Organizational tactics in acs with or without st segment elevation in comorbid patients at prehospital and in the hospital
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive synthesis of organizational tactics for ACS (STEMI and NSTEMI/UA) in comorbid patients, covering both prehospital and in-hospital phases.
Organizational Tactics in ACS (STEMI & NSTEMI/UA): Prehospital and In-Hospital — With Focus on Comorbid Patients
1. The Systems-Based Framework
ACS management is no longer a single-provider act — it is a chain-of-survival system spanning EMS, the ED, the catheterization lab (CCL), and the coronary care unit (CCU). STEMI systems of care emphasize:
- Time-sensitivity of every step
- Multidisciplinary team composition
- Parallel (not serial) activation of resources
The "Four Ds" framework captures the key process points for STEMI:
- Door — events before and at ED arrival
- Data — ECG acquisition
- Decision — diagnosis and reperfusion choice
- Drug/Device — fibrinolytic or PCI catheter placement
— ROSEN's Emergency Medicine, p. 994
2. Prehospital Organizational Tactics
2.1 Prehospital ECG — the Single Most Important Prehospital Tool
- A prehospital 12-lead ECG has 99% specificity and 93% positive predictive value for STEMI in patients with atraumatic chest pain
- Increases paramedic scene time by only 1–3 minutes
- Enables early hospital notification, parallel in-hospital preparation, and patient destination routing based on PCI capability
- Reduces time to hospital-based reperfusion (shown across urban, suburban, and rural settings)
Advantages of prehospital ECG include:
- Earlier STEMI detection
- Patient routing to PCI-capable center
- Pre-arrival hospital preparation (activating the cath lab team)
- More rapid initiation of reperfusion (fibrinolytic or primary PCI)
— ROSEN's Emergency Medicine, p. 994; Roberts and Hedges' Clinical Procedures in Emergency
2.2 Prehospital Notification and Hospital Activation
- Prehospital notification to the ED of an impending STEMI patient is now standard in established EMS systems
- This allows parallel activation of the STEMI Alert response before the patient arrives
- Selected STEMI systems allow direct ambulance-to-CCL bypass of the ED — this significantly decreases door-to-reperfusion time (though mortality benefit data remain inconclusive)
2.3 Prehospital Medication
Prehospital administration of ASA 325 mg is standard. For STEMI, prehospital ticagrelor loading has been studied (ATLANTIC trial) to address the problem that STEMI patients remain vulnerable to recurrent thrombosis even after receiving P2Y12 inhibitors — strategies include tablet crushing and IV platelet inhibitors. — Fuster and Hurst's The Heart, p. [acute phase]
2.4 Diagnosing ACS in Comorbid/Atypical Patients Prehospitally
ACS diagnosis in the prehospital setting is difficult because chest pain is a poor predictor of AMI, and adjunctive tools are limited. The following comorbid populations frequently have atypical or no chest pain:
| Comorbidity/Population | Typical Atypical Presentation |
|---|---|
| Diabetes mellitus | Dyspnea; 40% of diabetic MIs go unrecognized; scar without antemortem diagnosis 3× more common |
| Older adults (>85 y) | 60–70% present with anginal equivalents (weakness, dyspnea, altered mental status, extreme fatigue) |
| Women | <60% report typical chest pain; report dyspnea, indigestion, unusual fatigue, dizziness |
| Non-white populations | Higher rate of atypical presentations; documented disparity in treatment |
| Patients with prior CHF or stroke | Coincident ACS masked by the underlying condition |
| Dementia | Cannot reliably report symptoms |
Key principle: Dyspnea is the most common anginal equivalent. For prehospital personnel, recognizing a "different symptom" — not a classic one — is the key to catching ACS in comorbid patients. — ROSEN's Emergency Medicine, p. 994
3. In-Hospital Organizational Tactics
3.1 Immediate ED Triage
- Self-transported patients with possible ACS: triage nurse evaluation immediately, with ECG within 5–10 minutes of arrival
- ECG must be interpreted rapidly by a competent clinician — the goal is STEMI detection and life-threat exclusion; formal interpretation follows during full evaluation
- Hospital-based protocols and response plans are essential to reduce time-to-treatment
3.2 STEMI Pathway
Reperfusion strategy selection:
- If primary PCI is available: Activate the STEMI Alert — cardiologist and cath lab personnel mobilized immediately. Prehospital or ED-based activation yields high accuracy (low false-activation rate) while dramatically reducing time to definitive therapy.
