification recognizes 5 subtypes of Hodgkin lymphoma (HL), divided into two major categories based on the nature of the neoplastic cell.
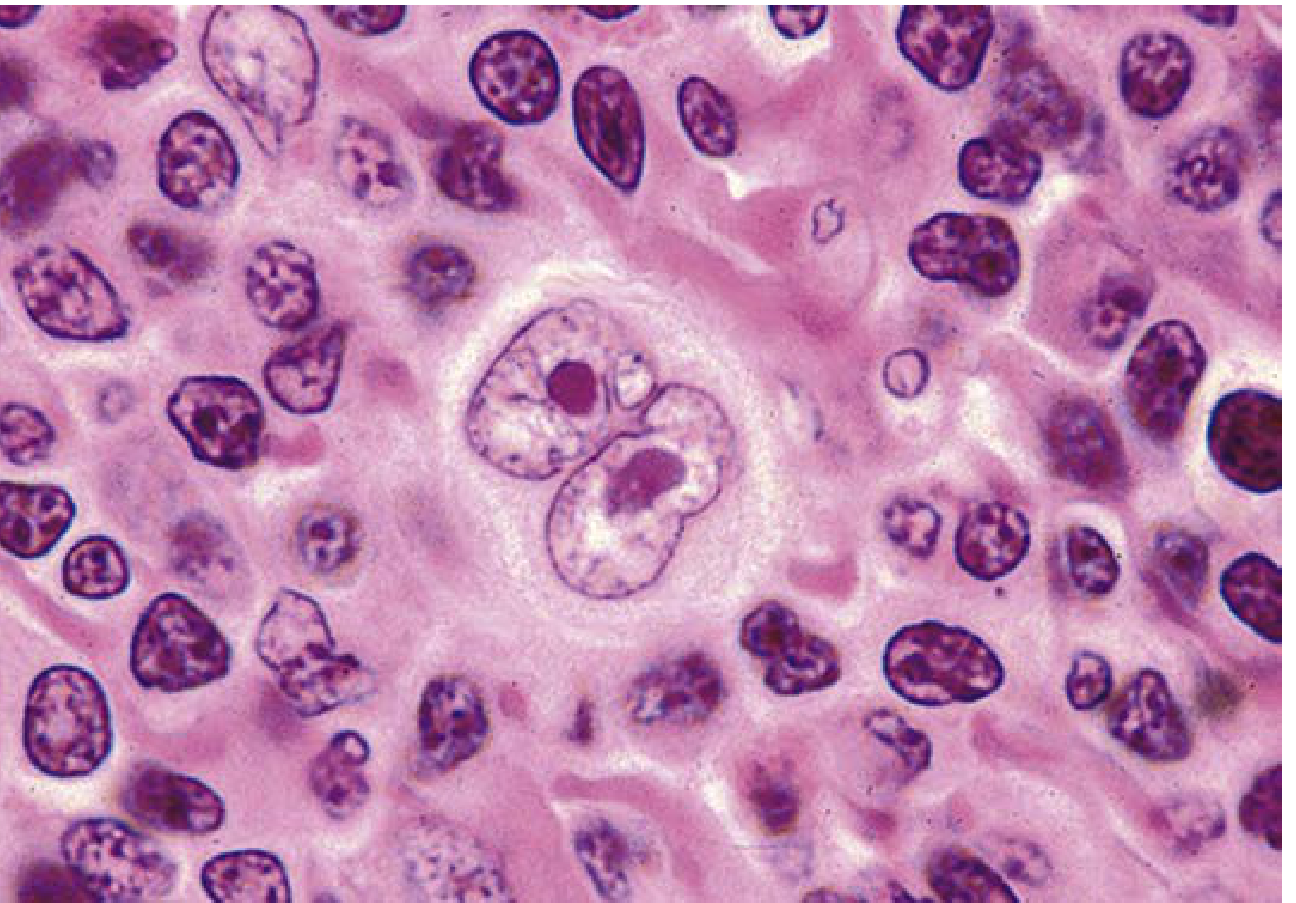
The Reed-Sternberg (RS) Cell - The Hallmark
The RS cell is the diagnostic sine qua non of all HL subtypes. It is a very large cell (15-45 µm) with an enormous multilobate nucleus, exceptionally prominent nucleoli, and abundant pale eosinophilic cytoplasm. The classic RS cell has two mirror-image nuclei or nuclear lobes, each with a large owl-eye nucleolus surrounded by a clear halo - giving the classic "owl-eye" appearance.
