Asthma and obesity full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"asthma" AND "obesity" AND "pathophysiology"
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive MD exam answer. Let me compile it.
Asthma and Obesity - Comprehensive MD Exam Answer (10 Marks)
Introduction
Obesity (BMI >30 kg/m²) and asthma are two of the fastest-growing global health burdens. Their association is bidirectional - obesity is a risk factor for developing asthma, and asthma is independently a risk factor for developing obesity. This coexistence creates a distinct, severe, difficult-to-treat clinical phenotype that demands specific understanding.
Epidemiology:
- Obese women aged 26-46 years have a threefold increased risk of developing asthma compared to lean women (Camargo et al.)
- Asthma incidence is 50% higher in overweight/obese individuals vs. normal-weight individuals
- Asthma prevalence in the USA: lean adults 7.1%, overweight 7.8%, obese 11.1%
- When BMI exceeds 60, asthma frequency may exceed 30%
- Children with early-onset asthma at age 4 have double the risk of developing obesity by age 8
- Up to 25% of new childhood asthma cases are attributable to obesity
- Nearly 60% of patients with severe asthma in the USA are obese
Pathophysiology
Figure: The Interaction of Obesity and Asthma
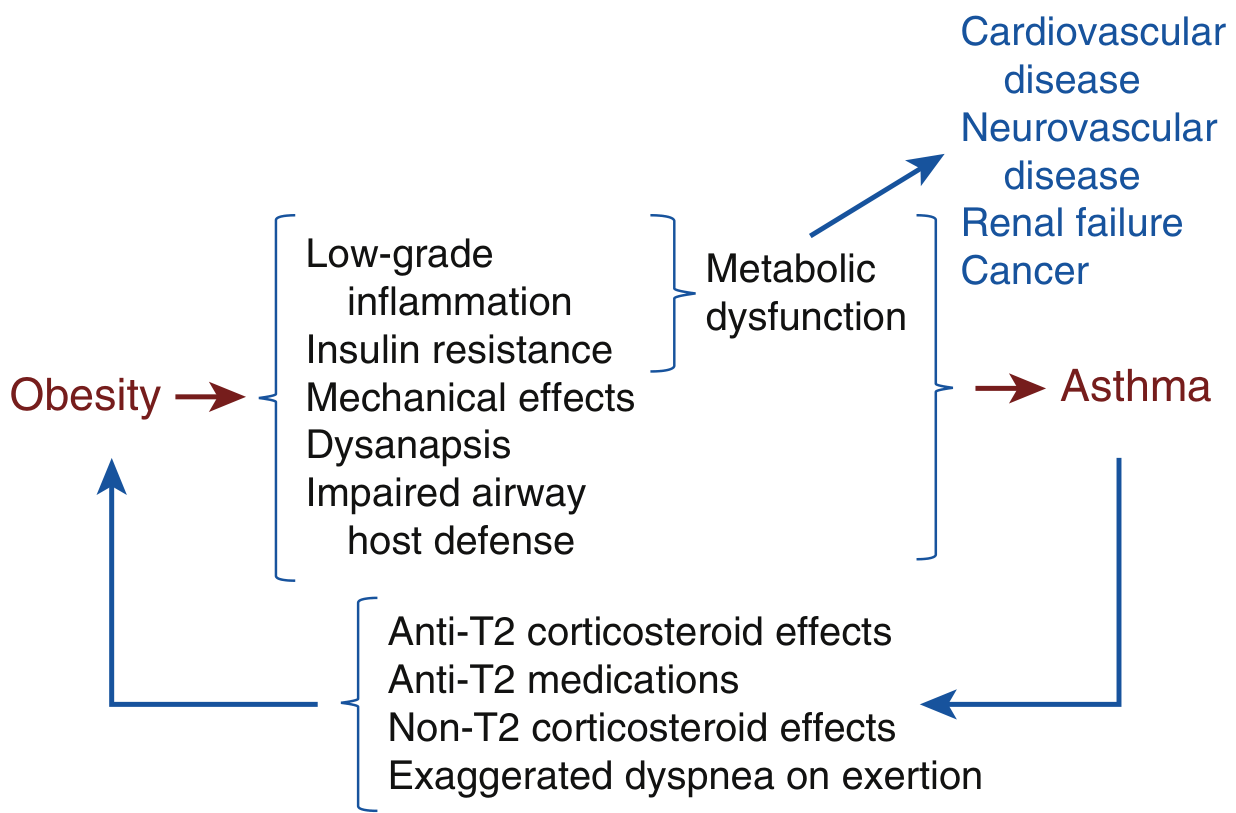
Figure 61.1 - Murray & Nadel's Textbook of Respiratory Medicine: Excessive visceral adipose tissue leads to metabolic dysfunction (chronic low-grade inflammation + insulin resistance) which drives asthma risk. Asthma and its therapies (anti-T2 drugs, corticosteroids) in turn increase obesity risk.
