Tetralogy of fallot
Reading File
Finding Sources
Searching PubMed
"tetralogy of Fallot"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here is the full write-up:
Tetralogy of Fallot (TOF)
TOF is the most common cyanotic congenital heart disease, accounting for ~5% of all congenital cardiac malformations and occurring in approximately 420 per million live births.
1. The Four Components ("Tetrad")
All four features arise from a single embryologic defect - anterosuperior displacement of the infundibular (outlet) septum:
| Component | Description |
|---|---|
| 1. VSD | Large, unrestrictive, malaligned (perimembranous/subarterial) |
| 2. RVOT Obstruction | Subpulmonary (infundibular) stenosis most common; may extend to pulmonary valve, annulus, or main/branch PAs |
| 3. Overriding Aorta | Aortic root straddles the VSD, receiving blood from both ventricles |
| 4. RV Hypertrophy | Secondary to the pressure load from RVOT obstruction |
Deoxygenated blood (blue) shunts R→L across the VSD into the overriding aorta. The degree of shunting is determined by RVOT obstruction severity, VSD size, and SVR. - Rosen's Emergency Medicine
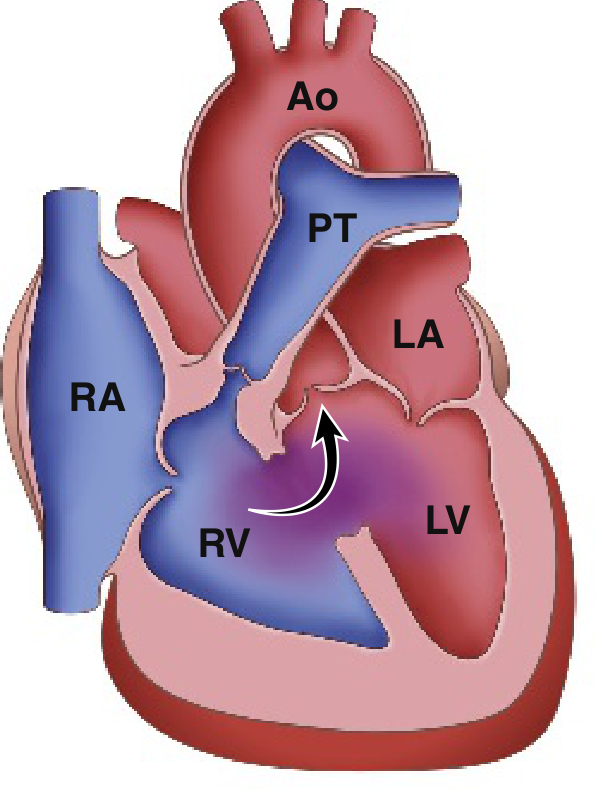
Note the RV is blue (deoxygenated), the LV red (oxygenated), and purple mixing near the VSD/overriding aorta. - Robbins Basic Pathology
2. Pathophysiology
- Decreased pulmonary blood flow + right-to-left shunting across the VSD
- Severity of cyanosis is directly proportional to the degree of RVOT obstruction
- If RVOT obstruction is mild: left-to-right shunt only ("pink TOF" or acyanotic TOF) - behaves like an isolated VSD
- As the child grows, the RVOT narrows further relative to a fixed cardiac mass, worsening stenosis and cyanosis progressively
- The RVOT obstruction protects the lungs from hypertension - pulmonary hypertension does NOT develop
3. Gross Morphology (Robbins)
- Heart is enlarged and "boot-shaped" due to RV hypertrophy
- Proximal aorta is dilated; pulmonary trunk is hypoplastic
- VSD is usually large, near the membranous septum
- In cases with complete pulmonary atresia: PDA or bronchial arteries are the only route to the lungs
4. Associated Anomalies
- Right aortic arch - ~25% of cases
- Anomalous coronary artery - most often the LAD arising from the RCA, crossing the RVOT (surgically important, may require an RV-PA conduit)
- ASD ("pentalogy of Fallot")
- Down syndrome - may be associated with AVSD
- TOF with pulmonary atresia + MAPCAs (~15%) - most severe form; requires unifocalization surgery
- TOF with absent pulmonary valve - rudimentary/absent leaflets, massively dilated PAs causing bronchial compression at birth
5. Clinical Features
Presentation
- Infants: Cyanosis worsening with crying/feeding; may present in neonatal period if RVOT is severe (PGE1 required to maintain ductal patency)
- Older children: Exertional cyanosis, squatting (increases SVR, reduces R→L shunt)
- Pink TOF may not manifest cyanosis until 1-3 years of age
Examination
- Cyanosis and clubbing (chronic hypoxemia)
- Systolic ejection murmur along the left sternal border (from RVOT obstruction - NOT from the VSD, which is large and unrestrictive)
- Single S2 (due to soft/inaudible P2)