- If only fibrinolysis is available: Emergency clinician activates the hospital reperfusion system. Checklists of inclusion/exclusion criteria must be available and fibrinolytic agents stored/administered in the ED. Consultative discussions before fibrinolysis should only be obtained in complicated situations — nonconsultative communications with other physicians should not cause delay.
- Interhospital transfer for PCI when the patient is also a fibrinolysis candidate: discouraged if definitive therapy will be delayed.
— ROSEN's Emergency Medicine, p. 1024
3.3 NSTEMI/UA Pathway — Risk Stratification Drives Organizational Decisions
All NSTEMI/UA patients receive:
- ASA
- Dual antiplatelet therapy (ASA + P2Y12 inhibitor: clopidogrel, ticagrelor, or prasugrel)
- Anticoagulation (UFH or LMWH; bivalirudin is an alternative)
- Nitrates, beta-blockers, oxygen (as needed)
Risk stratification determines invasive strategy timing (Table 4-11, Washington Manual):
| Timing | Criteria |
|---|---|
| Immediate/urgent (<2 h) | Refractory angina; worsening HF/MR; hemodynamic instability/shock; sustained VT/VF |
| Early invasive (<24 h) | High-risk score (TIMI ≥3 or GRACE >140); rapid rise in biomarkers; new ST depressions |
| Delayed invasive (24–72 h) | Diabetes; renal insufficiency (GFR <60); LVEF <40%; early post-infarction angina; prior PCI within 6 months; prior CABG; TIMI ≥2 or GRACE 109–140 |
| Ischemia-driven (conservative) | Low-risk (TIMI ≤1 or GRACE <109); low-risk biomarker-negative female patients; patient/clinician preference with no high-risk features |
Key for comorbid patients: Severe comorbid conditions such as advanced CKD, liver failure, or active malignancy may shift the balance toward an ischemia-driven strategy when risk outweighs benefit. However, a routine invasive strategy is generally recommended unless the risk clearly outweighs the benefit. — Washington Manual, p. 134–138
3.4 Comorbidity-Specific In-Hospital Considerations
