Hi orris
Hey! How can I help you today?
Can u give me Notes for the topic jvp medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here are comprehensive notes on Jugular Venous Pressure (JVP) compiled from Harrison's Principles of Internal Medicine (2025), Braunwald's Heart Disease, Medical Physiology, and other authoritative sources.
📋 JVP - Jugular Venous Pressure: Complete Notes
1. INTRODUCTION
- JVP is the single most important bedside measurement for estimating volume status and right atrial (RA) pressure
- Reflects right atrial pressure indirectly
- Internal jugular vein (IJV) is preferred over the external jugular vein (EJV)
- EJV is valved and not directly in line with the SVC and right atrium
- EJV can still be used to discriminate high vs. low CVP
2. HOW TO MEASURE JVP
- Patient positioned at 45 degrees (can vary: 30°, 45°, or 60°)
- Measure the vertical height of the venous pulsation above the sternal angle (angle of Louis)
- Add 5 cm (distance from sternal angle to mid-right atrium)
- Formula: JVP (cmH2O) = height above sternal angle (cm) + 5
- Normal: ≤ 8 cmH2O at rest
- Abnormal: >4.5 cm above sternal angle at 30° elevation
- Conversion: 1.36 cmH2O = 1.0 mmHg
- If venous pulsation is visible above the clavicle in sitting position = clearly abnormal (distance from clavicle to RA is at least 10 cm)
Clinical tip: If elevated JVP is suspected in semi-supine position, place the patient sitting with legs dangling below the bedside.
3. JVP WAVEFORM
The JVP waveform has 3 peaks and 3 descents:
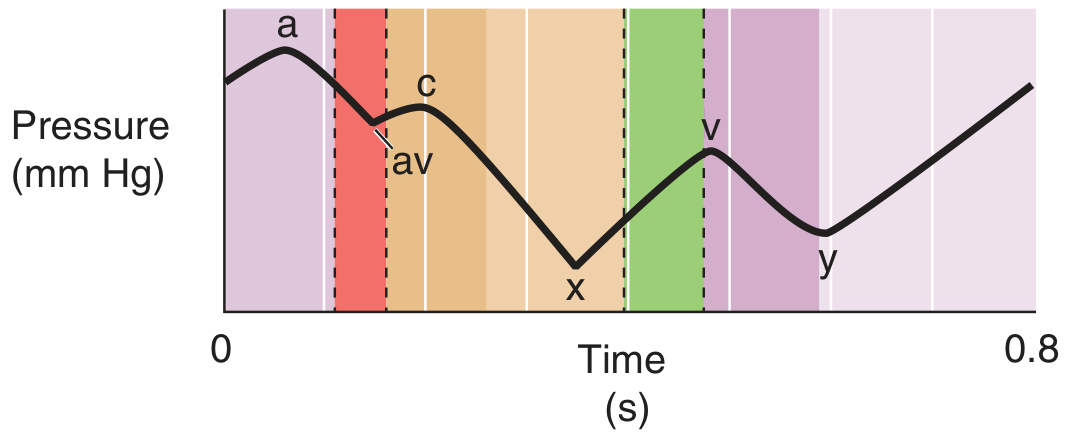
PEAKS (positive deflections):
| Wave | Timing | Cause |
|---|---|---|
| a wave | Just after P wave on ECG, before S1 | Right atrial presystolic contraction |
| c wave | Early ventricular systole | Tricuspid valve bulging into RA during early RV systole; also carotid pulsation artifact |
| v wave | Ventricular systole (late), peaks at S2 | Atrial filling against a closed tricuspid valve |
DESCENTS (negative deflections):
| Descent | Cause |
|---|---|
| x descent | Fall in RA pressure after a wave; atrial relaxation + tricuspid valve pulled downward during ventricular systole |
| y descent | Fall in RA pressure after tricuspid valve opens; rapid ventricular filling |
| av (minor) | Relaxation of RA + closure of tricuspid valve |
4. JVP vs. CAROTID PULSE - How to Distinguish
| Feature | JVP | Carotid Pulse |
|---|---|---|
| Waveform | Biphasic (a + v) in sinus rhythm | Monophasic |
| Obliteration by pressure | YES (easily obliterated) | No (cannot be obliterated) |
| Changes with posture | YES (decreases on sitting up) | No |
| Changes with inspiration | YES (decreases normally) | No |
| Palpable | No | Yes |
5. ABNORMAL JVP WAVEFORMS - High Yield
🔺 Elevated JVP (Raised JVP)
Causes:
- Right heart failure (most common)
- Cardiac tamponade - elevated JVP + muffled heart sounds + hypotension (Beck's triad)
- Constrictive pericarditis
- SVC obstruction
- Fluid overload / hypervolemia
- Pulmonary hypertension
- Tricuspid stenosis/regurgitation
- Restrictive cardiomyopathy
📊 Specific Waveform Abnormalities:
| Abnormality | Finding | Cause |
|---|---|---|
| Absent a wave | No a wave visible | Atrial fibrillation |
| Prominent a wave | Large a wave | Reduced RV compliance, RV hypertrophy, tricuspid stenosis |
| Cannon a wave | Huge a wave | AV dissociation (RA contracts against closed tricuspid valve) - identifies wide complex tachycardia as ventricular in origin |