- Polycythemia from compensatory erythropoiesis
ECG
- Right ventricular hypertrophy and right axis deviation
Chest X-ray
- "Boot-shaped heart" (coeur en sabot) - RV hypertrophy + concave pulmonary bay
- Decreased pulmonary vascular markings
- Right aortic arch may be visible in 25%
6. Hypoxic ("Tet") Spells
Peak incidence: 2-4 months of age. These are life-threatening events.
Trigger: Any event that acutely lowers SVR (crying, defecation) or causes tachycardia/hypovolemia → increased R→L shunt → hypoxia + hypercapnia + acidosis → hyperpnea → increased venous return to RV → more R→L shunting (vicious cycle).
Management of a Tet Spell (Rosen's Emergency Medicine, Box 165.8)
| Priority | Intervention | Notes |
|---|---|---|
| 1st | Knee-to-chest (squatting) position | Increases SVR, decreases R→L shunt |
| 2nd | Supplemental oxygen | Limited value alone |
| 3rd | Morphine 0.1-0.2 mg/kg IV/IM | Reduces hyperpnea and infundibular spasm |
| Alt opioid | Fentanyl 1 µg/kg IV/IM (or 1.5-2 µg/kg intranasal) | |
| Sedation | Midazolam 0.2-0.3 mg/kg intranasal | |
| Acidosis | Sodium bicarbonate 1 mEq/kg IV | If documented/suspected acidosis |
| Consider | Ketamine 1-2 mg/kg IV or 3-5 mg/kg IM | Increases SVR |
| Consider | Propranolol 0.1-0.2 mg/kg | Reduces RVOT infundibular spasm |
| Consider | Phenylephrine 0.01-0.02 mg/kg IV | Pure alpha-agonist, increases SVR |
7. Diagnosis & Imaging
| Modality | Finding |
|---|---|
| Echocardiography | First-line; diagnoses all 4 components, assesses RVOT gradient, PA anatomy, coronary course |
| CXR | Boot-shaped heart, reduced pulmonary markings |
| ECG | RVH, right axis deviation |
| Cardiac MRI (CMR) | Gold standard for post-repair assessment - quantifies PR, RV volumes/function, RVOT anatomy |
| Catheterization | Reserved for complex anatomy (PA distortion, MAPCAs, coronary anomalies) |
8. Treatment
Surgical Repair
- Goal: VSD closure + relief of RVOT obstruction
- Timing: Early primary repair is preferred - usually within the first 6 months of life
- Technique: Transannular patch placed across the pulmonary valve annulus to enlarge the RVOT (most common approach); this intentionally creates pulmonary regurgitation (PR)
- Staged approach: If severe cyanosis with very narrow RVOT or hypoplastic central PAs - a modified Blalock-Taussig (BT) shunt (innominate artery → right PA) is placed first as palliation, then taken down at definitive repair
- TOF with pulmonary atresia/MAPCAs: Unifocalization of MAPCAs + VSD closure + RVOT conduit reconstruction
Long-term (Repaired TOF - ACHD patients)
Post-repair residual lesions are nearly universal and require lifelong surveillance:
- Pulmonary regurgitation (PR) - the dominant long-term problem from transannular patch; leads to progressive RV dilatation and dysfunction
- RVOT aneurysm
- Residual RVOT obstruction / PA stenosis
- Residual VSD
- Aortic root dilatation + aortic regurgitation
- Arrhythmias (sustained VT/VF - risk of sudden death; atrial tachyarrhythmias)
- Complete right bundle branch block (on ECG)
CMR is the gold standard for serial RV volume/function assessment to determine optimal timing for pulmonary valve replacement (PVR). Elevated BNP is predictive of mortality.