Category 1: Classic Hodgkin Lymphoma (cHL)
The first four subtypes share the same neoplastic cell (the HRS cell) with identical immunophenotype: CD15+, CD30+, CD45-, B-cell markers negative or weak, PAX5+, MUM1+. EBV is associated with a significant proportion of cases.
1. Nodular Sclerosis (NS-HL)
Most common subtype (~65-70% of cases)
| Feature | Detail |
|---|---|
| Age/Sex | Adolescents and young adults; equal M = F |
| Typical site | Lower cervical, supraclavicular, mediastinal lymph nodes |
| Stage at presentation | Usually stage II |
| EBV association | Low (~10-15%) |
| Prognosis | Excellent |
Histology:
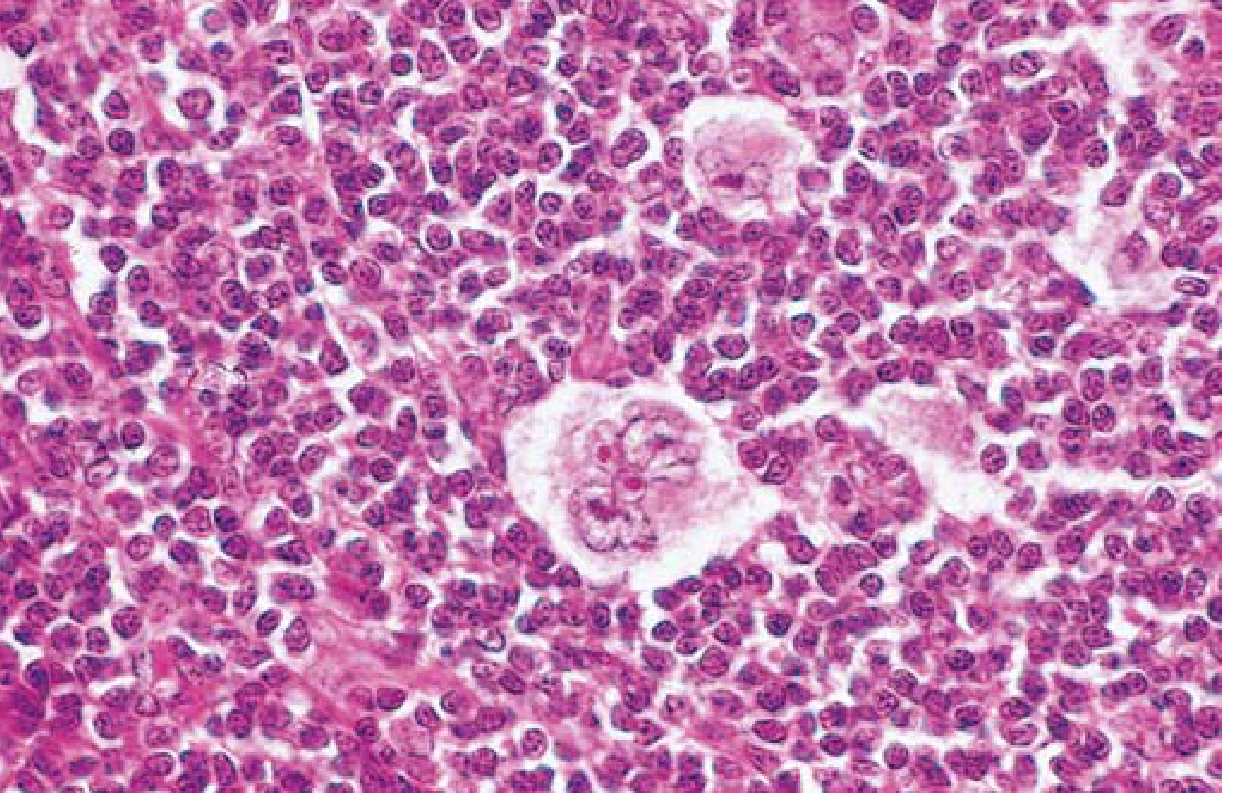
- Lacunar cells - the characteristic RS variant. These have a single multilobate nucleus with multiple small nucleoli and abundant pale cytoplasm. In formalin-fixed tissue, the cytoplasm retracts, leaving the nucleus sitting in an empty "lacune" (space).