1. Metabolic Dysfunction and Systemic Inflammation (Meta-Inflammation)
Excessive visceral adipose tissue causes two key derangements:
- Chronic low-grade systemic inflammation (meta-inflammation): elevated pro-inflammatory cytokines - IL-6, IL-1, TNF-α, and leptin
- Insulin resistance: impaired glucose uptake in muscle, fat, and liver - leading to hyperinsulinemia and eventually diabetes
Clinical relevance: Elevated systemic IL-6 is repeatedly associated with lower lung function, worse asthma symptoms, and higher exacerbation rates. These patients also have higher rates of hypertension, diabetes, and increased BMI - collectively suggesting metabolic dysfunction worsens airway disease severity.
2. Obesity and Inhibition of Type 2 (T2) Inflammation
This is the most important and nuanced mechanism:
- Normally, the T2 immune response (via IL-33 → ILC2 → IL-5) promotes adipose eosinophilia and alternatively activated macrophages (AAMs), which maintain visceral adipose homeostasis through lipolysis, insulin sensitivity maintenance, and thermogenesis induction
- Obesity shifts adipose tissue macrophages from the alternatively activated (anti-inflammatory) phenotype to a classically activated macrophage phenotype, producing the chronic low-grade inflammation of metabolic syndrome
- IL-33 also impacts whole-body metabolism via non-shivering thermogenesis, pancreatic insulin production, and glucose clearance
- Key consequence: Drugs that inhibit T2 inflammation (inhaled/systemic corticosteroids, anti-T2 biologics) may worsen metabolic dysfunction and promote weight gain by removing the homeostatic role of T2 inflammation in adipose tissue - a critical bidirectional link
3. Non-T2 Mechanisms of Asthma in Obesity
Human studies show T2 biomarkers (blood eosinophils, FeNO) are no different or lower in obese asthma vs. non-obese asthma, indicating that non-T2 pathways are also important:
- Impaired airway host defense: Obesity and metabolic dysfunction increase susceptibility to severe respiratory viral illness (COVID-19, influenza)
- Cytotoxic T lymphocyte dysfunction: Natural killer cells and CD8+ T cells are impaired in obesity, reducing ability to eliminate virally infected cells
- Obese asthmatics show alterations in natural killer cell function and decreased airway gene expression of cytotoxic T lymphocyte signals
