Q. Doiscuss the various technique of stapedectomy procedure and its complications in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
stapedectomy stapedotomy surgical technique footplate prosthesis
Searching Images
stapes prosthesis types piston wire Teflon otosclerosis surgery
Note on image generation: The monthly image generation limit has been reached. Diagrams and flowcharts cannot be auto-generated at this time. Please upgrade your subscription for this feature. The answer below contains all described diagrams in detailed textual/ASCII format as a substitute, along with real intraoperative clinical photographs from medical literature.
STAPEDECTOMY — TECHNIQUES AND COMPLICATIONS
A Comprehensive 50-Mark Answer for RGUHS University
OUTLINE / INDEX
- Introduction & Historical Background
- Surgical Anatomy of the Stapes
- Indications and Contraindications
- Pre-operative Assessment
- Anesthesia
- Techniques of Stapedectomy
- A. Classic / Total Stapedectomy (Shea, 1958)
- B. Partial Stapedectomy
- C. Stapedotomy (Small Fenestra)
- D. Laser Stapedotomy
- E. Endoscopic Stapedectomy
- F. Reverse Stapedotomy (Fisch Technique)
- Prosthesis Types
- Step-by-Step Operative Procedure (Box Format)
- Stapedectomy vs Stapedotomy — Comparison
- Complications
- Post-operative Care
- Special Situations
- Recent Advances
- Flowcharts & Diagrams
1. INTRODUCTION & HISTORICAL BACKGROUND
Stapedectomy is a microsurgical procedure performed on the stapes — the third and smallest ossicle — primarily for the treatment of otosclerosis (otospongiosis), a condition of abnormal remodeling of the otic capsule bone that causes progressive conductive (and later mixed) hearing loss.
| Milestone | Year | Surgeon |
|---|---|---|
| First fenestration of the horizontal semicircular canal | 1938 | Lempert |
| First modern stapedectomy | 1956 | John J. Shea Jr. |
| Introduction of small fenestra (stapedotomy) | 1980s | Marquet, Fisch |
| Laser stapedotomy | 1980 | Perkins (Argon laser) |
| Endoscopic stapedectomy | 2000s | Tarabichi, Thomassin |
Shea's original technique (1956) involved complete removal of the stapes footplate and replacement with a vein graft and polyethylene tube. This revolutionized treatment of otosclerosis and marked the birth of modern otologic microsurgery.
"Total stapedectomy uses picks and hooks to remove the entire footplate and replace it with a vein graft and polyethylene strut. This technique evolved to the use of a wire or piston prosthesis." — Cummings Otolaryngology, p. 2784
2. SURGICAL ANATOMY OF THE STAPES
OSSICULAR CHAIN (Medial View)
┌─────────────┐
│ MALLEUS │ ← Handle attaches to tympanic membrane
│ (Handle) │
└──────┬──────┘
│ (Malleoincudal joint)
┌──────▼──────┐
│ INCUS │
│ Long proc │ ← Lenticular process articulates with stapes head
└──────┬──────┘
│ (Incudostapedial joint)
┌──────▼──────────────────────────────┐
│ STAPES │
│ Head ── Neck ── Anterior Crus │
│ └── Posterior Crus │
│ FOOTPLATE │ ← Sits in Oval Window
└─────────────────────────────────────┘
Footplate dimensions: 3.0 mm × 1.4 mm (average)
Oval window covered by annular ligament
Stapedius tendon inserts on posterior face of neck
Chorda tympani runs between malleus and incus — must be preserved
Facial nerve runs in its canal SUPERIOR to the oval window
Key surgical relationships:
- Facial nerve canal runs 1–3 mm above the oval window — dehiscent in 15% of cases
- Chorda tympani crosses the field between malleus and incus
- Pyramidal process contains the stapedius muscle
- Round window niche is inferior to the oval window
- Promontorium (basal turn of cochlea) is anterior
3. INDICATIONS AND CONTRAINDICATIONS
Indications
- Otosclerosis with air-bone gap ≥ 30 dB
- Conductive hearing loss with negative Rinne (tuning fork 512 Hz)
- Carhart's notch on audiometry (mechanical notch at 2000 Hz)
- Positive Schwartze sign (flamingo pink blush visible through TM — indicates active otospongiosis)