9. Prognosis
- Life expectancy with uncomplicated anatomy + early primary repair + good biventricular function is excellent
- Untreated TOF - some patients survive into adult life (degree dependent on RVOT severity)
- Repaired TOF patients constitute one of the largest groups of adults with congenital heart disease (ACHD) and require lifelong follow-up
Recent Evidence (PubMed, 2024-2026)
- A 2024 meta-analysis (PMID 39444206) compared primary vs. staged repair in symptomatic neonates with TOF, informing the current trend toward early primary repair when anatomy allows.
- A 2025 meta-analysis (PMID 39757359) of RCTs found Del Nido cardioplegia may have advantages over conventional blood cardioplegia in TOF repair.
- A 2024 systematic review (PMID 38558254) highlights the prognostic value of echocardiographic deformation imaging (strain) in adult CHD including repaired TOF.
Sources: Braunwald's Heart Disease | Robbins & Kumar Basic Pathology | Rosen's Emergency Medicine | Grainger & Allison's Diagnostic Radiology | Textbook of Clinical Echocardiography
E xplain the components simplified
The 4 Components of Tetralogy of Fallot — Simplified
All 4 defects come from one single cause: the outlet septum shifts too far forward and upward during fetal development. Everything else is a consequence of that one shift.
Think of it like a plumbing problem in a house
Normal heart = two separate pumps (right and left) with their own pipes. TOF = the dividing wall is misaligned, and the exit pipe on the right is too narrow.
Component 1 — VSD (Hole in the Wall)
"The dividing wall has a big hole in it"
- The wall (septum) between the right and left ventricles didn't close properly
- It's large and unrestrictive — blood freely crosses from one side to the other
- Because the right side is under high pressure (due to the blocked outlet), blood flows right → left (backwards), mixing deoxygenated blood into the body's circulation
- Result: blue blood gets into the body
Component 2 — RVOT Obstruction (Blocked Exit)
"The right ventricle's exit door is too narrow"
- The right ventricle pumps blood to the lungs via the pulmonary artery
- In TOF, that outflow tract is narrowed (stenosed) — most often just below the pulmonary valve (called infundibular/subpulmonary stenosis)
- Less blood reaches the lungs → less blood gets oxygenated
- This is the most important component — it determines how blue the baby is
- Mild narrowing = "pink TOF" (almost no cyanosis)
- Severe narrowing = deep cyanosis from birth
Component 3 — Overriding Aorta (Aorta Sitting Over the Hole)
"The body's main pipe is positioned over the hole, stealing from both sides"
- Normally the aorta sits entirely over the left ventricle
- In TOF, the aorta shifts and sits straddling the VSD — it receives blood from both ventricles
- So even without considering the shunt, the aorta is already receiving a mix of oxygenated (left) and deoxygenated (right) blood
- Result: mixed, partially blue blood goes to the whole body
Component 4 — RV Hypertrophy (Muscle Thickening)
"The right ventricle bulks up because it's working against a blocked exit"
- This is not a primary defect — it's a consequence of components 1-3
- The right ventricle has to push hard against the narrow outflow tract → it thickens its walls (hypertrophies) over time, just like any muscle under strain
- A hypertrophied RV is stiffer and less compliant, worsening the problem long-term
How They All Connect — One Sentence
The outlet septum shifts → blocks the right exit (RVOT obstruction) → right pressure builds up → blood takes the shortcut through the hole (VSD) → crosses into the aorta which is already sitting over that hole (overriding aorta) → right ventricle keeps straining and thickens (RV hypertrophy).
