Acute and chronic pharyngitis. Classification. Etiology. pathogenesis, symptoms, diagnostics, differential oropharyngeal diagnosis between hypertrophic, granular, atrophic. Their treatment, complications, prevention
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive review of acute and chronic pharyngitis integrating content from Cummings Otolaryngology, Goldman-Cecil Medicine, and other authoritative sources.
Pharyngitis: Acute and Chronic
1. Definition and Classification
Pharyngitis is inflammation of the mucosa and underlying structures of the pharynx. It is broadly classified by:
By Duration:
- Acute pharyngitis — onset over hours to days; resolves within 3–7 days (infectious majority)
- Chronic pharyngitis — persistent or recurrent inflammation lasting weeks to months; often non-infectious in etiology
Chronic pharyngitis is further classified morphologically into three forms:
| Form | Key Feature |
|---|---|
| Hypertrophic (granular) | Lymphoid hyperplasia; granular cobblestone posterior wall |
| Atrophic (sicca) | Mucosal thinning, dryness, crusting; glandular atrophy |
| Simple (catarrhal) | Mild persistent mucosal congestion without structural change |
(Some classifications treat hypertrophic and granular as synonyms; others distinguish a lateral hypertrophic variant — hyperplasia of lateral bands — as a separate subtype.)
2. Etiology
Acute Pharyngitis
Viral (majority — ~70–90% of acute cases):
- Rhinovirus, influenza A/B, parainfluenza, adenovirus, coxsackievirus (herpangina, hand-foot-and-mouth), echovirus, RSV
- Epstein-Barr virus (EBV) — infectious mononucleosis
- Herpes simplex virus (HSV) — exudative or non-exudative pharyngitis
- HIV (acute retroviral syndrome)
- Rarely: CMV, measles, rubella
Bacterial (10–30% of cases; more common in children):
- Streptococcus pyogenes (Group A β-hemolytic Streptococcus, GAS) — most important bacterial cause (20–40% of pediatric cases; 5–15% of adult cases)
- Non-group A β-hemolytic streptococci (Groups B, C, G)
- Neisseria gonorrhoeae — sexually transmitted; often overlooked
- Corynebacterium diphtheriae — membranous pharyngitis; rare in vaccinated populations
- Arcanobacterium haemolyticum — resembles streptococcal pharyngitis with rash in young adults
- Fusobacterium necrophorum — Lemierre syndrome risk
- Mycoplasma pneumoniae, Chlamydophila pneumoniae — atypical organisms
Other:
- Fungal (Candida albicans) — immunosuppressed patients
- Parasitic (rare)
Chronic Pharyngitis
- Persistent low-grade infection or recurrent acute episodes
- Laryngopharyngeal reflux (LPR) — a leading non-infectious cause
- Tobacco smoke, alcohol, dry air, occupational irritants, dust
- Chronic mouth breathing (nasal obstruction, deviated septum, adenoid hypertrophy)
- Chronic sinusitis with postnasal drip
- Allergy / vasomotor rhinitis
- Systemic diseases: Sjögren syndrome, sarcoidosis, amyloidosis, pemphigus
- Vitamin A deficiency (contributes to atrophic changes)
3. Pathogenesis
Acute
- Viral: Direct cytopathic effect on pharyngeal epithelium → mucosal edema, erythema, cellular infiltrate. Many viral infections are transmitted droplet or contact route.
- GAS (Streptococcal): S. pyogenes adheres to pharyngeal epithelium via M protein and other surface adhesins → local invasion → release of streptolysin O, streptolysin S, pyrogenic exotoxins (causing scarlet fever rash), DNase, hyaluronidase → intense local inflammatory response → fever, exudate, lymphadenopathy.
- Pharyngitis induces antibodies against M protein, streptolysin O, DNase, hyaluronidase, and pyrogenic exotoxins.
- Non-treated infection may spread suppuratively or trigger immune-mediated sequelae (rheumatic fever, glomerulonephritis).