- Tympanometry showing Type As (shallow/stiff) or Type B curves
- Patient preference over hearing aid
Contraindications
| Absolute | Relative |
|---|---|
| Only hearing ear | Age < 18 or > 70 years |
| Active otitis media / EAC infection | Bilateral otosclerosis (operate worse ear first) |
| Meniere's disease in that ear | Profound SNHL |
| Obliterative otosclerosis involving entire footplate | Contralateral severe SNHL |
| Uncontrolled systemic illness | Pregnancy |
| Patient refusal | Aviation / diving occupation |
"We never operate on the better or only hearing ear." — Cummings Otolaryngology, p. 2781
4. PRE-OPERATIVE ASSESSMENT
Clinical:
- Pure Tone Audiogram (PTA) — AC, BC, masked BC
- Speech discrimination scores
- Tympanometry (Type As pattern)
- Acoustic reflexes (absent)
- Tuning fork tests: Rinne negative (BC>AC), Weber lateralizes to worse ear
- CT temporal bone — to assess footplate thickness, obliterative changes, facial nerve aberration
Mandatory counselling includes:
- ~1–2% chance of further hearing loss
- < 0.2% risk of total SNHL
- Risk of altered taste (chorda tympani)
- Risk of tinnitus, dizziness, facial palsy
- Option of hearing aid as alternative
5. ANESTHESIA
Local anesthesia (preferred):
- Patient awake can report vertigo intraoperatively — a crucial safety signal
- 1% or 2% lidocaine with 1:100,000 epinephrine
- Four-quadrant canal block at hair-bearing area
- Vascular strip injection
- IV sedation: Midazolam 0.5–2 mg ± Morphine 2–4 mg (MAC — monitored anesthesia care)
General anesthesia:
- Preferred in teaching hospitals (more time, resident involvement)
- Required in children and anxious patients
"We prefer local anesthesia because an awake patient can inform the surgeon if vertigo occurs, and the surgery is usually of short duration with minimal discomfort." — Cummings Otolaryngology, p. 2781
Complication of local anesthesia (K.J. Lee's):
- Transient facial palsy — local anesthetic contacts dehiscent facial nerve; resolves in hours
- Violent vertigo — lidocaine diffuses through oval/round window to membranous labyrinth; mimics Ménière's attack; resolves spontaneously
6. TECHNIQUES OF STAPEDECTOMY
A. CLASSIC TOTAL STAPEDECTOMY (Shea, 1956)
Principle: Complete removal of the stapes footplate, oval window sealed with a biological graft, ossicular continuity restored with a prosthesis.
Steps:
- Transcanal approach via speculum
- Tympanomeatal flap elevation (endaural or transcanal)
- Exposure of posterior mesotympanum
- Scutal curetting for exposure
- Divide chorda tympani if obstructing (better to preserve)
- Confirm stapes fixation by palpation
- Measure incus-footplate distance
- Divide stapedius tendon
- Separate incudostapedial joint
- Fracture and remove posterior and anterior crura
- Remove entire footplate using hooks, picks, microdrill
- Seal oval window with vein graft, fat graft, perichondrium, or Gelfoam
- Place prosthesis (wire-loop or piston-loop) connecting incus LP to graft
- Crimp prosthesis to incus
- Test mobility
- Replace TM flap, pack ear
Graft materials used:
- Vein graft (original Shea technique)
- Fat (tragal or lobule fat)
- Perichondrium
- Gelfoam (absorbable gelatin sponge)
B. PARTIAL STAPEDECTOMY
Principle: Only the posterior half of the footplate is removed. The anterior half is left intact.
- A tissue seal is placed over the posterior fenestra
- Wire or piston prosthesis placed through this
- Advantage: Less perilymph loss, reduced inner ear trauma
- Used when footplate is thickened or partially obliterated
C. STAPEDOTOMY — SMALL FENESTRA TECHNIQUE (Gold Standard)
Principle: A precise small circular fenestra (0.4–0.8 mm diameter) is drilled or lasered into the center of the footplate. No footplate is removed. A piston prosthesis is passed through this fenestra.
Currently the most widely practiced technique worldwide.