NSTEMI/UA patients carry more comorbidities than STEMI patients — both cardiac and noncardiac. — Washington Manual, p. 131
Diabetes:
- Demand ischemia (Type 2 NSTEMI) is common in the setting of severe physiologic stress
- Atypical symptoms increase diagnostic delay; maintain a low threshold for testing
- Delayed invasive strategy (24–72 h) is appropriate tier for diabetic patients with intermediate risk
Renal insufficiency (GFR <60):
- Falls in the delayed invasive tier
- Contrast nephropathy risk must be weighed; minimize contrast volume, consider hydration protocols
- Dose-adjust anticoagulants (LMWH → UFH if GFR <30; monitor anti-Xa)
Reduced LVEF (<40%):
- Also in delayed invasive tier
- Indicates prior myocardial damage, higher risk of cardiogenic shock
- HF management (volume status optimization) must occur in parallel
Women:
- Worse short-term and long-term outcomes in NSTEMI/UA due to delays in symptom recognition and underutilization of guideline-directed therapy and invasive management
- Low-risk biomarker-negative women may appropriately receive ischemia-driven strategy
Older adults:
- Present with coincident ACS in the setting of infection, trauma, or surgery
- Comprehensive approach (detailed history, physical exam, serial biomarkers, ECG) is required because ECG and biomarker changes may be nonspecific due to age-related changes and coexisting comorbidities — Sabiston Textbook of Surgery, p. [elderly ACS section]
3.5 ACS Diagnostic Algorithm
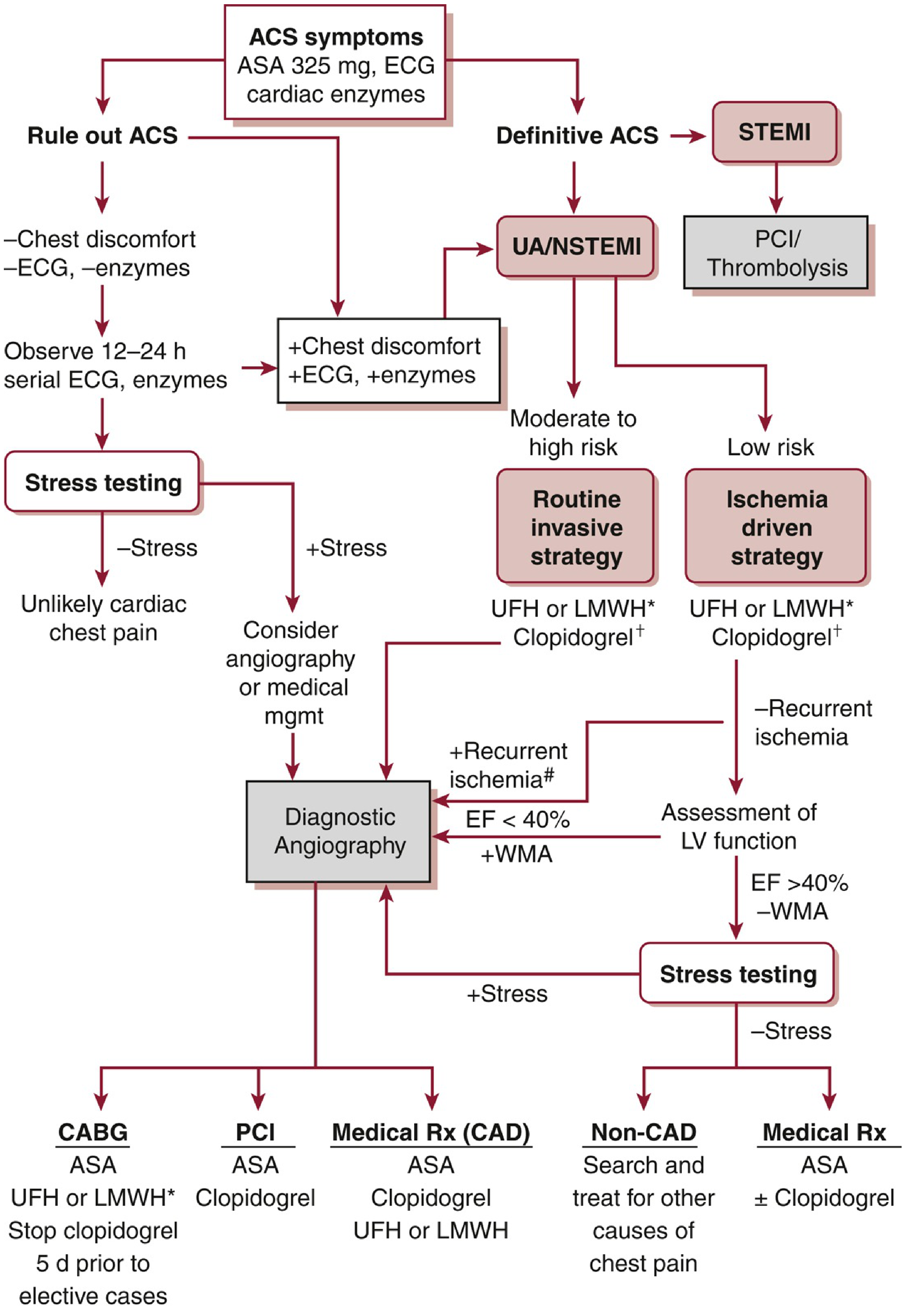
Figure: Diagnostic and therapeutic approach to ACS focusing on antiplatelet and antithrombotic therapy. STEMI → PCI/Thrombolysis. UA/NSTEMI → risk-stratified invasive vs. ischemia-driven strategies. — Washington Manual of Medical Therapeutics
3.6 TIMI Risk Score (Quantifying Risk in NSTEMI/UA)
Score 1 point for each:
- Age >65 years
- Known CAD (stenosis >50%)
- ≥2 episodes of chest pain in 24 hours
- ST-segment or T-wave changes