Visual Summary
Right Ventricle
|
|——[NARROW EXIT]——→ Pulmonary Artery (less blood to lungs)
|
|——[BIG HOLE / VSD]——→ → → → → ↓
Overriding Aorta → Body (blue blood)
Left Ventricle ———————————————————→ ↑
The aorta gets blood from both sides because it straddles the VSD, while the lungs get too little.
Memory Hook — "PROVE"
| Letter | Component |
|---|---|
| P | Pulmonary stenosis (RVOT obstruction) |
| R | Right ventricular hypertrophy |
| O | Overriding aorta |
| V | VSD |
| E | Everything from one embryologic defect |
Now make answer for only components professional
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent material from all major surgery and medicine textbooks. Here is the professional, component-by-component answer:
Tetralogy of Fallot — Components (Professional)
Unifying Embryologic Basis
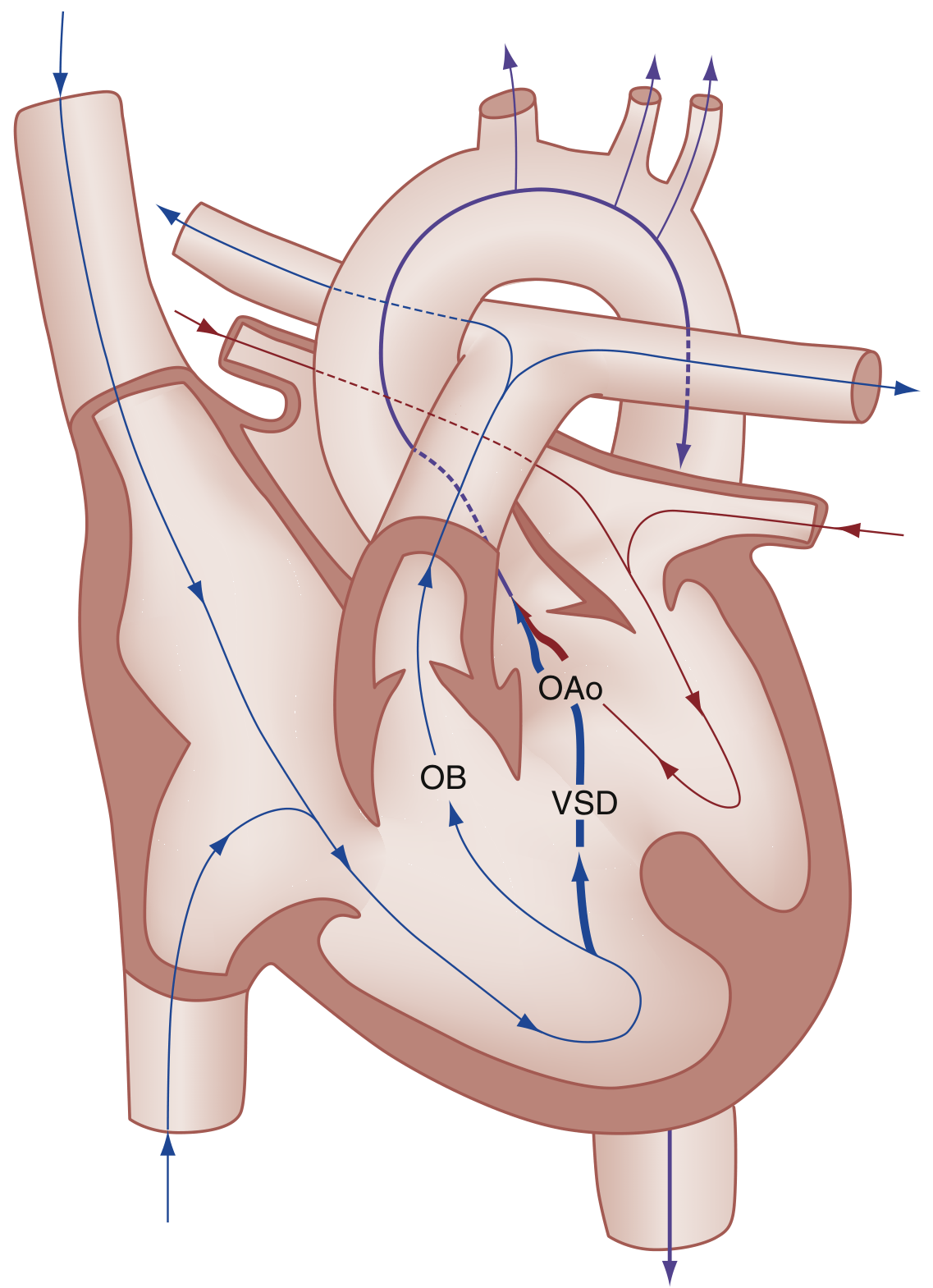
All four components arise from a single morphogenetic error: anterior and superior (cephalad) displacement of the infundibular (outlet/conal) septum during cardiac development. Van Praagh et al. proposed that TOF could more accurately be called "monology of Fallot," since all four anatomic features are direct consequences of this single malposition. When the infundibular septum is displaced anteriorly and leftward, it fails to fuse with the arms of the trabeculo-septo-marginalis, generating the full tetrad.