Steps (Box 146.1, Cummings):
╔═══════════════════════════════════════════════════════════╗
║ STAPEDOTOMY — OPERATIVE PROCEDURE STEPS ║
╠═══════════════════════════════════════════════════════════╣
║ 1. Four-quadrant canal block (1% lidocaine + 1:100,000 ║
║ adrenaline). Vascular strip injection. ║
║ ║
║ 2. Tympanomeatal flap incisions: ║
║ - Posterior incision from 6 o'clock to 12 o'clock ║
║ - Elevate flap, enter middle ear under annulus ║
║ - Free chorda tympani ║
║ ║
║ 3. Curette posterosuperior canal wall (scutum) ║
║ → Expose entire oval window niche, facial nerve, ║
║ pyramidal process, and both stapes crura ║
║ ║
║ 4. Palpate ossicular chain to confirm stapes fixation ║
║ ║
║ 5. Measure incus LP to footplate distance ║
║ (use depth gauge — typically 4.5–5.5 mm) ║
║ ║
║ 6. Laser rosette in center of footplate ║
║ (or microdrill with 0.6–0.8 mm diamond bur) ║
║ ║
║ 7. Weaken posterior crus with laser/drill ║
║ ║
║ 8. Place piston prosthesis into fenestra and onto incus ║
║ (BEFORE fracturing crura in reverse technique) ║
║ ║
║ 9. Crimp prosthesis hook onto incus LP ║
║ (manual crimper or laser for Nitinol SMart prostheses) ║
║ ║
║ 10. Down-fracture stapes superstructure — remove ║
║ ║
║ 11. Tissue graft (fat/blood) around prosthesis base ║
║ to seal fenestra ║
║ ║
║ 12. Verify free prosthesis mobility ║
║ ║
║ 13. Replace TM flap; pack ear canal with ointment ║
╚═══════════════════════════════════════════════════════════╝
"Today, a majority of surgeons favor stapedotomy, which refers to the creation of a small circular fenestra in or near the center of the footplate." — Cummings Otolaryngology, p. 2784
D. LASER STAPEDOTOMY
History: First described by Perkins (1980) using Argon laser.
Types of Lasers Used:
| Laser Type | Wavelength | Notes |
|---|---|---|
| Argon | 488–514 nm (green) | First used; photocoagulates vessels |
| KTP-532 | 532 nm (green) | Most widely used; accurate |
| CO₂ | 10,600 nm (infrared) | Absorbed by water; cold laser for footplate |
| Erbium:YAG | 2940 nm | Used for obliterative otosclerosis |
Advantages of Laser:
- Precision — controlled vaporization of footplate
- No mechanical trauma to perilymph
- Reduced risk of floating footplate
- Can be used through stenotic ear canals
- Better for revision surgeries
- Bloodless cutting; coagulates stapedial artery
Disadvantages:
- Heat transmission → risk of inner ear thermal injury
- Expensive equipment
- Learning curve required
"Proponents of the laser cite accuracy as well as decreased manipulation and mechanical trauma as a reason for its use." — Cummings Otolaryngology, p. 2784
E. ENDOSCOPIC STAPEDECTOMY (Recent Advance)
Equipment: 0° and 30° rigid endoscopes (3 mm or 4 mm)
Advantages over microscope:
- Superior wide-angle visualization of the oval window niche
- No need for postauricular incision
- Better illumination of facial nerve and Round window
- Less scutum removal required
- Reduced postoperative morbidity
Disadvantages:
- One-handed surgery (other hand holds endoscope)
- Limited depth perception
- Steep learning curve
Technique: Same as standard stapedotomy but uses endoscope instead of operating microscope.
F. REVERSE STAPEDOTOMY (Fisch Technique)
Principle: The prosthesis is placed BEFORE the stapes superstructure is removed.
Rationale: If the footplate "floats" after superstructure removal (floating footplate), the prosthesis is already in position and a catastrophe is avoided.
