Increased size of fetal kidneys
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the causes and evaluation of increased fetal kidney size.
Increased Size of Fetal Kidneys
Enlarged fetal kidneys are an important prenatal finding, most often detected on ultrasound. The kidneys should be measured in the midsagittal and axial planes and compared with standard reference tables; kidney size may appear normal before 20 weeks' gestation. To confirm enlargement, the kidneys must appear disproportionately large and are often echogenic (brighter than the liver).
Key Causes
1. Autosomal Recessive Polycystic Kidney Disease (ARPKD)
The most significant cause of massively enlarged fetal kidneys.
- Gene: PKHD1 (carrier rate 1:70)
- Ultrasound: Kidneys >5 SD above mean, bilateral, echogenic, with loss of corticomedullary differentiation
- Associated findings: Small/absent bladder, oligohydramnios or anhydramnios (80% of cases), possible hepatomegaly
- Pathology: Up to 100% of collecting ducts are affected by fusiform dilation; kidneys can enlarge up to 20× normal size while retaining reniform shape
- Outcome: 30–40% neonatal mortality from pulmonary hypoplasia; 1-year survival ~95% for those who survive the neonatal period
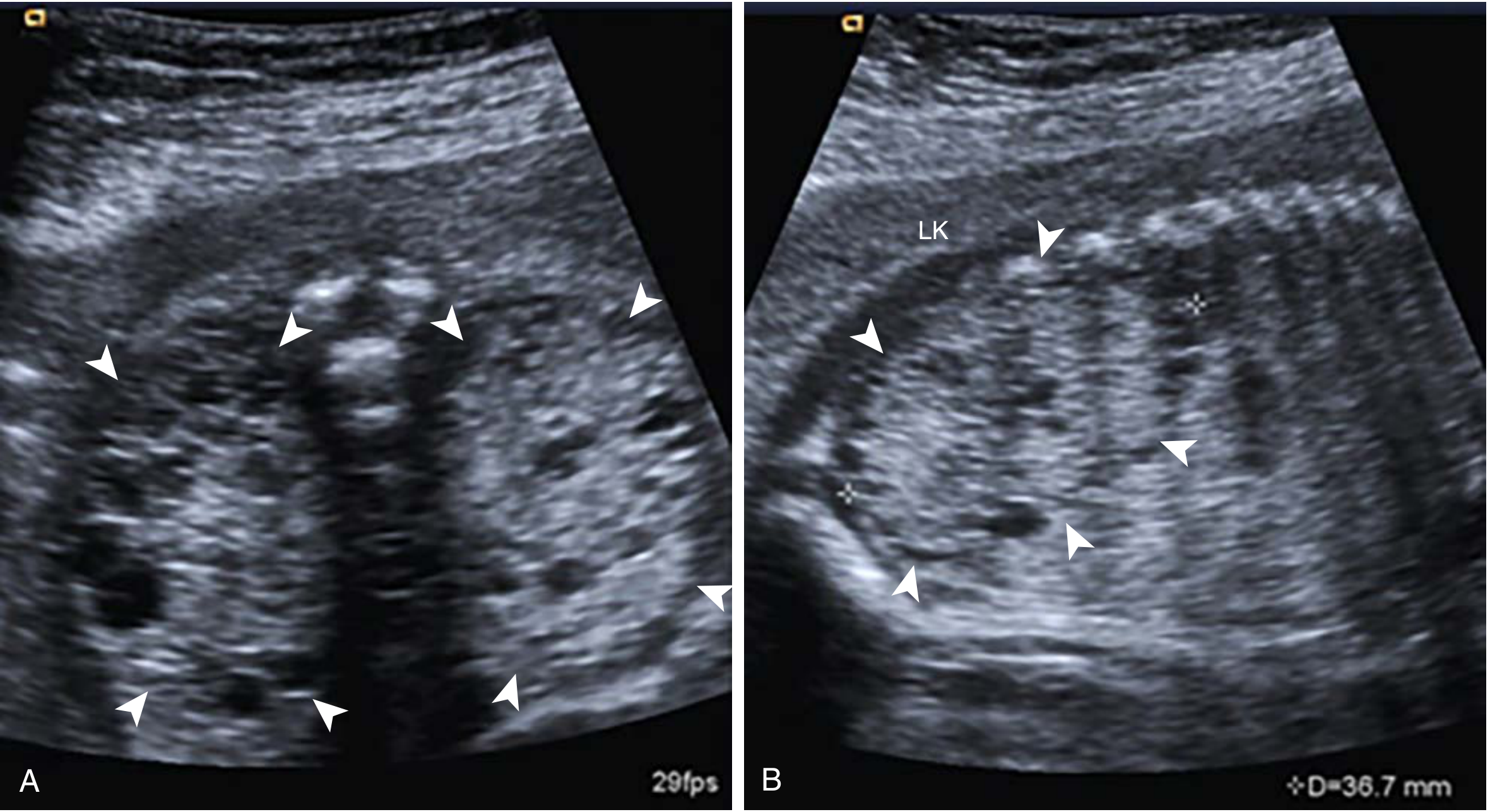
ARPKD at 21 weeks — bilateral enlarged echogenic kidneys with absent amniotic fluid (Creasy & Resnik's Maternal-Fetal Medicine)
2. Autosomal Dominant Polycystic Kidney Disease (ADPKD)
- Genes: PKD1, PKD2
- Ultrasound: Moderately enlarged echogenic kidneys with increased corticomedullary differentiation; discrete cysts atypical prenatally