- This explains why obese adults with asthma who get a respiratory tract infection are nearly 3x more likely to require systemic corticosteroids than lean patients
4. Impact of Obesity on Pulmonary Mechanics
Figure: Lung Volumes - Lean vs. Obese
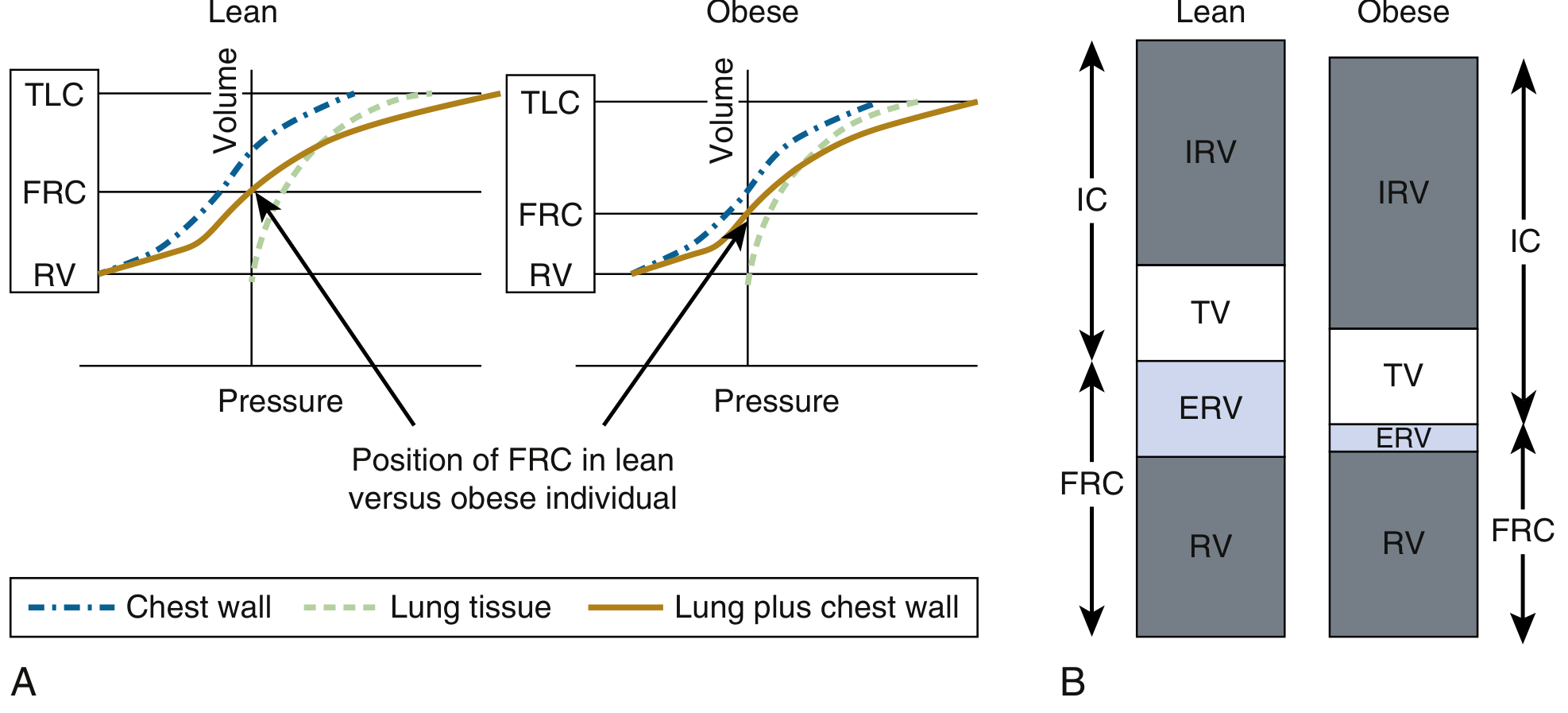
Figure 61.2 - Murray & Nadel's: In obesity, the chest wall is weighted with adipose tissue. This reduces the resting lung volume (FRC) and particularly decreases ERV (expiratory reserve volume).
Key mechanical effects:
- Reduced FRC (functional residual capacity) due to adipose loading of the chest wall
- Reduced ERV (expiratory reserve volume) - most prominently affected
- Dysanapsis: disproportionately small airways relative to lung parenchyma, increasing airway resistance
- Airways breathing near closing volume - intermittent airway closure leads to atelectasis, V/Q mismatch, and hypoxemia
- These changes are worse supine (positional worsening at night) and contribute to nocturnal symptoms
Spirometry pattern: Obese asthmatics often show a mixed obstructive-restrictive pattern, or simply a reduced FVC with preserved FEV1/FVC, complicating diagnosis.
Clinical Features
- Asthma in obese patients is more severe than in lean patients
- 2-4x increased risk of hospitalization for asthma exacerbations
- Higher risk of requiring mechanical ventilation or NIV during hospitalization
- Longer hospital stays
- Increased daytime and nocturnal symptoms
- Increased rescue SABA use
- Exacerbation triggers: viral URTI is more common - obese adults are more likely to develop influenza despite vaccination, and have worse outcomes
Factors contributing to increased severity (Table 61.1):
| Factor | Mechanism |
|---|---|
| Altered physiology | Reduced FRC, dysanapsis |
| Lower baseline lung function | Less pulmonary reserve during illness |
| Increased infection risk | Impaired cytotoxic T cell function |
| Impaired medication response | Reduced bronchodilator and ICS response |
| Comorbidities | GERD, OSA, depression, nasal polyposis |
Sex disparity: The association is more pronounced in women. Asthma rates in obese women are 14.6% vs. 7.9% in lean women. In men, the difference is less pronounced (7.1% obese vs. 6.1% lean).