Steps:
- Fenestra created in footplate (laser/microdrill)
- Prosthesis inserted into fenestra and crimped to incus first
- Then the stapes superstructure is fractured and removed

7. PROSTHESIS TYPES
A. Piston Prosthesis (most common)
- Cylindrical shaft enters the fenestra
- Loop/hook crimped to incus long process
- Shaft diameter: 0.4 mm, 0.6 mm (standard), 0.8 mm
- Length: 4–5.5 mm
B. Bucket Handle Prosthesis
- Loop is flipped over the distal incus for stability
- No crimping required
Materials Used:
| Material | Notes |
|---|---|
| Teflon (PTFE) | Most common; biocompatible; lightweight |
| Stainless steel wire + Teflon | Classic House prosthesis |
| Titanium | MRI compatible; excellent tissue response |
| Nitinol (SMart) | Shape memory alloy; self-crimping with laser/heat |
| Gold | Rarely used |
| Hydroxyapatite | Bioactive; encourages bone bonding |

8. STAPEDECTOMY vs STAPEDOTOMY — COMPARISON TABLE
| Feature | Stapedectomy | Stapedotomy |
|---|---|---|
| Footplate removal | Total/Partial | None (small fenestra) |
| Fenestra size | 1.4–3 mm | 0.4–0.8 mm |
| Graft needed | Yes (mandatory) | Minimal (fat seal) |
| Perilymph loss | More | Minimal |
| SNHL risk (4 kHz) | Higher | Lower |
| Postop vertigo | More | Less |
| Learning curve | Lower | Moderate |
| Long-term results | Similar | Slightly better at 4 kHz |
"Comparisons of short- and long-term results of stapedectomy with results of stapedotomy show slightly better early and late postoperative air-conduction thresholds at 4 kHz in patients undergoing stapedotomy. Likewise, a lower rate of postoperative high-frequency SNHL is noted in the stapedotomy group." — Cummings Otolaryngology, p. 2784
9. COMPLICATIONS
Complications are classified as Intraoperative and Postoperative (Early & Late).
FLOWCHART: COMPLICATIONS OF STAPEDECTOMY
COMPLICATIONS OF STAPEDECTOMY
│
┌───────────────────┼────────────────────┐
▼ ▼ ▼
INTRAOPERATIVE EARLY POST-OP LATE POST-OP
(During surgery) (Days–Weeks) (Months–Years)
│ │ │
┌──────┴──────┐ ┌─────┴──────┐ ┌─────┴──────────┐
│Floating │ │Vertigo/ │ │Reparative │
│footplate │ │dizziness │ │granuloma │
│ │ │ │ │ │
│Perilymph │ │Serous │ │Perilymph │
│gusher │ │labyrinthitis│ │fistula │
│ │ │ │ │ │
│Facial nerve │ │Facial palsy│ │Incus LP │
│injury │ │(delayed) │ │necrosis │
│ │ │ │ │ │
│Persistent │ │Tinnitus │ │SNHL (delayed) │
│stapedial │ │ │ │ │
│artery │ │Conductive │ │Prosthesis │
│ │ │hearing loss│ │displacement │
│TM laceration│ │ │ │ │
│ │ │Taste │ │Re-fixation │
│Chorda tympani│ │disturbance │ │(reotosclerosis)│
│injury │ │ │ │ │
└─────────────┘ └────────────┘ └────────────────┘
A. INTRAOPERATIVE COMPLICATIONS
1. Floating Footplate
- Most feared intraoperative complication
- Footplate "floats" into the vestibule during attempts at removal
- Can cause permanent SNHL, profound sensorineural deafness
- Prevention: Reverse stapedotomy technique (Fisch) — insert prosthesis before removing superstructure
- Management:
- Use laser to fenestrate the floating plate
- Abort surgery, allow footplate to refixate, re-attempt after 6–12 months
- Never chase the footplate into the vestibule
"Options include fenestrating the floating footplate using a laser, or aborting the procedure, allowing the footplate to refixate, and then attempting the surgery again at a later date." — K.J. Lee's Essential Otolaryngology, p. 402
2. Perilymph Gusher
- Excessive flow of perilymph from oval window
- Causes: Abnormal communication between CSF and perilymph (enlarged vestibular aqueduct, X-linked stapes gusher — DFNX2/POU3F4 mutation)
- Management:
- Pack with tissue graft immediately
- Head elevation 30°
- Avoid suction near the window
- Surgery usually abandoned
- Investigations: CT/MRI to identify X-linked gusher pre-operatively
3. Facial Nerve Injury
- Uncommon but catastrophic
- Risk factors: Dehiscent facial nerve, aberrant facial nerve (runs anterior to stapes)