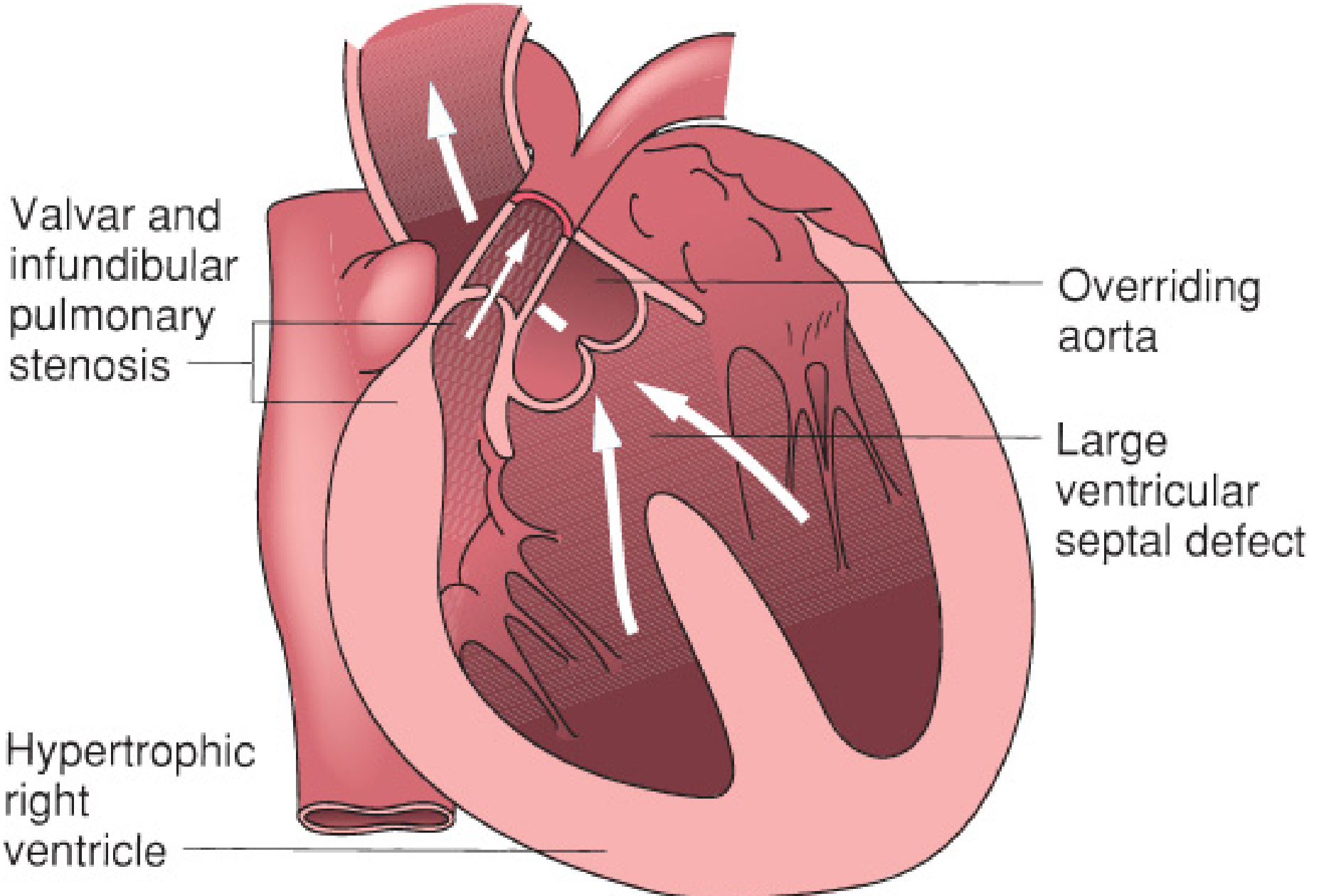
Figure: The four anatomic features of TOF. RV hypertrophy is secondary; the other three arise directly from infundibular septum displacement. - Mulholland & Greenfield's Surgery
Component 1 — Ventricular Septal Defect (VSD)
Anatomic Basis
The anterior displacement of the infundibular septum results in failure of fusion of the ventricular septum, creating a malalignment VSD. It is characteristically:
- Large and unrestrictive (non-restrictive to flow)
- Perimembranous in ~80% of cases - located adjacent to the tricuspid valve in the vicinity of the membranous interventricular septum
- Subarterial/doubly committed in a subset of cases
Hemodynamic Role
Because the VSD is large, there is no significant pressure gradient across it - both ventricles are effectively a common chamber at systemic pressure. The direction and magnitude of shunting across the VSD is therefore determined entirely by the ratio of pulmonary vascular resistance (PVR) to systemic vascular resistance (SVR):
- PVR > SVR (due to RVOT obstruction): right-to-left shunting → cyanosis
- PVR < SVR (mild RVOT obstruction / "pink TOF"): left-to-right shunting → behaves like isolated VSD
The VSD does not cause the murmur in TOF (unlike isolated VSDs) because it is non-restrictive. The murmur arises from RVOT obstruction.