Chronic
- Repeated acute insults → chronic mucosal edema → lymphoid hyperplasia (hypertrophic/granular form)
- Prolonged irritation (smoke, reflux, dry air) → progressive glandular atrophy, mucosal thinning, decreased mucus secretion → atrophic form
- LPR: Acid and pepsin reach the posterior pharynx → posterior laryngitis, interarytenoid edema, erythematous arytenoids, reactive changes
4. Clinical Symptoms
Acute Pharyngitis
| Feature | Viral | GAS Bacterial |
|---|---|---|
| Onset | Gradual | Abrupt |
| Sore throat severity | Mild–moderate | Moderate–severe |
| Fever | Low-grade or absent | High (38.5–40°C) |
| Cough/rhinorrhea | Common | Absent (key negative predictor) |
| Hoarseness | Sometimes | Rare |
| Headache | Occasional | Common |
| Malaise | Common | Common |
| Nausea/vomiting | Rare | Common (children) |
Additional presentations:
- EBV mononucleosis: fever, severe malaise, pharyngitis, cervical lymphadenopathy (large and tender), splenomegaly, palatal petechiae, occasional green/gray tonsillar exudate (indistinguishable from GAS)
- Herpangina (Coxsackievirus): vesicles → ulcers on anterior tonsillar pillars, soft palate, posterior pharynx
- Influenza: abrupt fever, headache, myalgias, sore throat, mild pharyngeal hyperemia without exudate
- HIV acute retroviral: fever, diffuse lymphadenopathy, maculopapular rash, pharyngitis (often with ulcerations)
Chronic Pharyngitis
All forms share:
- Persistent throat discomfort, tickling, irritation, or dryness
- Chronic throat-clearing
- Low-grade dysphagia
- Postnasal drip sensation ("globus")
5. Physical Examination & Diagnostics
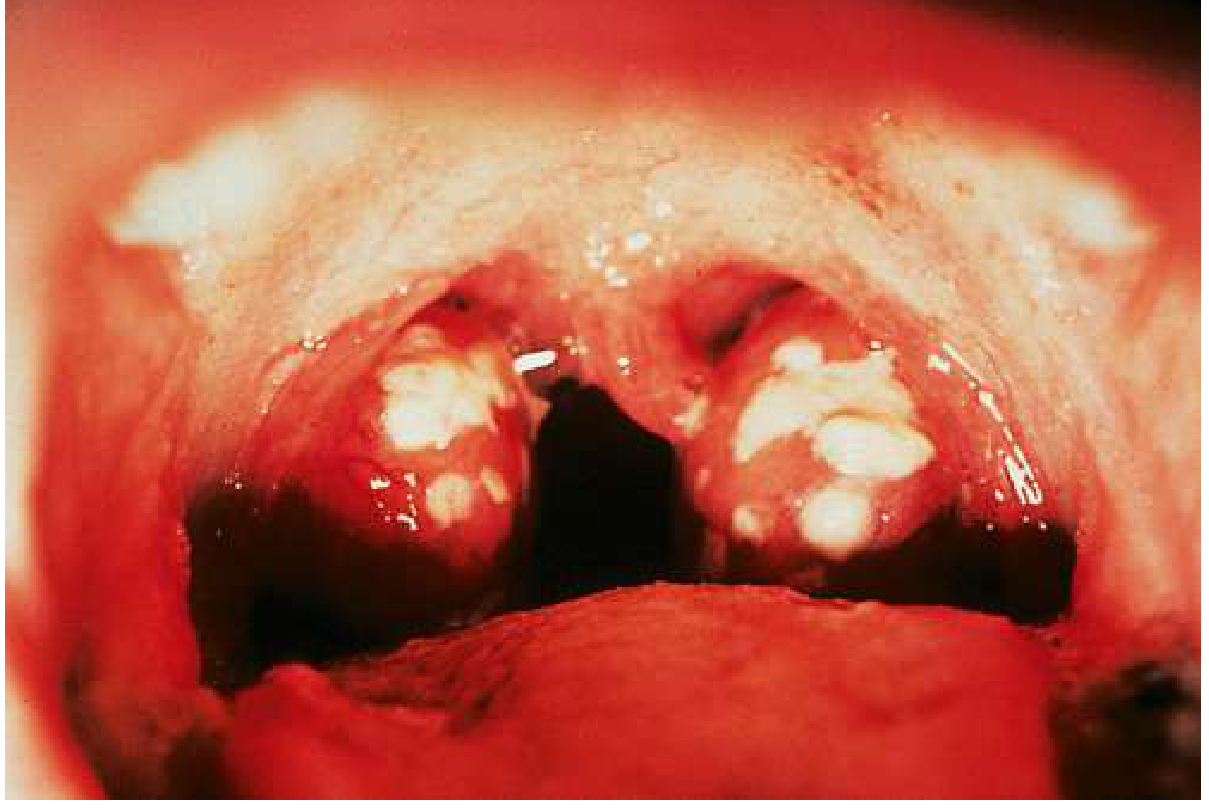
Acute Pharyngitis — Oropharyngeal Findings
Clinical scoring — Modified Centor Score (McIsaac Score):
| Criterion | Points |
|---|---|
| Temperature > 38°C | +1 |
| Absence of cough | +1 |
| Tender anterior cervical adenopathy | +1 |
| Tonsillar swelling or exudate | +1 |
| Age 3–14 years | +1 |
| Age ≥ 45 years | −1 |
- Score 0–1: No testing or antibiotics needed
- Score 2–3: Rapid antigen test recommended
- Score ≥ 4: Empiric antibiotics reasonable; culture if rapid test negative
Laboratory diagnostics:
- Rapid antigen detection test (RADT): Sensitivity ~85%; specificity high. If negative in children/adolescents → send throat culture.