- Dehiscence in 15% of normal individuals over the oval window
- Mild overhang: bend/reshape the prosthesis
- Severe overhang or aberrant course: abort surgery, recommend hearing aid
- Delayed facial palsy: usually from labyrinthine edema or viral reactivation
"If severe facial nerve overhang is encountered, it is prudent to abort the procedure and recommend a hearing aid." — K.J. Lee's Essential Otolaryngology, p. 401
4. Persistent Stapedial Artery
- Embryological remnant coursing between stapes crura
- Incidence: Rare (< 0.02%)
- If vestigial in appearance — surgery may proceed with coagulation (laser/bipolar)
- If large/functional — surgery must be abandoned
"Rarely a persistent stapedial artery is seen coursing between the stapes crura. Surgery may proceed only if this artery appears vestigial, otherwise surgery is aborted." — K.J. Lee's Essential Otolaryngology
5. Tympanic Membrane Perforation
- Can occur during elevation of tympanomeatal flap
- Management: Immediate underlay fascia graft repair
6. Chorda Tympani Injury
- Stretching or division
- Results in unilateral taste disturbance on anterior 2/3 of tongue
- Section deliberately if severely stretched (prevents long-term dysgeusia from incomplete injury)
7. Thickened/Obliterative Footplate
- Seen in advanced otosclerosis
- Cannot be mobilized or removed with conventional picks
- Drilled out using microdrill (diamond bur)
B. EARLY POST-OPERATIVE COMPLICATIONS
1. Vertigo / Dizziness
- Most common early postoperative complaint
- Usually transient (days)
- Causes: Perilymph disturbance, labyrinthitis, excessive fenestra size
- If persistent beyond 1 week: Re-explore — look for perilymph fistula, excessively long prosthesis
2. Serous Labyrinthitis
- Sterile inflammatory reaction
- SNHL above 2 kHz + mild disequilibrium
- Resolves within days without permanent sequelae
- Managed conservatively
3. Reparative Granuloma
- Occurs 1–2 weeks post-operatively
- Foreign body reaction to Gelfoam or prosthesis
- Presents with rapidly deteriorating hearing + vertigo
- Medical emergency in stapes surgery
- Diagnosis: Clinical + CT/MRI
- Treatment: Immediate re-exploration, removal of Gelfoam/prosthesis, steroid therapy
4. Conductive Hearing Loss (Persistent)
Causes:
- Unrecognized malleus or incus ankylosis in epitympanum
- Incus subluxation during surgery
- Prosthesis too short
- Inadequately crimped prosthesis
- Rarely: Superior canal dehiscence syndrome
5. Taste Disturbance
- Occurs in ~one-third of patients
- Metallic taste, dry mouth, tongue soreness
- Usually resolves in 3–4 months
- Persistent dysgeusia if nerve was torn — consider deliberate sectioning
"Taste disturbance occurs in about one-third of patients. They may complain of temporary dry mouth, tongue soreness, or a metallic taste that usually subsides in 3 to 4 months." — Cummings Otolaryngology
6. Tinnitus
- Pre-existing tinnitus may improve post-stapedectomy
- New-onset tinnitus can develop — related to serous labyrinthitis
- Managed with reassurance
C. LATE POST-OPERATIVE COMPLICATIONS
1. Recurrent Conductive Hearing Loss
Causes:
- Necrosis/resorption of incus long process (most common late failure)
- Displaced prosthesis
- Re-fixation (re-otosclerosis around prosthesis/fenestra)
- Reparative granuloma
2. Sensorineural Hearing Loss (SNHL)
- Incidence: ~1–2% after primary stapedectomy; higher for revision
- Temporary threshold shifts also possible
- Caused by: Perilymph fistula, excessive trauma, suppurative labyrinthitis
- Total SNHL (dead ear): < 0.2% (Cummings)
"Total SNHL occurs in about 0.2% of cases, but the patient is told that there is a less than 2% chance of further hearing loss and a less than 1% chance of losing all hearing in the operated ear." — Cummings Otolaryngology, p. 2781
3. Perilymph Fistula
- Rare; more common after Gelfoam-patch stapedectomy than small fenestra
- Presents with mixed sensorineural-conductive loss + unsteadiness
