Fusion procedure of spine
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching Images
spinal fusion procedure ALIF PLIF TLIF posterior lumbar interbody
Loading Image
Loading Image
Finding Sources
Here is a comprehensive overview of spinal fusion procedures, drawing from authoritative surgical and orthopedic textbooks.
Spinal Fusion (Arthrodesis)
Definition
Spinal fusion is a surgical procedure that permanently joins (fuses) two or more vertebrae so that they heal into a single, solid bony unit, eliminating motion at that segment.
— Gray's Anatomy for Students
Indications
Indications have significantly broadened over time. Core indications include:
- Mechanical pain — from the disc (discogenic pain) or posterior elements (facet arthropathy)
- Stabilization after fracture — especially osteoporotic vertebral fractures (OVFs)
- Neurologic compromise — spinal cord, conus, or nerve root compression with neurologic deficit (especially when acute, incomplete, and progressive)
- Progressive painful spinal deformity — scoliosis (idiopathic, neuromuscular), kyphoscoliosis, kyphosis
- Fracture nonunion / pseudarthrosis
- Tumor infiltration causing instability
- Spinal instability — e.g., in rheumatoid arthritis (subaxial subluxation >4 mm), ankylosing spondylitis, cervical myelopathy
- Spondylolisthesis, degenerative disc disease
— Gray's Anatomy for Students; Rockwood & Green's Fractures in Adults, 10e; Miller's Review of Orthopaedics, 9e
Surgical Approaches
There are three main access corridors, and they may be combined:
1. Posterior Approach
Fusion of posterior elements (facets, transverse processes, laminae). Most commonly adopted. Typically involves:
- Posterolateral fusion (PLF)
- Posterior lumbar interbody fusion (PLIF) — bilateral retraction of thecal sac, cage placed centrally
- Transforaminal lumbar interbody fusion (TLIF) — unilateral posterolateral approach, less neural retraction
2. Anterior Approach
Disc removal and anterior column reconstruction:
- Anterior lumbar interbody fusion (ALIF) — retroperitoneal approach, largest footprint cage, excellent sagittal alignment correction
- Anterior cervical discectomy and fusion (ACDF)
- Oblique lumbar interbody fusion (OLIF) — oblique anterolateral window between aorta and psoas
- Extreme lateral interbody fusion (XLIF) — direct lateral trans-psoas approach
3. 360-Degree (Combined) Fusion
Combines anterior and posterior constructs — provides strongest fixation and direct anterior decompression, at the cost of increased surgical time and morbidity.
Note: Anterior-only constructs should be avoided in metabolic bone disease (e.g., osteoporosis) due to poor substrate for plate/screw fixation and high risk of fixation failure.
— Gray's Anatomy for Students; Rockwood & Green's Fractures in Adults, 10e
Surgical Approaches — Axial CT Diagram
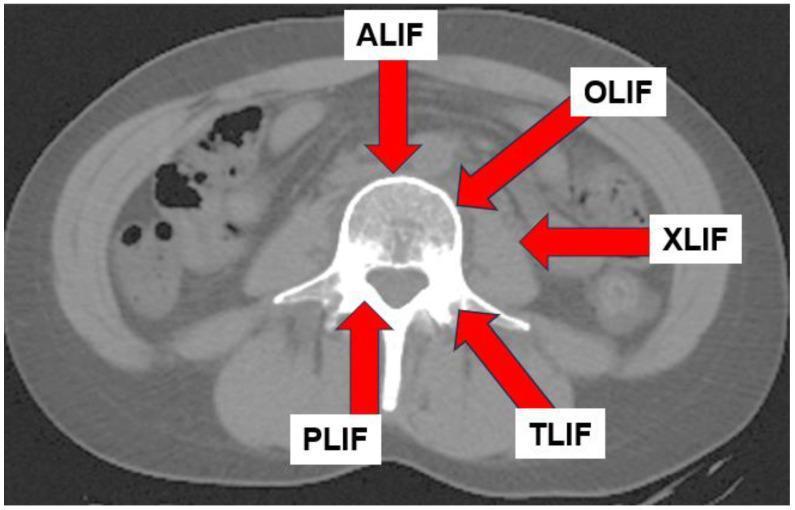
Axial CT of the lumbar spine showing the five main interbody fusion approach corridors.