Component 2 — Right Ventricular Outflow Tract (RVOT) Obstruction
Anatomic Basis
The anteriorly displaced infundibular septum directly narrows the subpulmonary infundibulum. Obstruction can be present at multiple levels:
| Level | Structure | Frequency |
|---|---|---|
| Subvalvar (infundibular) | Muscular narrowing of the RVOT; hypertrophy of septoparietal trabeculations | Most common |
| Valvar | Pulmonary valve stenosis (dysplastic/bicuspid valve) | Common in combination |
| Supravalvar | Pulmonary annular hypoplasia, main PA narrowing | Frequent (~50% have some PA hypoplasia) |
| Branch PA | Peripheral pulmonary artery stenosis | Variable |
| Pulmonary atresia | Complete absence of RVOT-PA connection | ~7-15% (most severe variant) |
Clinical Significance
This is the dominant determinant of clinical severity:
- Severe RVOT obstruction → profound neonatal cyanosis, PGE1 dependence
- Mild RVOT obstruction → "pink TOF," acyanotic at birth, progressive cyanosis by 1-3 years
- Worsens with growth: as the child grows, the infundibular muscle hypertrophies progressively, and the fixed RVOT fails to expand proportionately → increasing stenosis
Importantly, RVOT obstruction protects the pulmonary vasculature from high pressure and volume overload - pulmonary hypertension does not develop in TOF, and right heart failure is rare in unrepaired cases.