- Elevated cardiac biomarkers
- ASA use in the last 7 days
- ≥3 CAD risk factors (family history, DM, HTN, hyperlipidemia, tobacco)
Higher TIMI scores → higher 14-day rates of death, MI, or urgent revascularization → guide escalation toward routine invasive strategy. — Washington Manual, p. 134
3.7 ED Pharmacologic Management (Summary Table from ROSEN's)
| Medication Class | Examples | Indications | Risk Issues |
|---|---|---|---|
| Nitroglycerin | SL, topical, IV | Chest pain, pulmonary edema, BP control | Hypotension |
| Opioids | Morphine, fentanyl | Chest pain | Hypotension, respiratory suppression |
| β-Blockers (IV) | Metoprolol, labetalol, esmolol | BP, dysrhythmia control | Hypotension, bradycardia, cardiogenic shock |
| β-Blockers (oral) | Metoprolol | Inpatient use | — |
| ACE Inhibitors | Captopril, enalapril | HF, post-MI LV dysfunction | Hypotension, renal impairment |
4. Rule-Out ACS Strategy for Low-Risk / Indeterminate Patients
For patients without definitive ACS findings:
- Serial ECG and biomarker testing (12–24 h observation)
- High-sensitivity troponin protocols have shortened R/O MI time, increased detection, and improved throughput
- If biomarkers and ECG are negative → stress testing → if positive, consider angiography; if negative → unlikely cardiac chest pain
- The R/O MI process can be performed in the ED, observation unit, or acute care setting
Reducing the missed MI rate below current levels risks increasing unnecessary testing, resource overuse, and harm. Atypical, unanticipated ACS presentations will occur and not always be diagnosed initially — this does not represent inappropriate practice. — ROSEN's Emergency Medicine, p. 994
Summary
| Phase | Key Organizational Tactic |
|---|---|
| Prehospital | Prehospital 12-lead ECG; hospital pre-notification; direct-to-CCL bypass in selected STEMI; recognize atypical presentations in comorbid patients |
| ED Triage | ECG within 5–10 min; STEMI Alert activation; fibrinolysis checklist |