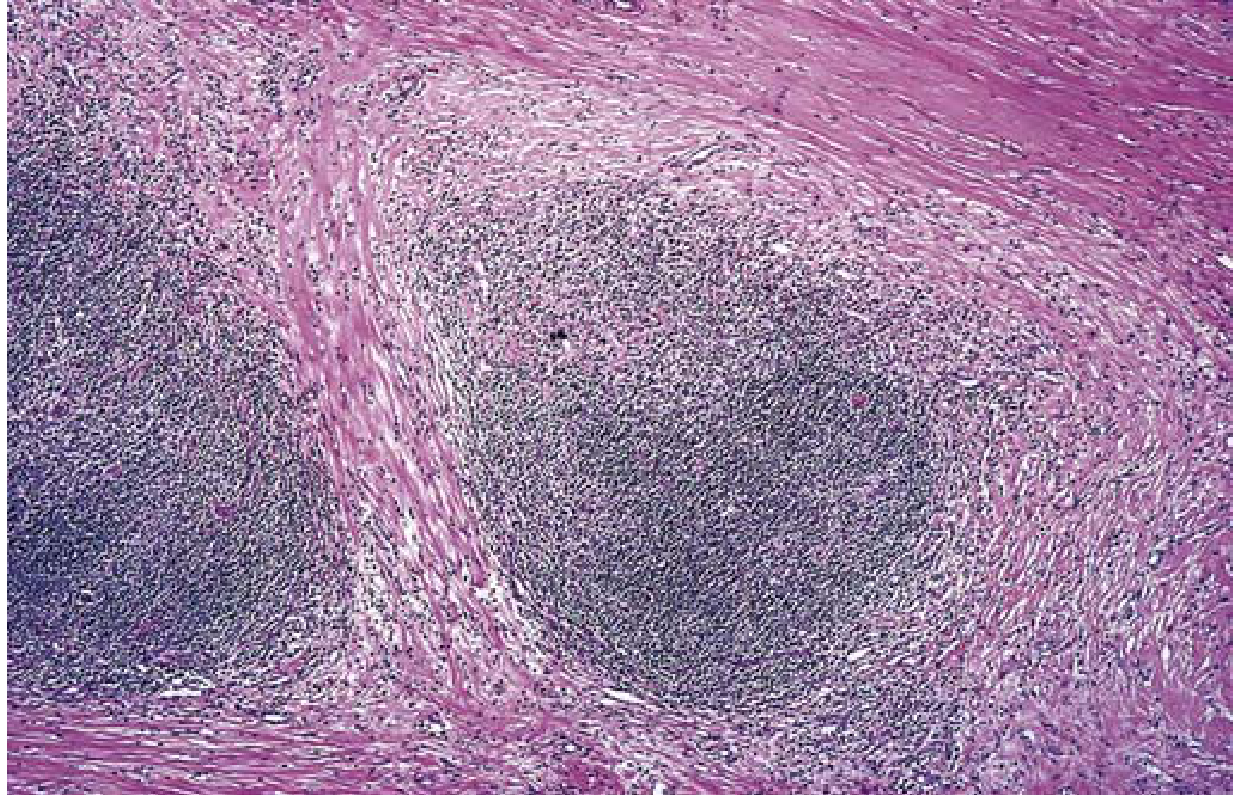
- Broad bands of collagen that divide the lymphoid tissue into circumscribed cellular nodules - this is what gives the subtype its name.
- Background: lymphocytes, eosinophils, macrophages.
- Grading: Grade 2 (syncytial variant) when sheets of neoplastic cells occupy ≥25% of nodules, often associated with necrosis.