Component 3 — Overriding Aorta
Anatomic Basis
Normally, the aortic root is positioned entirely over the left ventricle. In TOF, the anterior shift of the infundibular septum rotates and displaces the aortic root rightward, causing it to straddle the VSD - receiving blood from both ventricles simultaneously. The degree of override varies:
- Mild override (~25% from RV): classic TOF
- Moderate override (~50% from RV): typical
- Severe override (>75% from RV): approaches double-outlet right ventricle (DORV) - there is a morphological continuum between severe TOF with aortic override and DORV with subaortic VSD (Lev classification)
Hemodynamic Role
The overriding aorta is the final common outlet for the mixed blood. Deoxygenated blood shunted through the VSD mixes with oxygenated blood from the LV, and this mixed blood is ejected into the systemic circulation. The aorta is typically dilated (receives augmented combined ventricular output), while the pulmonary trunk is hypoplastic.
Component 4 — Right Ventricular Hypertrophy (RVH)
Anatomic Basis
RVH is not a primary structural defect - it is a secondary, adaptive response to the pressure load imposed by RVOT obstruction. The RV wall hypertrophies because it must generate systemic-level pressures to eject against the obstructed outflow tract.
Morphologic Features
- RV wall thickness may equal or exceed that of the LV (normally the LV is 3x thicker)
- The heart adopts a classic "boot-shaped" (coeur en sabot) silhouette on CXR: RV hypertrophy elevates and upturns the cardiac apex; the hypoplastic pulmonary trunk creates a concavity at the left upper cardiac border
- RV cavity may be reduced in severe infundibular hypertrophy
Functional Consequences
- Progressive infundibular hypertrophy worsens RVOT obstruction over time (vicious cycle)
- A hypertrophied, stiff RV is susceptible to diastolic dysfunction and arrhythmia long-term