| STEMI in-hospital | Primary PCI preferred; fibrinolysis if PCI unavailable/delayed; avoid consultative delays |
| NSTEMI/UA in-hospital | Universal ASA + anticoagulation; TIMI/GRACE risk scoring; timing of invasive strategy stratified by risk and comorbidities |
| Comorbid adjustments | Diabetics → delayed invasive tier; CKD → UFH preference, contrast minimization; low LVEF → parallel HF management; women → avoid under-treatment; elderly → low threshold for testing |
Stemi and nstemi management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, textbook-sourced guide to STEMI and NSTEMI management.
STEMI & NSTEMI/UA Management
STEMI — Overview
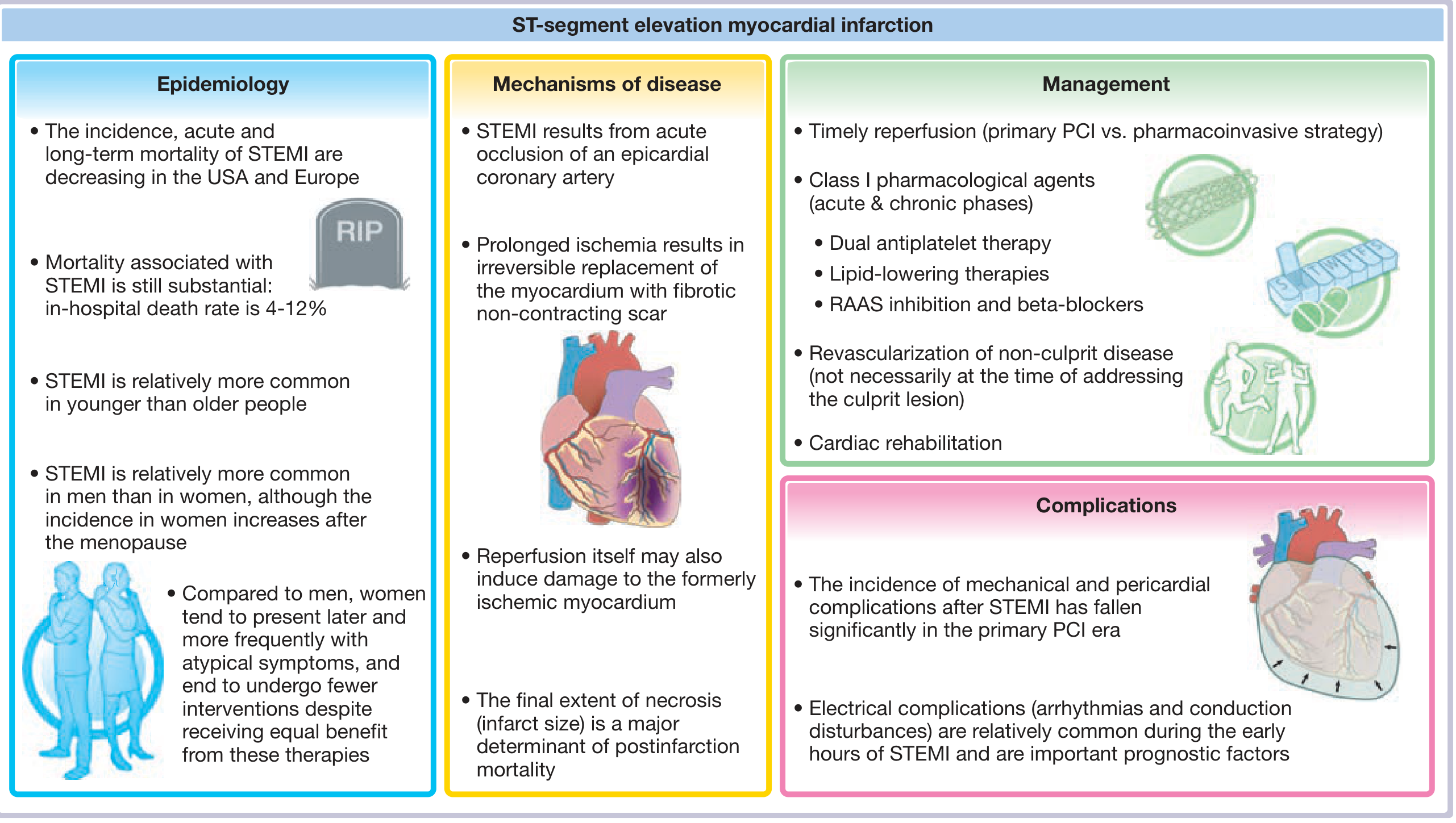
Fuster and Hurst's The Heart, 15th Ed. — Central Illustration: STEMI
1. STEMI: Reperfusion Strategy (The Core Decision)
Timely reperfusion is the most effective intervention. It has reduced in-hospital STEMI mortality from ~20% to ~5% over three decades. The reperfusion decision hinges on time from symptom onset to wire crossing (PCI) or time from diagnosis to fibrinolytic bolus.
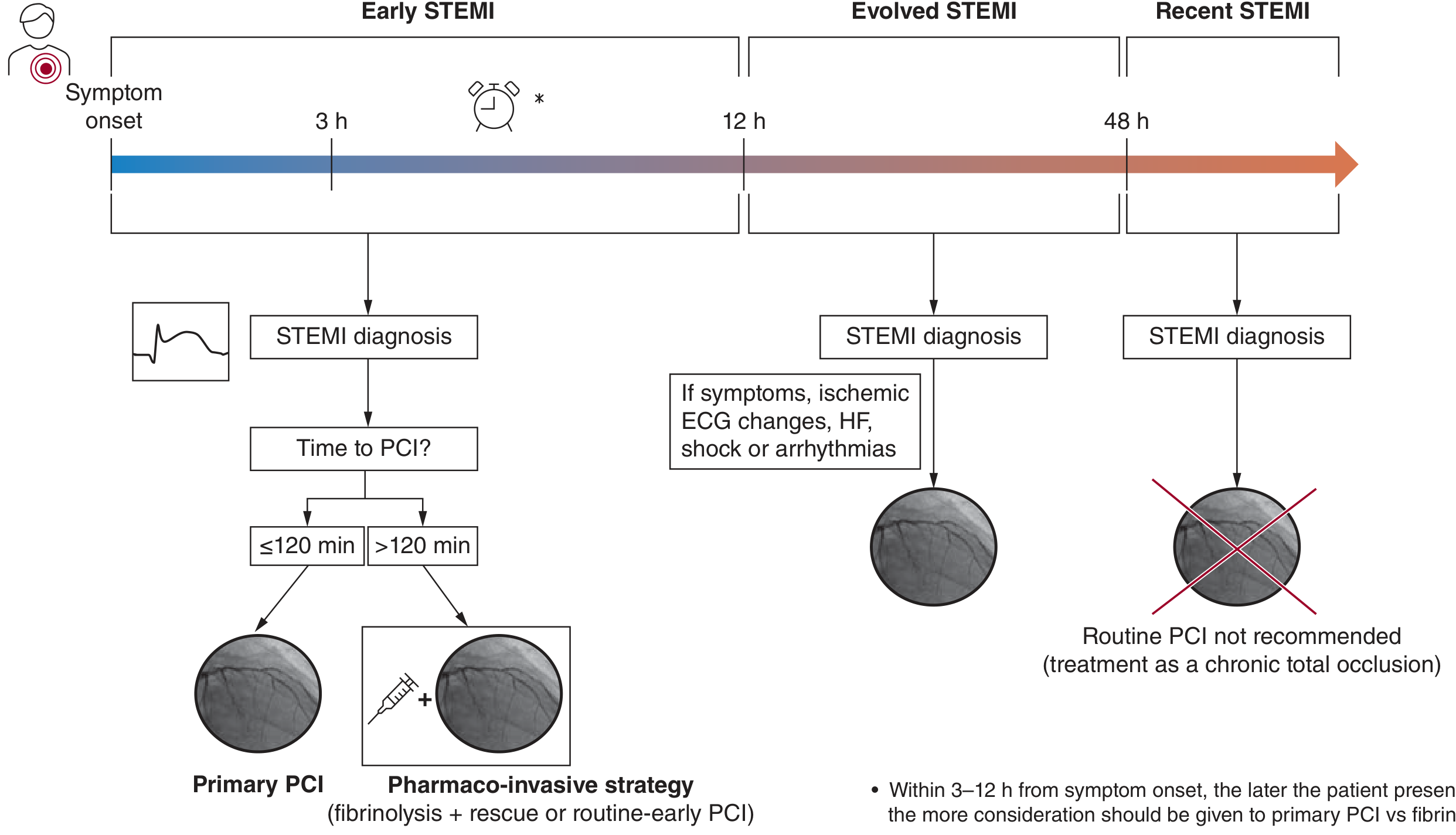
Figure 18-7: Selection of reperfusion strategy by time from symptom onset — Fuster and Hurst's The Heart
1.1 Early STEMI (<12 Hours from Symptom Onset)
Primary PCI (pPCI) is preferred over fibrinolysis when it can be performed within 120 minutes of STEMI diagnosis by an experienced team. A large meta-analysis of 23 RCTs confirmed pPCI reduces death, reinfarction, and stroke compared to thrombolytics. — Fuster and Hurst's The Heart, p. 605
Fibrinolysis is used when pPCI is not achievable within 120 minutes:
- Fibrin-specific agents are preferred
- Must be administered within 10 minutes of STEMI diagnosis
- Prehospital lytic administration is feasible, safe, and associated with reduced long-term mortality
- Efficacy decreases as time elapses (coronary thrombi mature, becoming harder to lyse)