- Rapid nucleic acid test (NAAT): Sensitivity 97.5%, specificity 95% — preferred.
- Throat culture: Gold standard. Posterior pharynx/tonsillar surface swab. Treat if positive; no need to culture adults with negative rapid test (low GAS prevalence, low rheumatic fever risk).
- Monospot/heterophile antibody test: EBV mononucleosis screening
- CBC: Atypical lymphocytosis in EBV; leukocytosis in bacterial infection
- ASO titer, anti-DNase B: Retrospective confirmation of GAS infection (used for rheumatic fever / glomerulonephritis workup)
6. Differential Diagnosis: Chronic Pharyngitis Forms
This is the core morphological/clinical distinction:
| Feature | Hypertrophic (Granular) | Atrophic (Sicca) |
|---|---|---|
| Pathology | Lymphoid follicle hyperplasia; submucosal edema; mucus gland hypertrophy | Mucosal thinning; glandular atrophy; submucosal fibrosis; reduced mucus secretion |
| Pharyngeal wall appearance | Cobblestone / granular posterior wall; irregular nodules of lymphoid tissue; hyperemic, thickened mucosa; increased mucus secretion (may be thick, sticky) | Pale, dry, thin, shiny mucosa; may have dry crusts or adherent mucus; vascular pattern visible through atrophic mucosa |
| Tonsils / lateral bands | Enlarged; lateral bands may be thickened (lateral hypertrophic variant) | Absent or regressed; mucosa may bridge former tonsillar fossa |
| Secretions | Excessive, thick, sticky mucus — causes hawking/throat-clearing | Scanty, viscous; dry crusts (especially posterior wall); patients complain of "sticky throat" |
| Symptoms | Sensation of something in throat (globus), hawking, postnasal drip, cough reflex, mild sore throat | Burning, dryness, scratching sensation, halitosis from crusts, dysphagia |
| Associated conditions | Chronic sinusitis, adenoid hypertrophy, chronic mouth-breathing, GER, tobacco | Sjögren syndrome, advancing age, heavy smoking (paradoxically), vitamin deficiency, post-radiation, prolonged mouth-breathing in dry climates |
| Etiology emphasis | Repeated infections, LPR, allergic/chronic mucosal irritation | Long-standing irritation, autoimmune glandular destruction, post-atrophic rhinitis |
Key differentiator: The posterior pharyngeal wall appearance is the cornerstone — cobblestone granularity (hypertrophic) vs. pale, dry, smooth atrophic mucosa.
7. Treatment
Acute Pharyngitis
Viral:
- Supportive: analgesics (NSAIDs, acetaminophen), adequate hydration, throat lozenges, warm saline gargles
- Influenza: Neuraminidase inhibitors (oseltamivir 75 mg bid × 5 days, zanamivir) — effective only if started within 48 hours; reduces duration by 1–2.5 days; recommended in high-risk groups
- EBV mononucleosis: Supportive; avoid contact sports (splenomegaly/rupture risk); avoid amoxicillin/ampicillin (causes widespread maculopapular rash in ~90% of EBV patients); corticosteroids for severe airway edema or thrombocytopenia
- HSV: Acyclovir — especially in immunosuppressed patients with chronic herpetic pharyngitis
GAS Bacterial Pharyngitis:
First-line:
- Penicillin V 250 mg × 4/day or 500 mg × 2/day × 10 days (antibiotic of choice)
- Amoxicillin 500 mg × 3/day or 875 mg × 2/day × 10 days (often preferred in children — pleasant taste, once-daily dosing studied)
Penicillin-allergic:
- Azithromycin 500 mg/day × 3 days (Z-pack) — note increasing macrolide resistance
- Clindamycin 300 mg × 4/day × 10 days
Recurrent infection (β-lactamase-producing co-pathogens):
- Amoxicillin-clavulanate 875/125 mg × 2/day × 10 days
- Cefuroxime axetil 250 mg × 2/day × 10 days — more effective than penicillin for primary treatment; effective for persistent infection
Adjunct:
- Single-dose oral or IM corticosteroid (dexamethasone 10 mg PO/IM × 1) reduces severity and duration of pain — particularly in severe cases and children
- Antibiotics reduce contagion period from ~2 weeks to 24 hours after initiation
- Must begin antibiotics within 10 days of symptom onset to prevent rheumatic fever
- Antibiotics do NOT reduce risk of post-streptococcal glomerulonephritis
Gonococcal pharyngitis:
- Ceftriaxone 500 mg IM single dose (+ treat for Chlamydia if not tested)