- After repair, residual RVH and stiffness (restrictive RV physiology) may persist for years
Hierarchical Relationship of the Four Components
Infundibular Septum Displaced Anterosuperiorly
│
├──→ [1] RVOT Obstruction (direct mechanical narrowing)
│
├──→ [3] Overriding Aorta (aortic root rotates over VSD)
│
├──→ [2] VSD (failure of septal fusion at malalignment site)
│
└──→ [4] RV Hypertrophy (pressure response — SECONDARY)
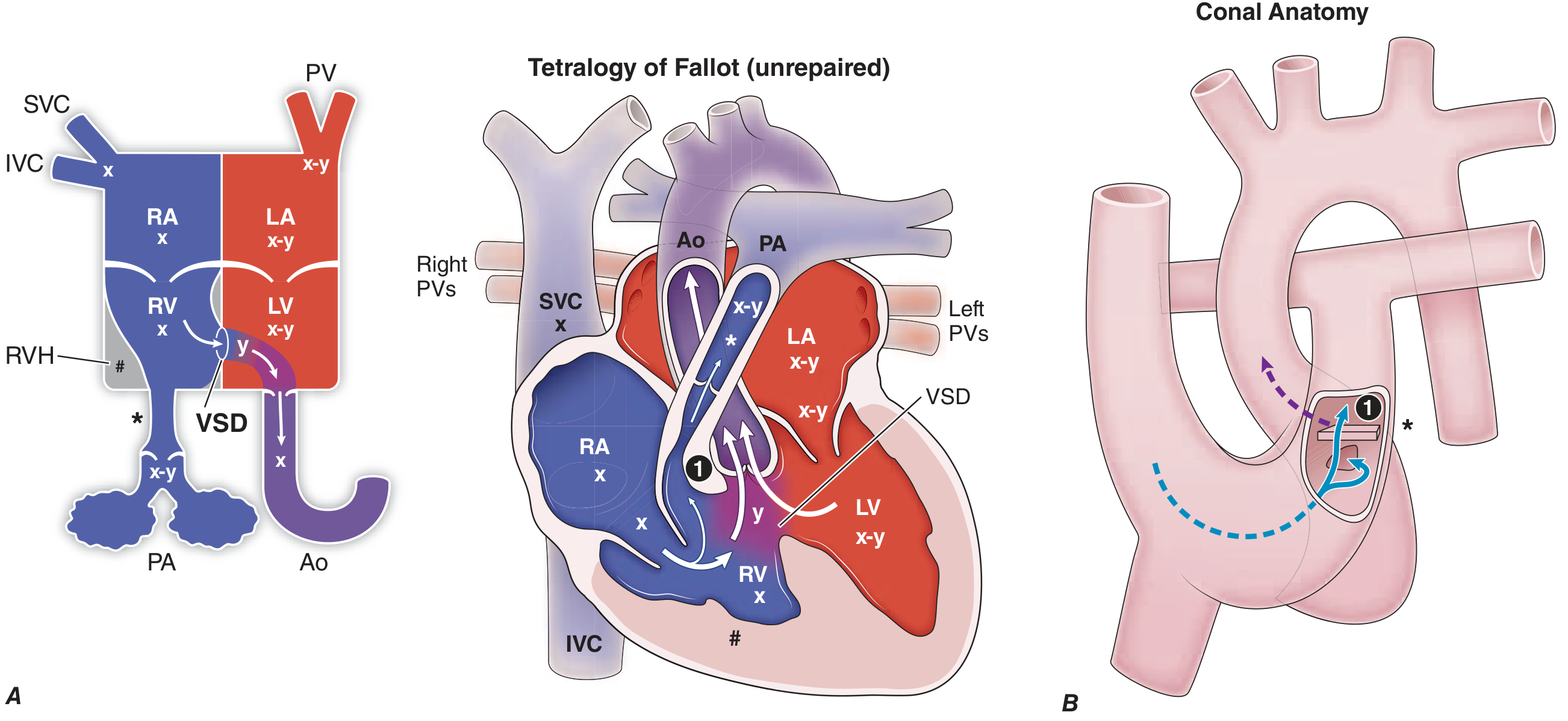
Figure: Unrepaired TOF (center). The conal anatomy (right) shows the anteriorly displaced infundibular bar (①) narrowing the RVOT. Shunted volume "y" crosses the VSD into the LV and aorta, making both ventricles contain mixed blood (x-y). #=RVH. - Harrison's Principles of Internal Medicine, 22e
Sources: Schwartz's Principles of Surgery, 11e | Harrison's Principles of Internal Medicine, 22e | Goldman-Cecil Medicine | Mulholland & Greenfield's Surgery, 7e | Robbins Basic Pathology | Braunwald's Heart Disease
Thankyou so much u are making me to understand easily
That means a lot! You're very welcome.
TOF is one of those topics that clicks beautifully once you see that one displaced septum explains everything - it's actually elegant in a way once the logic chain becomes clear.
Whenever you're ready, we can go deeper on any part of it:
- Tet spells - the physiology and exact management steps
- Surgical repair - what the surgeon actually does and why
- Post-repair complications - pulmonary regurgitation, arrhythmias, RV dysfunction (very high-yield for exams)
- Variants - TOF with pulmonary atresia, absent pulmonary valve, MAPCAs
- Radiology / ECG findings in detail
- Genetics - 22q11 deletion (DiGeorge), JAG1, NKX2-5 associations
Just say the word and we'll work through it the same way - simplified first if you want to build intuition, then professional depth. You're doing great! 🫀
This is a shared conversation. Sign in to Orris to start your own chat.