- After fibrinolysis → pharmaco-invasive strategy: routine-early or rescue PCI follows
1.2 Fibrinolysis Contraindications
| Absolute |
|---|
| Previous intracranial hemorrhage or stroke of unknown origin at any time |
| Ischemic stroke in the preceding 6 months |
| Central nervous system tumour or AVM |
| Major trauma, surgery, or head injury in the preceding 3 weeks |
| GI bleeding within the past month |
| Known bleeding disorder |
| Aortic dissection |
| Non-compressible punctures in past 24 hours |
Relative contraindications include: TIA in preceding 6 months, anticoagulant therapy, pregnancy, refractory hypertension (SBP >180), advanced liver disease, infective endocarditis, and active peptic ulcer.
1.3 Evolved STEMI (12–48 Hours)
- Reperfusion indicated only if symptoms persist, with ongoing ischemic ECG changes, heart failure, shock, or arrhythmias
1.4 Recent STEMI (>48 Hours)
- Routine PCI is NOT recommended — treat as a chronic total occlusion
2. STEMI: Antithrombotic Therapy
Antiplatelet Therapy
Aspirin (ASA): 150–325 mg loading dose → 75–100 mg daily indefinitely
P2Y12 Inhibitors (Dual Antiplatelet Therapy — DAPT):
| Agent | Loading / Maintenance | Key Points |
|---|---|---|
| Ticagrelor | 180 mg load / 90 mg BID | PLATO trial: ↓16% CV death/MI/stroke vs clopidogrel; preferred in STEMI |
| Prasugrel | 60 mg load / 10 mg daily | TRITON-TIMI 38: ↓19% primary endpoint vs clopidogrel; avoid in prior stroke/TIA, age ≥75, weight <60 kg |
| Clopidogrel | 300–600 mg load / 75 mg daily | Alternative when ticagrelor/prasugrel contraindicated |
Note on delayed onset: >30% of STEMI patients treated with ticagrelor or prasugrel show high platelet reactivity for up to 2 hours post-ingestion. Solutions include prehospital administration, tablet crushing, or IV cangrelor. — Fuster and Hurst's The Heart, p. 610
Cangrelor: IV, reversible P2Y12 inhibitor with very short half-life → rapid potent platelet inhibition; bridge to oral agents or use when oral dosing is not possible.
