give me a table with 15 columns and 1 image of diarrhea
Reading File
search_medical_text
diarrhea etiology classification diagnosis management
search_medical_image
diarrhea pathophysiology intestinal
GradeResponse
GradeResponse
Here is a comprehensive table on diarrhea with 15 columns, followed by the image.
Diarrhea: 15-Column Clinical Reference Table
| # | Category | Definition | Onset | Duration | Mechanism | Common Pathogens / Causes | Key Symptoms | Stool Characteristics | Diagnosis | First-Line Treatment | Antibiotic Use | Rehydration Approach | Prevention | Complications |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Acute Watery | ≥3 loose stools/day | Sudden | < 14 days | Secretory / osmotic | Norovirus, rotavirus, ETEC, Vibrio cholerae | Nausea, vomiting, cramps | Watery, high-volume, no blood | Clinical; stool culture if severe | Oral rehydration; loperamide for mild-moderate | Not recommended for viral; azithromycin for traveler's diarrhea | Balanced electrolyte solution (ORS) in elderly/cholera; fluids + saltines otherwise | Hand hygiene; avoid high-risk foods while traveling | Dehydration, electrolyte imbalance |
| 2 | Dysentery | Bloody diarrhea with mucus | Sudden | < 14 days | Invasive / inflammatory | Shigella, Salmonella, Campylobacter, EIEC, Entamoeba histolytica | Fever, tenesmus, bloody stool | Small-volume, bloody, mucoid | Stool culture; PCR if available | Antibiotics (azithromycin, fluoroquinolone) | Indicated — directed by culture/sensitivity | ORS; IV fluids if severe | Food/water safety; cook meats thoroughly | Sepsis, HUS, toxic megacolon |
| 3 | Traveler's Diarrhea (TD) | Diarrhea acquired abroad | Within 1–2 wks of travel | 3–5 days | Usually bacterial secretory | ETEC (most common), Campylobacter, Shigella, norovirus | Abrupt loose stools, cramps, low-grade fever | Watery, sometimes bloody | Clinical; culture if persistent | Bismuth subsalicylate; loperamide + antibiotic if moderate-severe | Azithromycin or rifaximin; chemoprophylaxis in high-risk groups | ORS; sports drinks | Pre-travel counseling; avoid uncooked food/tap water | Post-infectious IBS |
| 4 | Persistent Diarrhea | Diarrhea lasting 14–30 days | Variable | 14–30 days | Mixed or parasitic | Giardia lamblia, Cryptosporidium, Cyclospora | Bloating, fatigue, weight loss | Fatty/loose, foul-smelling | Stool O&P; antigen EIA; PCR | Metronidazole (Giardia); nitazoxanide (Crypto) | Targeted antiparasitic | Continued ORS; nutritional support | Safe water (boiling, filtration) | Malabsorption, nutritional deficiency |
| 5 | Chronic Diarrhea | Diarrhea > 30 days | Insidious | > 30 days | IBD, malabsorption, functional | Crohn's, UC, celiac disease, IBS, microscopic colitis | Weight loss, nocturnal stools, blood/mucus | Variable — watery to fatty | Colonoscopy, biopsy, serologies, breath tests | Treat underlying cause (5-ASA, steroids, gluten-free diet) | Rarely indicated | Per underlying disease | Management of underlying condition | Anemia, malnutrition, colon cancer risk (IBD) |
| 6 | Secretory Diarrhea | Large-volume watery diarrhea | Variable | Variable | Active ion secretion (e.g., CFTR activation by cholera toxin) | Cholera toxin, VIPoma, carcinoid | Profuse watery stool, minimal pain | Large-volume, watery, "rice-water" in cholera | Clinical + stool osmotic gap (< 50 mOsm/kg) | Aggressive ORS/IV fluids; treat cause | Doxycycline for cholera | IV fluids (Ringer's lactate) for severe cholera | Cholera vaccine; safe water | Severe dehydration, death if untreated |
| 7 | Osmotic Diarrhea | Stool driven by unabsorbed solutes | Rapid after ingestion | Stops with fasting | Osmotic pull of water into lumen | Lactase deficiency, sorbitol, lactulose, Mg antacids | Bloating, flatulence | Watery; high osmotic gap (> 125 mOsm/kg) | Dietary history; hydrogen breath test | Eliminate offending agent | Not indicated | ORS if dehydrated | Dietary modification | Usually self-limited; nutritional gaps if prolonged |
| 8 | Antibiotic-Associated Diarrhea | Diarrhea during/after antibiotic course | During or up to 8 wks post-antibiotics | Days to weeks | Microbiome disruption; C. difficile toxin | Clostridioides difficile (severe), Clostridium perfringens | Watery diarrhea; fever; abdominal pain; pseudomembranous colitis in C. diff | Watery; may be bloody in C. diff | Stool GDH + toxin EIA; PCR for C. diff | Discontinue offending antibiotic; metronidazole or vancomycin for C. diff | Vancomycin or fidaxomicin for C. difficile | ORS | Judicious antibiotic use; probiotics if post-antibiotic | Pseudomembranous colitis, toxic megacolon, recurrence |
