What is umbilical artery doppler
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
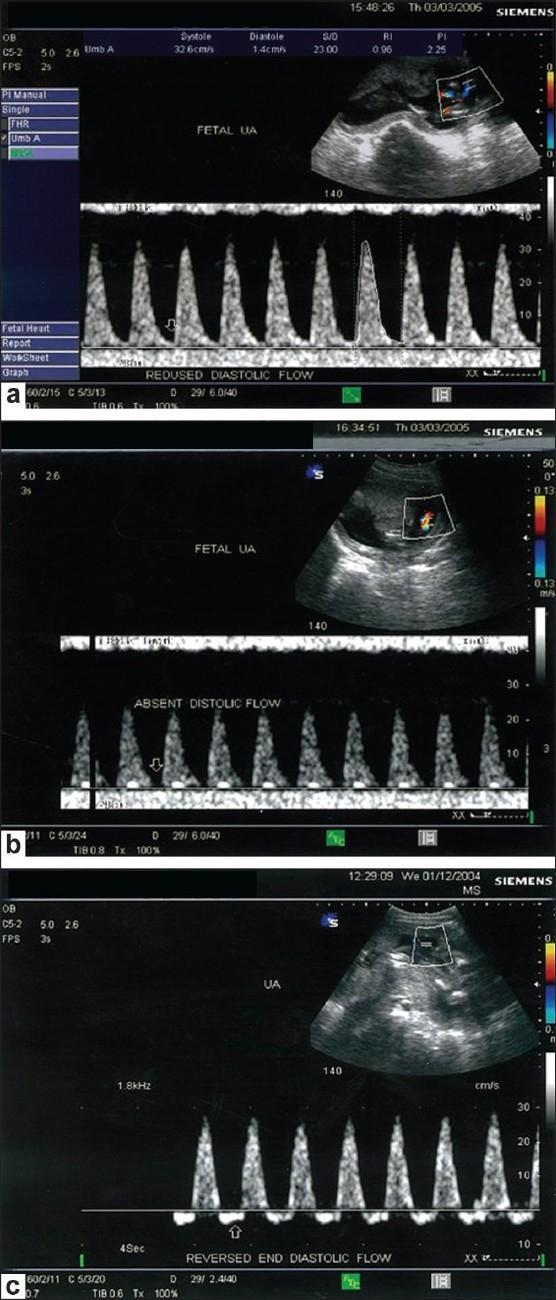
umbilical artery doppler waveform absent reversed end-diastolic flow
Loading Image
Loading Image
Reading File
I now have comprehensive textbook content. Let me compile the answer.
Umbilical Artery Doppler
Umbilical artery Doppler velocimetry is a non-invasive ultrasound technique that uses spectral Doppler to assess blood flow velocity waveforms in the umbilical artery, reflecting the vascular resistance of the placental circulation.
Physiological Basis
The umbilical arteries arise from the common iliac arteries and are the dominant outflow of the distal aortic circulation. Because they have no somatic branches after their origin, they purely mirror the downstream resistance of the placenta. Normally, umbilical artery resistance falls progressively through pregnancy as the number of tertiary stem villous vessels increases.
In pathological conditions (e.g., preeclampsia, chronic hypertension, FGR), obliteration or pruning of the placental arterial tree increases resistance, causing characteristic waveform changes. — Creasy & Resnik's Maternal-Fetal Medicine, p. 724
Technique
The Doppler sample gate is enlarged to encompass the entire vessel and sample a single umbilical artery. Because the Doppler index is calculated as a ratio of systolic to diastolic velocity, the angle of insonation does not affect measurement, making the technique reproducible.
Key indices used:
- S/D ratio (systolic-to-diastolic ratio)
- Resistive Index (RI) = (S − D) / S
- Pulsatility Index (PI) = (S − D) / mean velocity
Waveform Progression (Normal → Severely Abnormal)
| Finding | Meaning | Severity |
|---|---|---|
| Normal | Continuous forward diastolic flow, low resistance | Normal |
| Elevated S/D / PI | Rising placental resistance | Abnormal |
| Absent End-Diastolic Velocity (AEDV) | Flow reaches zero during diastole | Ominous |
| Reversed End-Diastolic Velocity (REDV) | Flow dips below baseline — retrograde during diastole | Severely ominous |
The elastic component added by an insufficiently compliant placenta causes retrograde recoil after each pulse, producing REDV.