| Large v wave (CV fusion = Lancisi's sign) | Prominent v wave merging with c | Tricuspid regurgitation - waveform becomes "ventricularized" |
| Prominent x descent | Sharp x | Cardiac tamponade, normal |
| Absent x descent | - | Tricuspid regurgitation |
| Prominent y descent | Sharp, rapid y | Constrictive pericarditis (corresponds to pericardial knock) |
| Absent/slow y descent | Flat y | Cardiac tamponade, tricuspid stenosis |
6. KEY CLINICAL SIGNS INVOLVING JVP
Kussmaul's Sign
- Paradoxical rise (or failure to fall) in JVP with inspiration
- Normally JVP falls with inspiration (intrathoracic pressure decreases)
- Seen in:
- Constrictive pericarditis
- Restrictive cardiomyopathy
- Severe biventricular heart failure
- RV infarction
- Cardiac tamponade (occasionally)
Hepatojugular Reflux (HJR) / Abdominojugular Test
- Apply firm pressure over the right upper quadrant (liver) for 15-30 seconds
- Patient must breathe normally (not strain/Valsalva)
- Positive = sustained rise in JVP ≥ 3-4 cmH2O
- Abdominojugular test: Firm midabdominal compression for 10s → rise in RA pressure → abrupt drop on release
- Suggests elevated left-sided filling pressures
- Positive HJR has high specificity for heart failure
Friedreich's Sign
- Sharp and deep Y descent in JVP
- Seen in: Constrictive pericarditis
7. JVP IN SPECIFIC CONDITIONS
| Condition | JVP | Key Feature |
|---|---|---|
| Right heart failure | Elevated | Prominent v waves if TR present |
| Cardiac tamponade | Elevated | Prominent x descent, absent y descent |
| Constrictive pericarditis | Elevated | Kussmaul's sign, Friedreich's sign (prominent y descent), pericardial knock |
| Tricuspid regurgitation | Elevated | Giant cv/v wave, absent x, "ventricularized" waveform, Lancisi's sign |
| Tricuspid stenosis | Elevated | Large a wave, slow y descent |
| Atrial fibrillation | Variable | Absent a wave |
| AV dissociation / VT | Variable | Cannon a waves |
| Hypovolemia | Low JVP | Flat neck veins |
| Cardiogenic shock | Elevated JVP | Low CO, elevated SVR |
| Distributive shock | Low JVP | High CO, low SVR |
8. PROGNOSTIC SIGNIFICANCE
- Elevated JVP has important prognostic value in heart failure
- Predicts higher risk of:
- Hospitalization for heart failure
- Death from heart failure
- Right atrial pressure >10 mmHg (bedside JVP) has 88% positive predictive value for pulmonary artery wedge pressure >22 mmHg
- Changes in JVP with therapy parallel changes in left-sided filling pressures
9. RESPIRATORY EFFECTS ON JVP
- Normal inspiration: JVP falls (decreased intrathoracic pressure → more venous return → RA empties better)
- Kussmaul's sign: JVP rises with inspiration (constrictive pericarditis, restrictive disease, severe RHF)
- The respiratory cycle modulates mean venous pressure via changes in intrathoracic pressure
QUICK REVISION SUMMARY
JVP Waveform:
a (RA contraction) → av ↓ → c (tricuspid bulge) → x ↓ (atrial relaxation)
→ v (atrial filling) → y ↓ (tricuspid opens)
High-yield associations:
• No a wave = AF
• Cannon a wave = AV dissociation / VT
• Large v wave = Tricuspid regurgitation
• Absent y descent = Tamponade
• Prominent y + Kussmaul's = Constrictive pericarditis
• Kussmaul's sign = Constrictive pericarditis / Restrictive CMP / RV infarct
Sources: Harrison's Principles of Internal Medicine 22E (2025), Braunwald's Heart Disease 12th Ed, Medical Physiology (Boron & Boulpaep), Fuster & Hurst's The Heart 15th Ed, The Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.