| 9 | Inflammatory Diarrhea | Diarrhea with mucosal damage | Variable | Variable | Mucosal invasion / cytokine release | IBD flare, radiation enteritis, ischemic colitis | Bloody stool, fever, severe cramps | Bloody, mucoid, small-volume | Endoscopy + biopsy; fecal calprotectin | Corticosteroids, biologics (IBD); supportive | Not usually indicated | IV fluids in severe cases | IBD management adherence | Perforation, stricture, toxic megacolon |
| 10 | Malabsorptive Diarrhea | Failure to absorb nutrients | Insidious | Chronic | Mucosal damage or enzyme deficiency | Celiac disease, short bowel syndrome, pancreatic insufficiency | Steatorrhea, weight loss, bloating | Fatty, pale, foul-smelling, floats | Fecal fat; D-xylose test; celiac serology; imaging | Dietary restriction (gluten-free); pancreatic enzymes | Not indicated | Nutritional support; fat-soluble vitamin replacement | Treat underlying disease | Malnutrition, osteoporosis, anemia |
| 11 | Functional Diarrhea / IBS-D | Chronic diarrhea without structural cause | Variable | Chronic, intermittent | Altered gut motility + visceral hypersensitivity | Stress, prior infection (post-infectious IBS), diet | Urgency, cramping, relieved by defecation | Loose to watery, no blood | Rome IV criteria; diagnosis of exclusion | Low-FODMAP diet; loperamide; antispasmodics | Not indicated | Not typically needed | Stress reduction; dietary management | Impaired quality of life; anxiety |
| 12 | Neonatal / Pediatric Diarrhea | Diarrhea in infants and children | Acute or chronic | Variable | Viral (most common); osmotic in formula intolerance | Rotavirus, norovirus, adenovirus; cow's milk protein allergy | Vomiting, irritability, fever, dehydration signs | Watery, yellow-green | Clinical; rotavirus antigen test | ORS (Pedialyte); continue breastfeeding | Avoid antibiotics for viral; azithromycin for Campylobacter | Low-osmolarity ORS | Rotavirus vaccine; breastfeeding; hand hygiene | Severe dehydration, death in low-income settings |
| 13 | Immunocompromised Diarrhea | Diarrhea in HIV/transplant/chemo patients | Variable | Prolonged | Opportunistic infections; GvHD; drug side effects | CMV colitis, Cryptosporidium, MAC, Microsporidium | Chronic profuse diarrhea, weight loss, fever | Watery, large-volume | Endoscopy + biopsy; stool PCR panel | Treat specific pathogen; ART optimization in HIV | Pathogen-directed (ganciclovir for CMV, etc.) | Aggressive hydration; nutritional support | ART adherence; prophylaxis | Wasting syndrome, sepsis, death |
| 14 | Drug-Induced Diarrhea | Diarrhea caused by medication | Shortly after drug initiation | Resolves with discontinuation | Direct mucosal irritation; motility changes; osmotic | Metformin, antibiotics, NSAIDs, colchicine, chemotherapy, laxatives | Loose stools, cramps; no fever | Variable | Medication review; temporal correlation | Discontinue or reduce offending drug; switch formulation | Not indicated | ORS if dehydrated | Medication counseling; dose titration | Usually self-limited; dehydration if severe |
| 15 | Food Poisoning / Toxin-Mediated | Rapid-onset diarrhea after ingestion of contaminated food | Within hours (1–6 hrs for toxin; 8–16 hrs for spore-forming) | 24–48 hrs | Pre-formed toxin ingestion | Staphylococcus aureus, Bacillus cereus, Clostridium perfringens | Sudden nausea, vomiting, profuse diarrhea | Watery, non-bloody | Clinical; food history; stool culture in outbreaks | Supportive — fluids and rest | Not indicated (toxin, not live infection) | ORS; IV fluids if unable to tolerate oral | Safe food handling, refrigeration, cooking temperatures | Dehydration; electrolyte disturbances |
Image: Pathophysiology of Secretory Diarrhea (Mouse Ileal Loop Model)
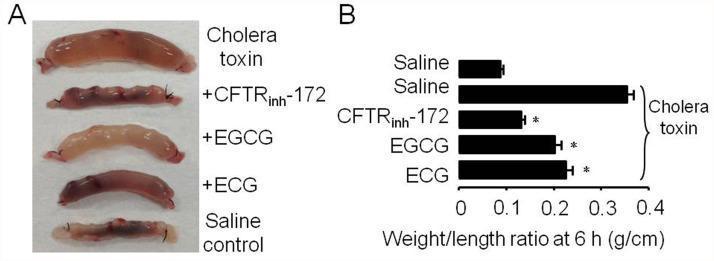
Figure: Experimental mouse ileal loop model illustrating secretory diarrhea. Panel A shows bowel distension caused by cholera toxin versus saline control. Treatment with CFTR inhibitor (CFTRinh-172) or green tea polyphenols (EGCG, ECG) visibly reduces fluid accumulation. Panel B quantifies bowel weight-to-length ratios — cholera toxin alone produces the highest ratio (~0.35 g/cm), while CFTR inhibition and polyphenol treatment significantly reduce this (p < 0.001), demonstrating the central role of CFTR chloride channels in secretory diarrhea. (Source: PMC Clinical VQA)
Sources: "Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults" (p. 3); Harrison's Principles of Internal Medicine; PMC Clinical VQA dataset.
This is a shared conversation. Sign in to Orris to start your own chat.