Clinical Significance
- Beneficial in high-risk pregnancies (FGR, placental insufficiency, preeclampsia) — reduces perinatal mortality by up to 29% when added to antenatal testing in IUGR fetuses
- Not recommended for routine low-risk surveillance
The end-diastolic flow is the most important prognostic feature:
- AEDV: Odds ratio for fetal death 3.59 (fetal death rate ~6.8%) in FGR <34 weeks
- REDV: Odds ratio for fetal death 7.27 (fetal death rate ~19%) — often an unstable state that may precede fetal death by only hours to days
Adverse Outcomes Predicted by Abnormal UA Doppler
(BOX 32.1, Creasy & Resnik's, p. 725 — frequency rises from AEDV → REDV)
- Cesarean section for fetal distress
- Acidosis / Hypoxemia
- Low Apgar score
- Ventilator / long-term oxygen requirement
- Anemia, thrombocytopenia, transfusions
- Intraventricular hemorrhage
- Necrotizing enterocolitis
- Perinatal mortality
Management Implications
| Gestational Age | Finding | Action |
|---|---|---|
| >33–34 weeks | Persistent AEDV | Deliver |
| <33 weeks | AEDV | Individualize — multivariable fetal assessment (BPP, MCA Doppler, ductus venosus), consider antenatal steroids |
| Any GA | REDV | Prepare for delivery; antenatal steroids if BPP normal; refer to tertiary center |
| Any GA | AEDV or REDV | Rule out fetal anomalies/aneuploidy (~20% prevalence); consider karyotype/microarray |
Adjunct Doppler Studies
When UA findings worsen, the middle cerebral artery (MCA) and ductus venosus Doppler provide additional assessment of fetal systemic arterial and venous circulation respectively, particularly useful in the preterm fetus. — Creasy & Resnik's Maternal-Fetal Medicine, p. 724
What is a doppler in previous question
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have enough to give a clear, well-grounded answer.
What is Doppler? (in the context of umbilical artery Doppler)
The Doppler Effect — The Underlying Principle
Doppler refers to a technique based on the Doppler effect, a physical phenomenon first described by Austrian physicist Christian Doppler. It states that when a sound wave is reflected by a moving object, the frequency of the reflected wave is different from the transmitted frequency.
- If the object is moving toward the transducer → reflected frequency is higher
- If the object is moving away → reflected frequency is lower
This change in frequency is called the Doppler shift (Fs − FT).
In medical ultrasound, the "moving objects" are red blood cells flowing through blood vessels. The ultrasound machine transmits sound waves into the body, and the waves reflect off moving blood cells. By measuring the Doppler shift, the machine calculates blood flow velocity.
The Doppler Equation
$$v = \frac{c \cdot (F_s - F_T)}{2 \cdot F_T \cdot \cos\theta}$$
Where:
- v = blood flow velocity (m/s)
- c = speed of sound in blood (~1540 m/s)
- Fs = backscattered (received) frequency
- FT = transmitted frequency
- θ = angle between the ultrasound beam and the direction of blood flow
The angle (θ) is critical — the beam must be as parallel to blood flow as possible. A 90° angle gives zero signal; up to 20° deviation causes <6% error, which is acceptable. — Textbook of Clinical Echocardiography
Types of Doppler Used in Obstetrics
| Type | How it works | Use |
|---|---|---|
| Pulsed-wave (PW) Doppler | Sends pulses, times the return to sample a specific depth/location | Used for umbilical artery — samples a specific point in the cord |
| Continuous-wave (CW) Doppler | Constantly transmits and receives; no depth localization | High-velocity measurements |
| Color Doppler | Maps flow direction and velocity across an area using color coding (red = toward, blue = away from transducer) | Used to locate the umbilical artery visually before sampling |
| Power Doppler | Detects presence of flow regardless of direction; more sensitive | Used to confirm vessel presence (e.g., single umbilical artery) |
What Doppler Measures in the Umbilical Artery
In the umbilical artery, PW Doppler produces a spectral waveform — a graph of velocity over time across the cardiac cycle. From this, key indices are calculated:
- S/D ratio — peak Systolic velocity ÷ end-Diastolic velocity
- Resistive Index (RI) = (S − D) / S
- Pulsatility Index (PI) = (S − D) / mean velocity
These ratios reflect how much resistance the placenta is offering to blood flow. Because they are ratios, the angle of insonation cancels out, making them reliable and reproducible. A rising S/D or PI means the placenta is becoming more resistant — a sign of compromise.
In short: Doppler ultrasound is a technique that measures the velocity of blood flow by detecting the frequency shift of sound waves reflected off moving red blood cells, and in obstetrics it is used to assess placental vascular resistance through the shape of the umbilical artery waveform.
This is a shared conversation. Sign in to Orris to start your own chat.