- Associated findings: Normal bladder, normal amniotic fluid; parent(s) with renal cysts
- Discrete cysts are unusual in utero; presentation is milder than ARPKD
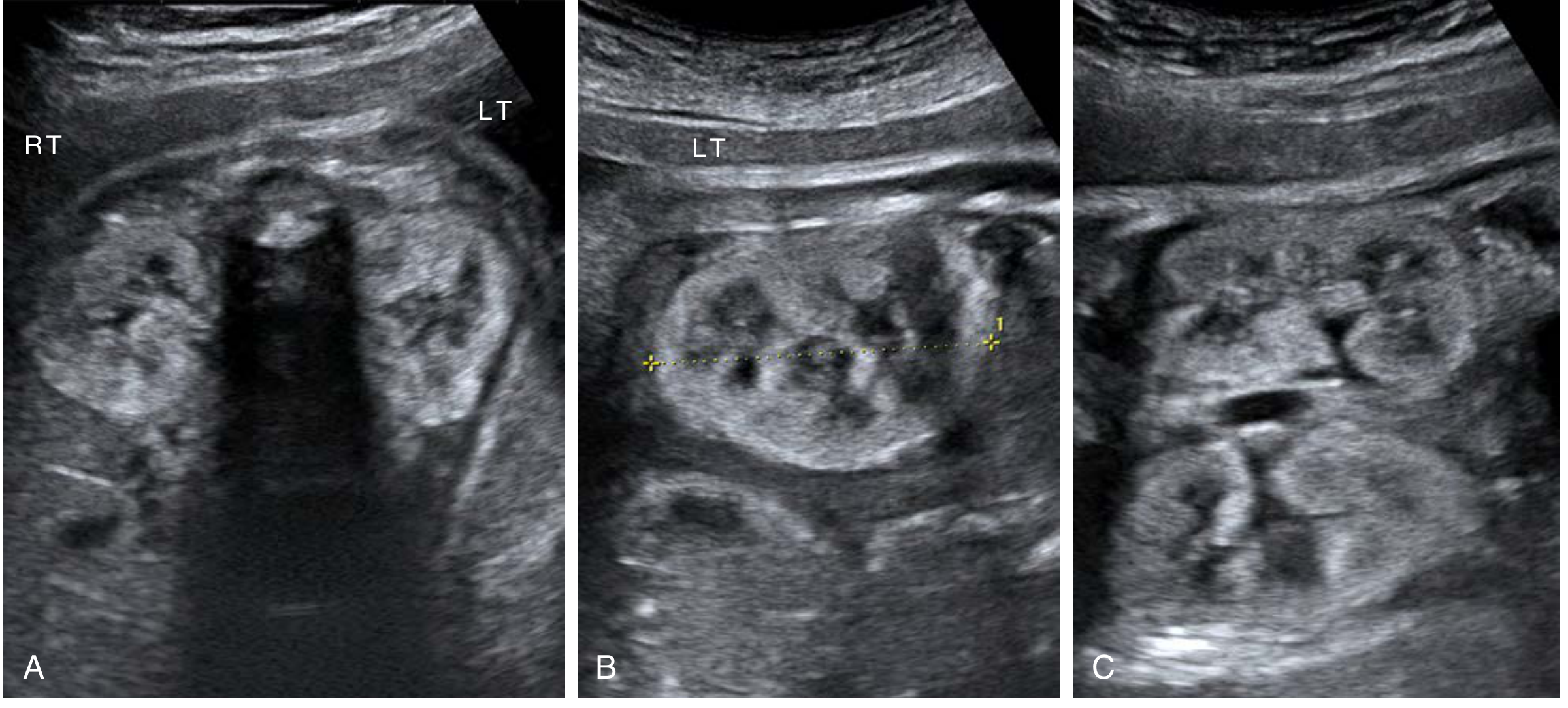
ADPKD at 31 weeks — echogenic kidneys with preserved corticomedullary differentiation (Creasy & Resnik's Maternal-Fetal Medicine)
3. Syndromes Associated with Enlarged Echogenic Kidneys
| Syndrome | Key Additional Features | Genetics |
|---|---|---|
| Meckel-Gruber syndrome | Multicystic enlarged kidneys + occipital encephalocele + polydactyly ± oligohydramnios | AR (MKS1, TMEM67, CEP290, etc.) |
| Bardet-Biedl syndrome | Large hyperechogenic kidneys + polydactyly ± genital anomalies | AR (BBS1–12, TMEM67, CEP290) |
| Beckwith-Wiedemann syndrome | Organomegaly (bilateral symmetric renal enlargement) + macroglossia + omphalocele | Imprinting defect 11p15 |
| Perlman syndrome | Renal hamartomas, nephroblastomatosis, macrosomia | AR (DIS3L2) |
| Finnish-type nephrotic syndrome | Enlarged cystic kidneys + elevated AFP | AR (NPHS1) |
| Oro-facial-digital syndrome | Cystic kidneys + oral/facial/digital anomalies | X-linked (OFD1) |
4. Large Dysplastic Kidneys
- Cystic elements can generate a large kidney; most extreme example is multicystic dysplastic kidney (MCDK)
- Large dysplastic kidneys are also a feature of somatic overgrowth syndromes (Beckwith-Wiedemann, Simpson-Golabi-Behmel)
- Postnatal ultrasound shows increased echogenicity, loss of corticomedullary differentiation, and cortical cysts
5. Echogenic Kidneys (Differential — not always enlarged)