Instrumentation & Fixation
Pedicle Screw Systems
The foundation of modern spinal fixation. Screws are placed through the pedicles into the vertebral body and connected by longitudinal rods. In osteoporotic bone:
- Cement augmentation of pedicle screws significantly reduces fixation failure risk
- Cement can be injected prior to screw placement or via cannulated fenestrated screws
- Novel technique: SAIF (Stent-Screw-Assisted Internal Fixation) — uses vertebral body stents + fenestrated screws to prevent cement leakage and restore vertebral height
Interbody Cages
Titanium, PEEK, or carbon fiber spacers packed with bone graft material, placed in the disc space to:
- Restore disc height
- Provide structural anterior column support
- Create a scaffold for bony fusion
Cross-links
Connect bilateral rods to enhance rotational stability.
— Rockwood & Green's Fractures in Adults, 10e
Postoperative Radiograph (L4–L5 TLIF/PLIF)

AP and lateral radiographs of a single-level posterior lumbar interbody fusion at L4–L5 showing bilateral pedicle screws, connecting rods, and a wedge-shaped interbody cage.
Bone Grafting
Fusion requires biologic material to stimulate new bone growth across the segment:
| Graft Type | Source | Properties |
|---|---|---|
| Autograft (iliac crest) | Patient's own bone | Gold standard — osteogenic, osteoinductive, osteoconductive |
| Allograft | Cadaveric bone bank | Osteoconductive, osteoinductive; no donor site morbidity |
| Bone morphogenetic protein (BMP) | Recombinant (rhBMP-2) | Powerful osteoinductive; used off-label in spinal fusion |
| Bone graft substitutes | Synthetic (calcium phosphate, etc.) | Osteoconductive scaffold |
| Demineralized bone matrix (DBM) | Processed allograft | Osteoinductive; used as extender |
BMP combined with autograft in non-instrumented spinal fusion models has shown augmented healing capacity, though evidence remains controversial.
— Rockwood & Green's Fractures in Adults, 10e
Special Scenarios
Cervical Spine (Rheumatoid Arthritis)
- Subaxial subluxation >4 mm → posterior spinal fusion ± decompression
- Anterior fusion if sagittal alignment restoration needed or to improve fusion rates in multilevel posterior constructs
Scoliosis
- Idiopathic: posterior spinal fusion with segmental instrumentation for curves meeting surgical threshold
- Neuromuscular (e.g., Duchenne MD): posterior spinal fusion with segmental instrumentation to the pelvis, ideally before pulmonary/cardiac deterioration
- "Growth-friendly" techniques (growing rods, VEPTR, Shilla) used to avoid premature fusion in young children; formal fusion deferred
Osteoporotic Vertebral Fractures
- Posterior-based constructs preferred
- Adjuncts: cement-augmented screws, anterior column reconstruction, combined approaches
- Staging of procedures reduces risk of perioperative complications (e.g., postoperative visual loss in long-duration cases)
— Miller's Review of Orthopaedics, 9e; Rockwood & Green's Fractures in Adults, 10e
Key Complications
| Complication | Notes |
|---|---|
| Pseudarthrosis (nonunion) | Failed fusion — may require revision; associated with smoking, NSAIDs |
| Adjacent segment disease | Accelerated degeneration above/below fusion level |
| Hardware failure | Screw loosening, rod breakage, cage migration |
| Neurologic injury | From retraction, screw malposition |
| Perioperative visual loss (POVL) | Ischemic optic neuropathy — risk increased with long-duration and multilevel fusion; staging reduces risk |
| Infection / wound dehiscence | |
| Junctional fractures | Especially in osteoporotic patients with long constructs |
NSAIDs postoperatively are typically avoided after spinal fusion due to dose-dependent inhibition of fusion healing. Spine surgeons generally do not permit NSAID use in the postoperative fusion period.
— Miller's Anesthesia, 10e; Rockwood & Green's Fractures in Adults, 10e
Summary
Spinal fusion is a versatile procedure spanning the full length of the spine, adaptable through multiple surgical corridors (anterior, posterior, lateral, combined). Modern techniques combine rigid instrumentation with biologic grafting to achieve solid arthrodesis. Patient selection, surgical approach, fixation strategy, and bone quality are the key determinants of outcome.
Anterior lumbar interbody fusion
Finding Sources
Finding Sources
Searching Images
anterior lumbar interbody fusion ALIF technique cage placement
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Anterior Lumbar Interbody Fusion (ALIF)
Definition
ALIF is a lumbar interbody fusion technique performed through an anterior (retroperitoneal or transperitoneal) approach, in which the intervertebral disc is completely excised and replaced with a structural cage or graft to achieve solid anterior column arthrodesis.