DAPT Duration:
- Standard: 12 months post-STEMI
- Short DAPT (3–6 months) can be considered when bleeding risk is high
- De-escalation strategies (e.g., switching from prasugrel/ticagrelor to clopidogrel) are evidence-based options
- Dual pathway inhibition beyond 1 year (ASA + low-dose rivaroxaban 2.5 mg BID) for selected high-risk patients
Anticoagulants (Acute Phase)
| Agent | Use Case |
|---|---|
| UFH | Preferred during primary PCI |
| Enoxaparin (LMWH) | STEMI managed conservatively or beyond 24h; avoid if GFR <30 (use UFH) |
| Bivalirudin | At least as effective as heparin for PCI; direct thrombin inhibitor; no heparin-induced thrombocytopenia risk |
| Fondaparinux | Alternative anticoagulant; do not use as sole anticoagulant during PCI (catheter thrombosis risk) |
Switching between UFH and LMWH during active treatment increases bleeding risk — avoid crossover. — ROSEN's Emergency Medicine, p. 1028
3. STEMI: Multivessel Disease Management
- 52% of STEMI patients have at least one non-infarct-related artery (non-IRA) with obstructive disease; 18.8% have three-vessel disease
- Complete revascularization (non-IRA PCI either at the index procedure or staged) is now preferred over culprit-only PCI — COMPLETE trial: complete revascularization reduced CV death/MI (7.8% vs 10.5% at 3 years; HR 0.74)
- Exception — Cardiogenic shock (CULPRIT-SHOCK trial): multivessel PCI at time of STEMI with shock does NOT improve outcomes and may be harmful → perform culprit-only PCI first; staged non-IRA PCI if patient stabilizes
4. STEMI: Adjunctive Pharmacological Therapy
Beta-Blockers
- Oral metoprolol in all haemodynamically stable patients without contraindications
- IV beta-blockers only for ongoing ischemia or tachyarrhythmia without HF or low output
- Contraindicated in cardiogenic shock, significant bradycardia, high-degree AV block, severe reactive airway disease
RAAS Inhibition
- ACE inhibitors (captopril, enalapril, ramipril): started within 24–48 h in patients with LVEF ≤40%, anterior STEMI, HF, hypertension, or diabetes. Continue indefinitely if LVEF reduced
- ARBs (valsartan): ACE-inhibitor intolerance
- Aldosterone antagonists (eplerenone): LVEF ≤40% + either HF symptoms or diabetes; eGFR >30, K⁺ <5.0
Statins
- High-intensity statin (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) started immediately, continued indefinitely
- Target LDL <55 mg/dL (<1.4 mmol/L); add ezetimibe or PCSK9 inhibitor if not achieved
Nitroglycerin
- IV NTG for ongoing chest pain, hypertension, pulmonary edema
- Contraindicated with phosphodiesterase inhibitor use, or if SBP <90 mmHg, or right ventricular infarction (hypotension risk)
5. STEMI: Complications
| Category | Examples |
|---|---|
| Electrical | VF/VT (peak in first hours — most important early mortality cause), bradyarrhythmias, AV blocks (inferior STEMI) |
| Mechanical | Free wall rupture, ventricular septal defect, papillary muscle rupture (acute MR) |
| Pericardial | Early pericarditis (days 1–3), Dressler syndrome (weeks later) |
| Pump failure | Cardiogenic shock, HF, RV infarction |
The incidence of mechanical and pericardial complications has fallen significantly in the primary PCI era. — Fuster and Hurst's The Heart
6. NSTEMI / Unstable Angina — Management
6.1 Definition and ECG
- UA: ischemia without myocardial necrosis (biomarkers negative); ECG may show ST depression or T-wave inversion or be normal
- NSTEMI: elevated biomarkers + clinical syndrome, without ST elevation; ECG typically shows ST depression, T-wave inversion, or nonspecific changes
- ST depression in V1–V4 may represent true posterior (inferobasal) MI → check posterior leads (V7–V9); any elevation in posterior leads = STEMI equivalent requiring emergent reperfusion
- Absence of ST elevation does NOT mean lower risk: in-hospital mortality with ST depression is similar to STEMI (~15–16%) — ROSEN's Emergency Medicine, p. 351
6.2 Universal Initial Therapy (All NSTEMI/UA)
All patients receive regardless of final revascularization strategy:
| Drug Class | Agent | Details |
|---|---|---|
| Antiplatelet | ASA | 325 mg immediately, then 75–100 mg daily |
| P2Y12 inhibitor | Ticagrelor (preferred) or clopidogrel | DAPT for 12 months |
| Anticoagulant | UFH or LMWH (enoxaparin) | UFH 48h or LMWH up to 8 days/until discharge |
| Statin | High-intensity | Start immediately |
| Beta-blocker | Oral metoprolol | Haemodynamically stable patients |
| Nitrates | SL / IV NTG | Symptom relief |
| ACE inhibitor / ARB | As above | LVEF ≤40%, HF, DM, HTN |
6.3 Risk Stratification: TIMI and GRACE Scores
TIMI Score (1 point each):
- Age >65
- Known CAD (stenosis >50%)
- ≥2 anginal episodes in 24 hours
- ST changes (depression/T-wave changes)
- Elevated cardiac biomarkers
- ASA use in last 7 days
- ≥3 CAD risk factors
GRACE Score: incorporates age, heart rate, SBP, creatinine, Killip class, ST deviation, elevated biomarkers, cardiac arrest at admission → more precise mortality prediction.