Other causes of echogenic (and occasionally large) kidneys include:
- TCF2 deletions — most frequent genetic cause of fetal echogenic kidney
- Tuberous sclerosis (often with cardiac rhabdomyomas)
- CMV infection
- Renal vein thrombosis
- Trisomy 13, 18, 21
- Normal variant
Diagnostic Approach
- Measure kidneys in midsagittal and axial planes; compare with gestational-age reference tables
- Assess echogenicity (must be brighter than liver to be considered echogenic), corticomedullary differentiation, presence of cysts
- Assess amniotic fluid — oligohydramnios strongly suggests impaired urine production
- Look for extrarenal anomalies (CNS, digits, face) to identify syndromic causes
- Family history — affected siblings or parent with renal cysts guides ARPKD/ADPKD distinction
- Fetal MRI is warranted when oligohydramnios or maternal body habitus limits ultrasound
- Genetic testing — chromosomal microarray and gene panel for inherited causes
Prognosis
- Hyperechoic renal parenchyma is associated with abnormal renal function in 80% of cases
- Oligo/anhydramnios + large echogenic kidneys (>4 SD) in the second trimester = poor prognosis (pulmonary hypoplasia + renal failure)
- Normal or increased amniotic fluid = good prognosis for neonatal survival
- Nonisolated hyperechoic kidneys with extrarenal anomalies carry ~75% perinatal mortality
Sources: Creasy & Resnik's Maternal-Fetal Medicine, 8e; Campbell-Walsh-Wein Urology, 12e; NKF Primer on Kidney Diseases, 8e
Not hyperechogenic only slightly enlarged kidneys
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.