Diagnostic Evaluation
Obesity complicates asthma diagnosis because:
- Dyspnea on exertion may be due to deconditioning, not asthma
- T2 biomarkers are unreliable in obesity:
- Blood eosinophils perform poorly as a biomarker of airway T2 inflammation in obese patients (circulating eosinophils may reflect metabolic changes)
- FeNO may be altered based on age of asthma onset in obesity
- Spirometry may show mixed pattern
- Objective bronchodilator reversibility testing is still necessary
Management
A. Standard Asthma Medications (with caveats)
Bronchodilators (SABA/LABA):
- Obese Black and Hispanic children are less likely to respond to bronchodilators
- Obese adults show smaller FEV1 improvements with SABAs than lean adults
- Response to LAMAs on lung function is similar in lean vs. obese, but effect on control and exacerbations is unreported
- Theophylline: paradoxically may increase exacerbations in obese patients - avoid
Inhaled Corticosteroids (ICS):
- Impaired response in obese older children and adults
- Reasons: altered ventilatory patterns affect drug deposition, pharmacokinetic changes, impaired induction of anti-inflammatory pathways
- Fewer obese patients have T2-high disease, so fewer respond to ICS
Systemic Corticosteroids: Should be avoided as much as possible - promote further weight gain and metabolic dysfunction
B. Anti-T2 Biologics
- Not directly assessed in RCTs for obese asthmatics specifically
- Caution: Anti-T2 biologics may worsen metabolic dysfunction and contribute to weight gain (by removing the homeostatic T2 effect on adipose tissue)
- T2 biomarkers are altered in obesity, making patient selection difficult
- Retrospective studies show variable response
C. Comorbidity Management (Table 61.2)
Treating comorbidities is particularly important in obese asthma:
| Comorbidity | Notes |
|---|---|
| Gastroesophageal reflux (GERD) | Common in obesity; treating is important even if evidence for direct asthma benefit is mixed |
| Obstructive sleep apnea (OSA) | Worsens nocturnal asthma; CPAP therapy |
| Depression | Higher prevalence in obese patients; associated with poor asthma control |
| Nasal polyposis | As seen in lean severe asthma |
D. Diet, Exercise, and Weight Loss
- Losing ≥5% of body weight is associated with measurable improvement in asthma control
- Exercise addition to weight loss programs provides additional benefit
- A structured weight loss program is more effective than simple advice
- Dietary quality improvement: reduce processed foods/sugars; increase fruit, fiber, vegetables - may reduce exacerbations and improve bronchodilator responsiveness independently of weight
E. Bariatric Surgery
- Indicated in morbidly obese patients who have not responded to nonsurgical approaches
- Retrospective evidence shows significant reduction in asthma exacerbations in the 2 years post-surgery vs. 2 years pre-surgery
- Laparoscopic approaches are well tolerated and minimize surgical risk
- Should only be considered after careful risk-benefit discussion
- Improves multiple obesity-related comorbidities concurrently
Summary: Key Points for Exam
- The obesity-asthma relationship is bidirectional - each is a risk factor for the other
- Pathophysiology involves: metabolic dysfunction (IL-6, insulin resistance), T2 inhibition paradox, non-T2 immune defects (cytotoxic T cell dysfunction), and mechanical effects (reduced FRC/ERV, dysanapsis)
- Obesity causes a T2-low asthma phenotype predominating - therefore ICS and anti-T2 biologics work less well
- T2 inhibition by medications promotes obesity - a critical bidirectional loop
- Clinical disease is more severe: 2-4x hospitalization risk, higher need for ventilatory support, increased viral exacerbations
- T2 biomarkers (eosinophils, FeNO) are unreliable in obese patients for guiding biologic therapy
- Theophylline is paradoxically harmful in obese asthma
- Weight loss ≥5% improves asthma control; bariatric surgery is effective in morbidly obese patients
- Comorbidity treatment (OSA, GERD, depression) is integral to management
Sources: Murray & Nadel's Textbook of Respiratory Medicine (Chapter 61: Asthma and Obesity), Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.