6.4 Invasive vs. Conservative Strategy — Timing
| Strategy | When |
|---|---|
| Immediate invasive (<2 h) | Refractory angina; hemodynamic instability/shock; sustained VT/VF; worsening HF or new MR |
| Early invasive (<24 h) | TIMI ≥3 or GRACE >140; rapidly rising biomarkers; new ST depressions |
| Delayed invasive (24–72 h) | Diabetes; CKD (GFR <60); LVEF <40%; early post-infarction angina; prior PCI <6 months; prior CABG; TIMI ≥2 or GRACE 109–140 |
| Ischemia-driven (conservative) | TIMI ≤1 or GRACE <109; low-risk biomarker-negative women; patient/clinician preference without high-risk features |
In NSTEMI/UA, a routine invasive approach reduces recurrent MI, hospitalizations, and death compared to conservative management — unless risk clearly outweighs benefit. — Washington Manual of Medical Therapeutics, p. 138
6.5 Anticoagulation in NSTEMI/UA
| Agent | Notes |
|---|---|
| Enoxaparin | 1 mg/kg SC BID; preferred over UFH for conservative management; reduce to 1 mg/kg daily if GFR <30 |
| UFH | Preferred if early PCI planned (<24h) or renal failure (GFR <30) |
| Bivalirudin | At time of PCI; alternative to UFH; patients already on UFH may switch to bivalirudin at PCI |
| Fondaparinux | Alternative; not to be used alone during PCI |
Only high-risk UA (ongoing pain, dynamic ECG changes, new ischemic changes) benefits from anticoagulation — a stable, pain-free UA patient with normal ECG and biomarkers may not require heparin. — ROSEN's Emergency Medicine, p. 1028
6.6 Post-Angiography Decisions
| Finding | Action |
|---|---|
| Culprit vessel amenable to PCI | PCI + stenting (ASA + clopidogrel post-PCI) |
| Left main / multivessel disease | CABG (stop clopidogrel/ticagrelor ≥5 days pre-elective CABG; prasugrel ≥7 days) |
| Non-obstructive CAD | Medical therapy: ASA ± P2Y12; search for other causes |
| Normal coronaries | Investigate for demand ischemia, vasospasm, myocarditis, MINOCA |
7. Comparison Summary: STEMI vs. NSTEMI Management
| Feature | STEMI | NSTEMI/UA |
|---|---|---|
| Hallmark | Persistent ST elevation; complete coronary occlusion | No ST elevation; partial occlusion or demand ischemia |
| Reperfusion timing | Emergent (minutes) | Risk-stratified (hours to days) |
| Primary strategy | pPCI if available within 120 min; fibrinolysis otherwise | Routine invasive vs. ischemia-driven by TIMI/GRACE |
| Antiplatelet | ASA + ticagrelor/prasugrel (preferred over clopidogrel) | ASA + ticagrelor or clopidogrel |
| Anticoagulation | UFH (pPCI); LMWH (conservative) | LMWH (preferred if no urgent PCI); UFH (urgent PCI) |
| Multivessel disease | Complete revascularization (staged or index PCI); culprit-only if shock | Directed by anatomy after angiography |
| Fibrinolysis | Yes — when PCI not available within 120 min | Never indicated |
| DAPT duration | 12 months standard | 12 months standard |
| RAAS/statin/BB | Universal in eligible patients | Universal in eligible patients |
Sources: Fuster and Hurst's The Heart (15th Ed.) — Chapter 18; ROSEN's Emergency Medicine (9th Ed.) — Chapter 64; The Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.