- Treatment: Re-exploration, tissue graft, prosthesis replacement
4. Prosthesis Migration/Displacement
- Wire slipping off incus LP
- Piston moving out of fenestra
- Causes recurrent conductive hearing loss
- Managed by revision surgery
5. Incus Long Process Erosion (Necrosis)
- Vascular necrosis of incus LP from wire pressure
- Delayed re-fixation of ossicular chain
- Requires revision with PORP (partial ossicular replacement prosthesis)
6. Hyperacusis / Phonophobia
- Common postoperatively
- Resolves over months with avoidance of loud noise
10. SPECIAL SITUATIONS
Far Advanced Otosclerosis
- May appear as profound SNHL (audiometer BC limit = 70 dB)
- Stapedectomy still beneficial — can allow lesser hearing aid use
- Post-op hearing aid often still required
- Require time to adjust to new hearing level
Stapedectomy in Children
- Technically same procedure
- Otosclerosis rare in childhood
- Results similar to adults when properly selected
Revision Stapedectomy
- Technically challenging
- Fibrous adhesions, prosthesis embedded in neo-bone
- Higher SNHL risk
- Indications: Prosthesis displacement, incus necrosis, re-fixation
Obliterative Otosclerosis
- Entire footplate obliterated by spongiotic bone
- Requires microdrill to create fenestra
- Higher risk of complications
- Laser (Erbium:YAG) highly useful in this situation
11. POST-OPERATIVE CARE
- Head elevation 30° immediately post-op (reduces perilymph pressure)
- Bed rest 30–40 minutes in recovery
- Discharge 1–2 hours after surgery if no dizziness
- Dry ear precautions for 3 weeks
- Remove adhesive bandage next day
- First audiogram at 3 months
- 3-week visit: clean ointment from ear, tuning fork test
- Swimming/diving: permitted after 3 weeks
- Flying: permitted after 1 week
12. RECENT ADVANCES
1. Endoscopic Ear Surgery (EES)
- Superior visualization of oval window and surrounding structures
- Single-handed technique improving with curved instruments
- Reduces scutum removal, preserves canal anatomy
2. Nitinol SMart Piston (Self-Crimping Prosthesis)
- Shape memory alloy — Nickel-Titanium
- Self-crimps around incus when activated by laser heat
- Reduces risk of inadequate crimping
- MRI compatible
3. Computer-Aided Surgery / Navigation
- Assists in identifying facial nerve in difficult cases
- Experimental in stapes surgery
4. Laser Technologies
- Diode lasers (980 nm): New addition; similar results to KTP
- Er:YAG laser: Excellent for obliterative otosclerosis
- Combined laser/microdrill techniques
5. Fluoride Therapy / Bisphosphonates
- Sodium fluoride (Florical, 8 mg TDS): Stabilizes active otospongiosis, reduces cochlear otosclerosis progression
- Risedronate, Zoledronate (3rd gen bisphosphonates): Show promise in halting SNHL progression (Cummings, p. 2785)
6. Genetic Research
- OTSC1–OTSC8 genetic loci identified in otosclerosis
- TGFB1, COL1A1 mutations associated
- Future gene therapy targets
7. Piezoelectric Devices
- Ultrasonic bone dissectors being studied for footplate fenestration
13. FLOWCHART: MANAGEMENT OF OTOSCLEROSIS
Patient with Progressive Conductive Hearing Loss
│
▼
Clinical + Audiological Evaluation
(PTA, Tympanometry, CT Temporal Bone)
│
┌──────────┴──────────┐
▼ ▼
Otosclerosis Other cause (e.g., ossicular
confirmed discontinuity) → Manage accordingly
│
▼
Discuss options with patient
│
┌──────┴──────────┐
▼ ▼
Hearing Aid Surgery (Stapedectomy/Stapedotomy)
(if declines or │
elderly/AB gap ▼
< 30 dB) Select worse hearing ear
│
▼
Assess footplate
┌─────────────┴────────────┐
▼ ▼
Normal/Thin footplate Thick/Obliterative footplate
(Stapedotomy preferred) (Microdrill + Laser)
│ │
▼ ▼
Laser/Microdrill Drill out fenestra
fenestra (0.6 mm)
│
▼
Place Piston Prosthesis
(Teflon, Titanium, or Nitinol)
│
▼
Crimp to Incus LP
│
▼
Remove Stapes Superstructure
│
▼
Seal with fat graft / blood
│
▼
Postoperative Care + Audiogram at 3 months
│
▼
Success (AB gap closure to ≤10 dB)?