— Gray's Anatomy for Students; Grainger & Allison's Diagnostic Radiology
Indications
- Degenerative disc disease (discogenic axial low back pain)
- Spondylolisthesis (isthmic or degenerative)
- Lumbar instability
- Revision surgery — pseudarthrosis after posterior fusion
- Sagittal imbalance / loss of lumbar lordosis requiring restoration
- Adjacent segment disease
- Lumbar disc pathology unsuitable for posterior access (e.g., L5–S1 with high iliac crest)
- As the anterior component of a 360° combined fusion
Surgical Approach
Access Corridor
The anterior lumbar spine is accessed via one of two routes:
| Route | Description |
|---|---|
| Retroperitoneal (more common) | Left-sided approach; peritoneum swept anteriorly to expose L4–L5 and L5–S1 without entering the abdomen |
| Transperitoneal | Peritoneal cavity entered; allows access to L5–S1 but higher visceral complication risk |
A vascular surgeon or access surgeon typically performs the approach and vessel retraction. The left common iliac artery and vein and the aortic bifurcation must be carefully mobilized. At L5–S1, the middle sacral vessels are ligated.
Key Steps
- Patient positioned supine with lumbar lordosis maintained
- Retroperitoneal dissection — peritoneum swept to the right
- Identification and retraction of great vessels (aorta, inferior vena cava, iliac vessels)
- Preservation of the superior hypogastric plexus (anterior to L5–S1 disc)
- Complete anterior annulotomy and discectomy
- Thorough endplate preparation (decortication)
- Sizing and insertion of interbody cage ± bone graft / BMP
- Fluoroscopic confirmation of cage position
- Optional supplementary posterior fixation (pedicle screws)
The Cage
ALIF allows placement of a significantly larger footprint cage than posterior techniques because there is no neural tissue to work around. This is a key advantage.
Cage Types
- Rectangular / lordotic wedge-shaped — restores disc height and lumbar lordosis
- Ring-type cages (e.g., LT-CAGE) — oval, hollow center packed with bone graft/BMP; two cages placed side by side
- Stand-alone ALIF cage with integrated screws — fixation into adjacent endplates without posterior instrumentation
- Expandable cages — allow in-situ height adjustment
Materials
Titanium, PEEK (polyether ether ketone), carbon composite polymers — radiolucent materials have radiopaque markers for fluoroscopic guidance.
— Grainger & Allison's Diagnostic Radiology; Rockwood & Green's Fractures in Adults, 10e
Imaging
AP Radiograph — Dual LT-CAGE Placement at L5–S1
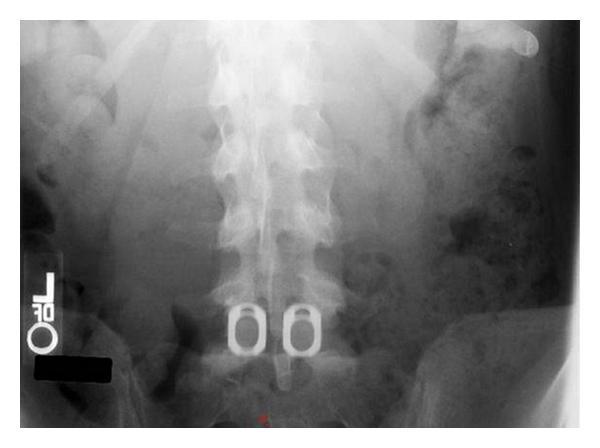
AP radiograph: two radiopaque ring-type LT-CAGEs placed side-by-side at L5–S1 following ALIF. Wide spacing (6 mm) maximizes decorticated endplate area for bone graft/BMP integration.
Intraoperative Lateral Fluoroscopy — L5–S1 ALIF

Intraoperative lateral fluoroscopy at L5–S1 showing a standalone ALIF cage with integrated screws extending into both adjacent endplates.
Coronal CT — Successful ALIF (Bridwell Grade I Fusion)
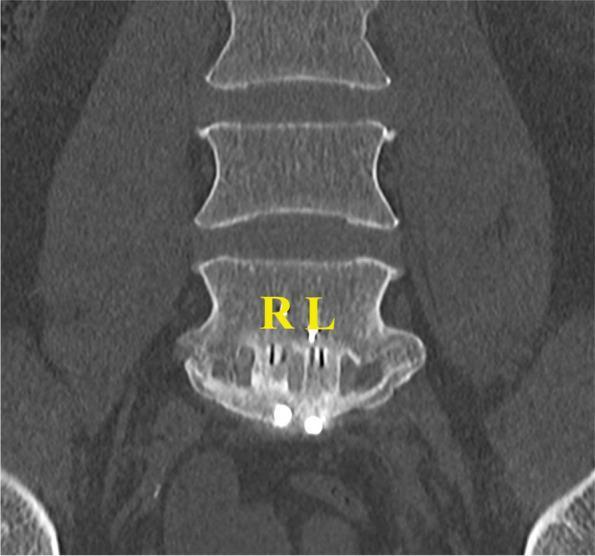
Coronal CT: complete bony bridging through the ALIF cage (right chamber: bioactive glass; left chamber: autologous bone), classified as Bridwell Grade I fusion.