2. Mixed Cellularity (MC-HL)
Second most common (~25% of cases)
| Feature | Detail |
|---|---|
| Age/Sex | Most common subtype in patients >50 years; male predominance |
| EBV association | Highest - up to 70% of cases |
| Stage | More often disseminated |
| Prognosis | Still very good |
Histology:
- Classic RS cells are plentiful - this is the subtype where you see the most "textbook" owl-eye RS cells.
- Diffuse polymorphic infiltrate: small lymphocytes, eosinophils, plasma cells, histiocytes, and RS cells.
- No collagen bands (unlike NS).
- Necrosis and disorderly fibrosis may be present.
- More likely to present with B symptoms and systemic manifestations than NS.
3. Lymphocyte-Rich (LR-HL)
Uncommon subtype (~5%)
| Feature | Detail |
|---|---|
| Background | Abundant lymphocytes with few other reactive cells |
| RS cells | Classic RS cells present but may be sparse |
| Prognosis | Favorable |
Histology:
- Diagnostic RS cells with classic cHL immunophenotype (CD15+, CD30+).
- Background dominated by lymphocytes; eosinophils and plasma cells are scarce.
- Defined by the tissue reaction (lymphocyte predominance) but RS cells have classic cHL immunophenotype - distinguishing this from NLPHL is important and requires immunohistochemistry.
4. Lymphocyte Depletion (LD-HL)
Rarest classic subtype (<1%)
| Feature | Detail |
|---|---|
| Age | Older patients; may be associated with HIV |
| Presentation | Often presents with advanced stage; B symptoms common; bone marrow involvement frequent |
| EBV association | High |
| Prognosis | Worst of the classic subtypes |
Histology:
- Neoplastic cells predominate; lymphocytes are relatively diminished (the opposite of lymphocyte-rich).
- Two patterns: diffuse fibrosis (paucicellular, hypocellular stroma with fibrosis) or reticular pattern (sheets of pleomorphic RS cells and variants).
- Normocytic anemia in ~50% of cases.
- BM involvement is common; lymphocytosis and thrombocytosis (seen in other HL subtypes) are usually absent.
Category 2: Nodular Lymphocyte-Predominant HL (NLPHL)
~5% of all HL cases - a biologically distinct entity
| Feature | Detail |
|---|---|
| Age/Sex | Males 30-50 years predominantly |
| Typical site | Peripheral lymphadenopathy (cervical, axillary) - mediastinal involvement is rare |
| EBV association | Absent |
| Prognosis | Excellent, even for stages I and II |
Histology:
- Architecture effaced by a nodular infiltrate of small B cells with an associated follicular dendritic network.
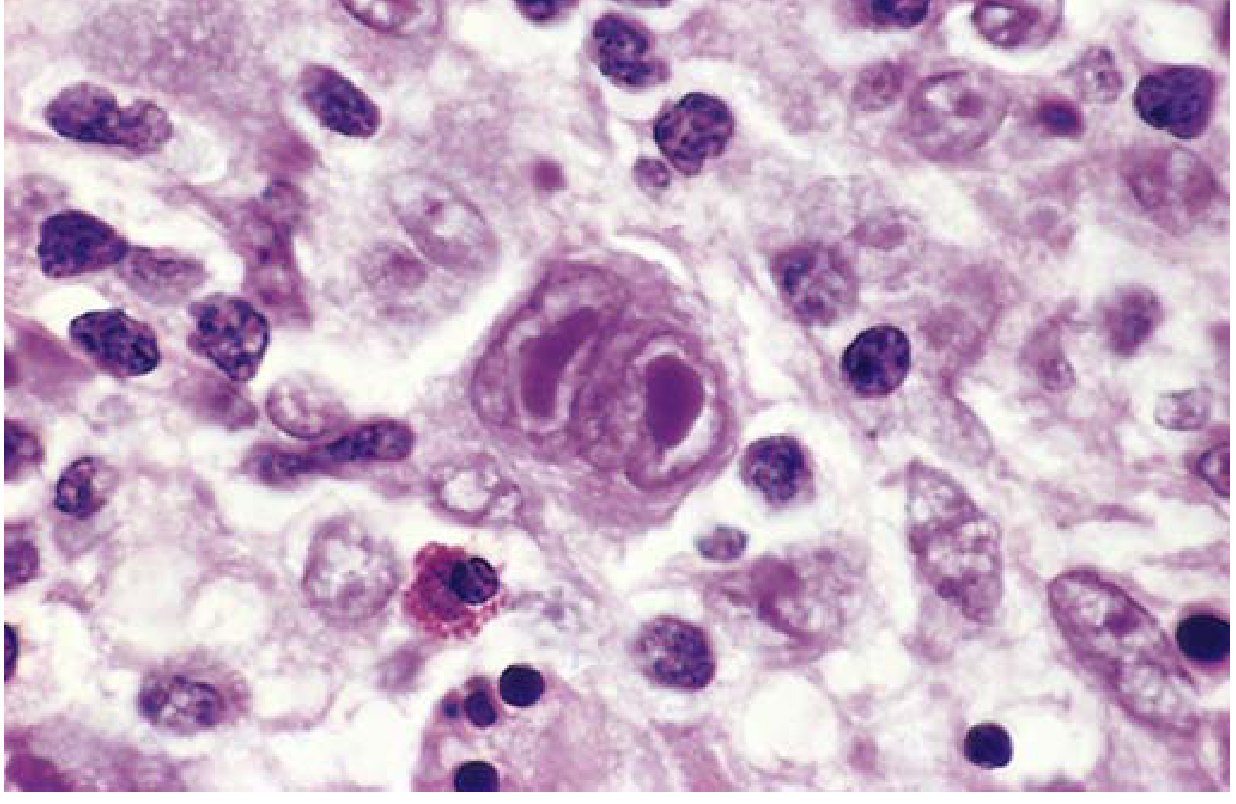
- The neoplastic cells are L&H (lymphocytic and histiocytic) cells, also called "popcorn cells" - large cells with delicate, multilobed nuclei with vesicular chromatin resembling popped popcorn. Nucleoli are less prominent than in classic RS cells.
- Classic RS cells are rare.
- Background: predominantly small B cells; CD3+/CD57+ T cells form rosettes around L&H cells (diagnostically helpful).
- Six immunoarchitectural patterns have been recognized.
Immunophenotype of L&H (popcorn) cells - completely different from cHL:
| Marker | NLPHL (L&H cells) | Classic HL (HRS cells) |
|---|---|---|
| CD20 | Positive | Negative/weak |
| CD45 | Positive | Negative |
| CD30 | Absent/weak | Positive |
| CD15 | Absent | Positive |
| BCL-6 | Positive | Negative |
| Oct2, BOB.1 | Positive | Absent |
| EMA | Often positive | Negative |
Summary Comparison Table
| Subtype | Frequency | RS Cell Variant | Key Morphology | EBV | Prognosis |
|---|---|---|---|---|---|
| Nodular Sclerosis | 65-70% | Lacunar cell | Collagen bands + nodules | Low | Excellent |
| Mixed Cellularity | ~25% | Classic RS (owl-eye) | Diffuse polymorphic infiltrate | High (70%) | Very good |
| Lymphocyte-Rich | ~5% | Classic RS | Lymphocyte-dominant background | Low | Favorable |
| Lymphocyte Depletion | <1% | Pleomorphic/rare RS | Few lymphocytes; neoplastic cells predominate | High | Worst of cHL |
| NLPHL | ~5% | Popcorn cell (L&H) | Nodular; B-cell background; T-cell rosettes | Absent | Excellent |
Key Pathogenetic Points
- All HL subtypes originate from germinal center B cells (proven by identical IgH gene rearrangements with somatic hypermutation in single microdissected RS cells).
- Classic cHL RS cells escape immune surveillance by: (1) losing β2-microglobulin/MHC-I expression, and (2) overexpressing PD-L1/PD-L2 - the basis for the dramatic response to anti-PD-1 therapy (e.g., pembrolizumab, nivolumab).
- RS cells secrete IL-5 (eosinophil recruitment), TGF-β (fibrosis), and IL-13 (autocrine growth).
Sources: Robbins & Kumar Basic Pathology (9780323790185), p. 417-420; Henry's Clinical Diagnosis and Management by Laboratory Methods (9780323673204), p. 770-772
This is a shared conversation. Sign in to Orris to start your own chat.