Candidal pharyngitis:
- Fluconazole or nystatin suspension
Chronic Pharyngitis — General Principles
- Eliminate causative factors: smoking cessation, alcohol reduction, humidification, treat nasal obstruction, sinusitis, adenoids
- Treat LPR: dietary modification, elevate head of bed, proton pump inhibitor × 3 months
- Treat allergic disease: antihistamines, intranasal corticosteroids
Chronic Hypertrophic (Granular) Pharyngitis
- Address underlying causes (reflux, allergy, chronic infection)
- Alkaline or saline irrigations/gargles (reduce crusts, thin secretions)
- Topical anti-inflammatory sprays
- Cauterization or laser ablation of discrete granular nodules (in refractory cases)
- Immunotherapy for allergic component
Chronic Atrophic Pharyngitis
- Mucosal hydration: frequent water intake, saline irrigations, humidification
- Vitamin A supplementation (addresses glandular atrophy in deficiency states)
- Alkaline-oil inhalations (olive oil, mineral oil aerosols — lubricate mucosa)
- Treat underlying systemic disease (Sjögren: artificial saliva, pilocarpine; sarcoid: corticosteroids)
- Biostimulants (FIBS, aloe vera — used in Eastern European protocols)
- Avoid further irritants absolutely
8. Complications
Acute Pharyngitis (especially GAS)
Suppurative complications:
- Peritonsillar abscess (quinsy) — most common local complication; unilateral uvular deviation, "hot potato" voice, trismus
- Retropharyngeal/parapharyngeal abscess — neck stiffness, drooling, airway risk
- Otitis media — spread via Eustachian tube
- Sinusitis — contiguous spread
- Mastoiditis, meningitis, brain abscess (rare)
- Lemierre syndrome (Fusobacterium): septic thrombophlebitis of internal jugular vein
- Bacteremia / septicemia
- Scarlet fever (GAS pyrogenic exotoxin): characteristic rash, strawberry tongue, perioral pallor
- Streptococcal toxic shock syndrome (uncommon)
Non-suppurative (immunological) complications — GAS only:
- Acute Rheumatic Fever (ARF): 2–4 weeks post-pharyngitis; carditis, migratory polyarthritis, Sydenham chorea, erythema marginatum, subcutaneous nodules — prevented by antibiotics within 10 days
- Post-streptococcal glomerulonephritis (PSGN): 1–3 weeks post-pharyngitis; hematuria, proteinuria, edema, hypertension — NOT prevented by antibiotics
EBV Mononucleosis:
- Splenic rupture (avoid contact sports for 3–4 weeks)
- Airway obstruction from massive tonsillar enlargement
- Hemolytic anemia, thrombocytopenia
- Meningoencephalitis (rare)
- Amoxicillin/ampicillin rash
Chronic Pharyngitis:
- Chronic cough, recurrent upper respiratory infections
- Progression to laryngitis, chronic laryngopharyngeal reflux disease
- Sleep-disordered breathing
- Risk marker for malignancy (persistent symptoms warrant laryngoscopy if >4 weeks duration without resolution)
9. Prevention
Acute (especially GAS):
- Hand hygiene — primary prevention of spread
- Avoid sharing utensils, glasses
- Respiratory droplet precautions
- Prompt antibiotic treatment shortens infectious period to 24 hours post-initiation
- Influenza vaccination annually — at least 70% effective; recommended for age >50, children 6–24 months, pregnant women, healthcare workers, immunocompromised, residents of long-term care facilities
- Hib vaccine — prevents epiglottitis (not pharyngitis per se, but related)
- Tonsillectomy — reduces frequency of throat infections in patients with recurrent symptomatic GAS episodes despite appropriate antimicrobial therapy (effective short-term)
Chronic:
- Smoking cessation
- Nasal breathing — treat all causes of obstruction
- Adequate indoor humidification (especially in dry/cold climates)
- Treat GERD/LPR proactively
- Occupational protection from dust and chemical irritants
- Avoid excessive voice strain
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Chapters 201 and the pharyngitis/laryngitis review chapter)
- Goldman-Cecil Medicine, International Edition (Chapters 269 and 397)
- Tintinalli's Emergency Medicine; ROSEN's Emergency Medicine; Sherris & Ryan's Medical Microbiology
This is a shared conversation. Sign in to Orris to start your own chat.