Advantages Over Posterior Approaches
| Feature | ALIF | PLIF/TLIF |
|---|---|---|
| Cage footprint | Largest — covers full endplate | Smaller |
| Disc removal | Complete | Partial |
| Lordosis restoration | Excellent | Moderate |
| Neural retraction | None required | Required |
| Posterior musculature | Preserved | Disrupted |
| Access to L5–S1 | Excellent (not limited by iliac crest) | Limited at L5–S1 |
| Paraspinal muscle damage | None | Significant (open) |
Bone Grafting / Biologics
- Autologous iliac crest bone graft (ICBG) — traditional gold standard; donor site pain is a recognized morbidity
- Recombinant BMP-2 (rhBMP-2) — powerful osteoinductive agent; widely used in ALIF cages (off-label); associated with heterotopic ossification and retrograde ejaculation risk
- Allograft / DBM / ceramics — used alone or as extenders
— Grainger & Allison's Diagnostic Radiology; Cummings Otolaryngology (bone graft reference)
Complications
Approach-Related (Anterior)
| Complication | Mechanism |
|---|---|
| Retrograde ejaculation | Injury to the superior hypogastric sympathetic plexus (T10–L2 fibers coursing anterior to L5–S1 disc); reported rates up to 5–10% in men |
| Vascular injury | Left common iliac vein most vulnerable; can be catastrophic |
| Ureteral injury | Rare; ureter must be identified and protected |
| Ileus / bowel injury | Retroperitoneal dissection; more common with transperitoneal approach |
| Venous thromboembolism | Prolonged vessel retraction, immobility |
| Wound infection / hernia | Abdominal wall complication |
The sympathetic thoracolumbar fibers (T10–L2) are susceptible to injury during transperitoneal anterior lumbar discectomy and interbody fusion. Complaints of loss of ejaculation (failure of emission or retrograde ejaculation) are common after these surgeries. The ability to experience orgasm is typically retained. — Bradley & Daroff's Neurology in Clinical Practice
Fusion-Related
| Complication | Features |
|---|---|
| Pseudarthrosis | Risk factors: smoking, diabetes, obesity, osteoporosis, multilevel surgery |
| Cage subsidence | Soft or osteoporotic endplates; loss of disc height restoration |
| Cage migration / retropulsion | May compress neural structures — requires revision |
| Adjacent segment disease | Accelerated degeneration above fusion level |
| Infection / spondylodiscitis | Requires aggressive management; CT/MRI for diagnosis |
Postoperative Imaging Assessment
- Plain radiographs — hardware position, cage migration, alignment; dynamic flexion–extension views for pseudarthrosis
- CT — gold standard for fusion assessment; evaluates cage position, endplate integrity, bone bridging (Bridwell classification)
- MRI — soft tissue and neural evaluation; identifies epidural haematoma, abscess, adjacent segment disease
Hardware failure (fractured screws, cage subsidence) should be suspected if plain radiographs show >4 mm translation or >10° angular motion on flexion–extension views; CT demonstrates lucent lines at graft–bone interface indicating pseudarthrosis. — Grainger & Allison's Diagnostic Radiology
Bridwell Fusion Classification (CT)
| Grade | Description |
|---|---|
| I | Solid bridging bone, no lucency |
| II | Graft intact, no lucency, remodeling visible |
| III | Graft intact but with lucency at top or bottom |
| IV | Graft collapsed, lucency through graft |
Summary
ALIF provides unparalleled access to the anterior disc space, enabling complete discectomy, large-footprint cage placement, excellent disc height and lordosis restoration, and biologic-rich graft environments — all without disrupting posterior musculature or neural structures. The tradeoff is the need for an access surgeon, risk to major vessels, and the unique risk of retrograde ejaculation from superior hypogastric plexus injury. It is the preferred approach at L5–S1 and in patients requiring significant sagittal alignment correction.
Posterior lumbar body interfusion
Finding Sources
Finding Sources
Searching Images
posterior lumbar interbody fusion PLIF technique cage pedicle screws
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Loading Image
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.