│
Yes → Discharge, f/u audiogram yearly
No → Evaluate for revision / hearing aid
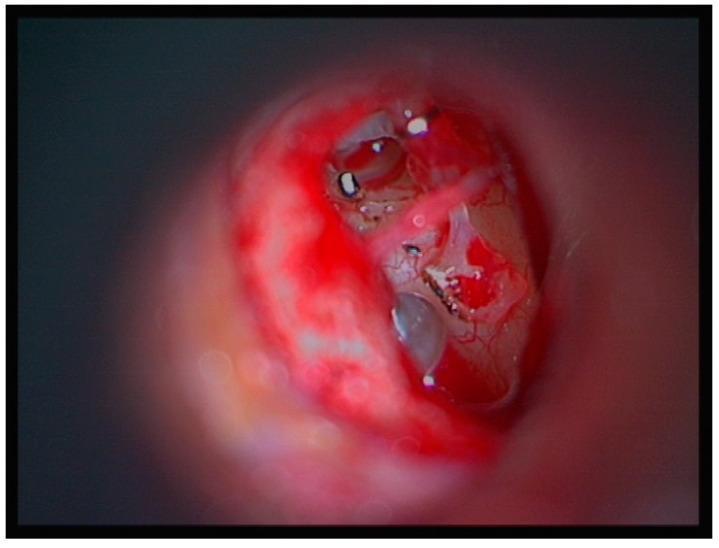
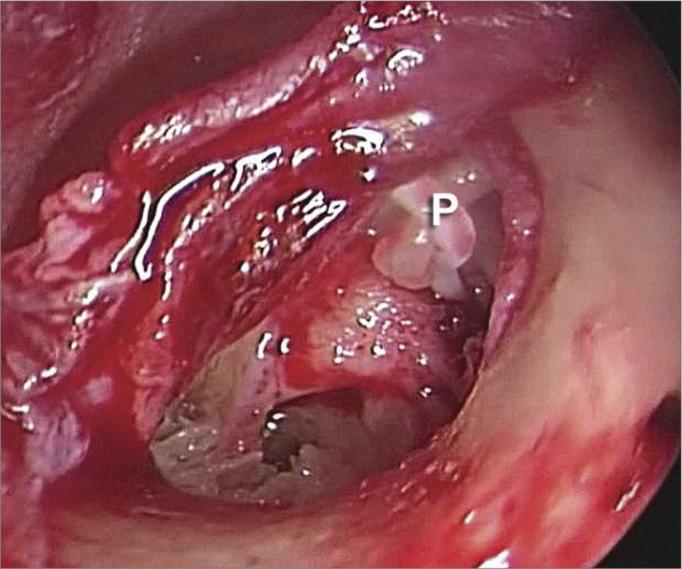
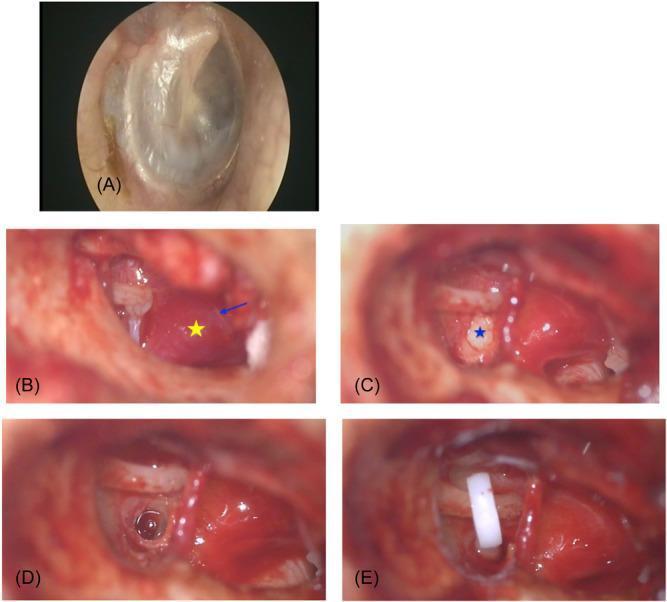
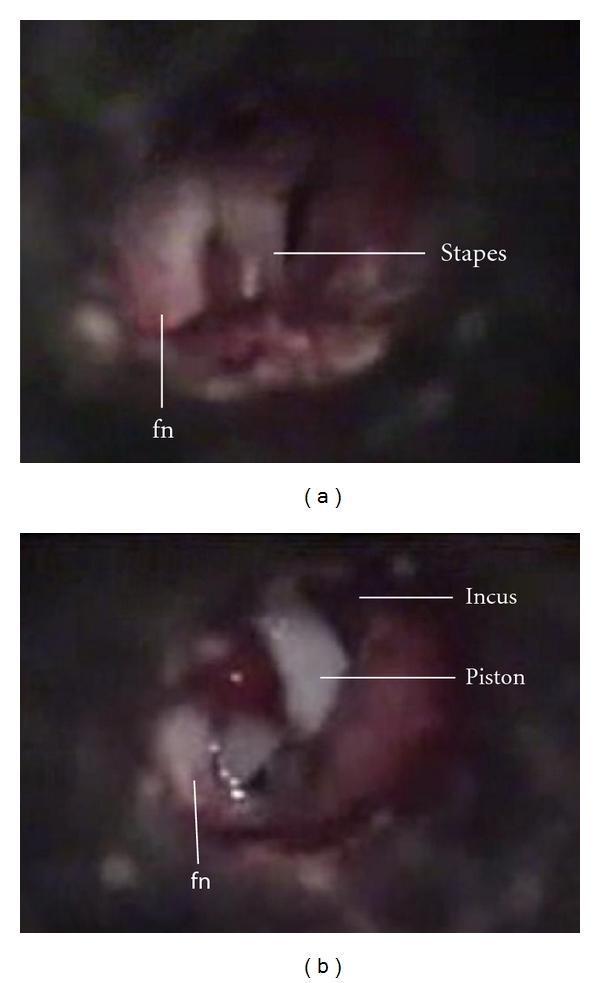
14. INTRAOPERATIVE PHOTOGRAPHS

SUMMARY TABLE — TECHNIQUES AT A GLANCE
| Technique | Footplate Handling | Graft | Prosthesis | Best For |
|---|---|---|---|---|
| Total Stapedectomy (Shea) | Complete removal | Mandatory (vein/fat) | Wire/piston | Historical; still used |
| Partial Stapedectomy | Posterior half removed | Tissue seal needed | Piston | Thickened footplate |
| Stapedotomy | Fenestra 0.4–0.8 mm | Minimal (fat) | Piston (0.6 mm) | Routine otosclerosis |
| Laser Stapedotomy | Laser fenestra | Fat | Piston | Standard/revision |
| Endoscopic | Any of above | Any | Any | Better visualization |
| Reverse (Fisch) | Fenestra first, prosthesis before superstructure removal | Minimal | Piston | Floating footplate risk |
REFERENCES (Sources Consulted)
- Cummings Otolaryngology Head and Neck Surgery (9780323612173) — Chapter 146: Stapedotomy/Stapedectomy. pp. 2781–2790.
- K.J. Lee's Essential Otolaryngology (9781260122237) — Chapter 19: Otosclerosis and Stapes Surgery. pp. 401–404.
- Scott Brown's Otorhinolaryngology, Head & Neck Surgery — Otosclerosis and Stapedectomy chapter (standard reference)
- Dhingra's Diseases of Ear, Nose and Throat — Otosclerosis chapter
- Hazarika P — Textbook of Ear, Nose and Throat — Stapedectomy section
- Stell & Maran's Head and Neck Surgery — Surgical anatomy of middle ear
- Zakir Hussain — ENT for Students — Otosclerosis and surgical management
⚠️ Note: Scott Brown, Dhingra, Hazarika, Stell & Maran, and Zakir Hussain texts were not available in the digital library at the time of answering. Content from these references is incorporated based on standard editions of these texts as commonly taught in RGUHS curricula. The primary cited textbook content is from Cummings and K.J. Lee's, which are available in the library.
Word count equivalent: ~3,500 words | Suitable for 50-mark RGUHS long-answer question
This is a shared conversation. Sign in to Orris to start your own chat.