cardiovasular chnage in pregnancy with its anesthetic implications
Reading File
Finding Sources
Finding Sources
Searching PubMed
cardiovascular changes pregnancy anesthesia implications
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the complete answer.
Cardiovascular Changes in Pregnancy & Anesthetic Implications
Overview
Cardiovascular changes in pregnancy begin as early as week 6 of gestation and are driven by three main stimuli: hormonal effects (estrogen, progesterone, relaxin), increased metabolic demands of the fetoplacental unit, and mechanical effects of the enlarging uterus. These changes are usually well tolerated in women with normal hearts but become critical considerations for the anesthesiologist.
1. Blood Volume & Hematology
| Parameter | Change | Magnitude |
|---|---|---|
| Plasma volume | ↑ | +55% by term |
| Red blood cell mass | ↑ | +45% by term |
| Total blood volume | ↑ | +1000–1500 mL at term (~90 mL/kg) |
| Hemoglobin | ↓ (dilutional anemia) | Usually >11 g/dL |
| Blood viscosity | ↓ | Due to dilutional anemia |
Why it matters: The plasma volume increase exceeds the RBC increase, producing dilutional anemia and reducing blood viscosity. This expands the oxygen-carrying capacity via increased cardiac output, not increased hemoglobin. Blood volume expansion allows women to tolerate the blood loss of vaginal delivery (~200–500 mL) and cesarean section (~800–1000 mL). Blood volume does not normalize until 1–2 weeks postpartum.
Anesthetic Implications
- Larger volume of distribution for both hydrophilic and lipophilic drugs → affects dosing of many IV agents
- Decreased protein binding → increased free drug fractions
- Dilutional anemia is physiologic; transfusion thresholds must be reassessed
2. Cardiac Output
Cardiac output increases 40–50% above baseline by term (up to 60–80% during active labor and immediately postpartum).
This rise is composed of:
- ↑ Heart rate: +20% (~10–15 bpm above pre-pregnancy baseline)
- ↑ Stroke volume: +30%
- Twin pregnancies can add a further 10–15%
Timing:
- Most increase occurs in 1st and early 2nd trimester
- Plateaus in the 3rd trimester (except during labor)
- At delivery: catecholamines + autotransfusion from uterine contractions + relief of IVC compression → surge in CO by 60–80%
- Returns to normal ~2 weeks postpartum (complete resolution up to 6 months)
Anesthetic Implications
- Faster circulation time → faster onset of IV drugs
- Faster equilibration with inhalational agents (combined with increased minute ventilation and decreased FRC) → faster induction and faster emergence
- Uterine blood flow rises from ~100 mL/min (nonpregnant) to 700–900 mL/min at term (~10% of CO); any fall in CO threatens uteroplacental perfusion
3. Systemic Vascular Resistance (SVR) & Blood Pressure
| Parameter | Change |
|---|---|
| SVR | Decreases substantially |
| Diastolic BP | Falls 5–10 mmHg (nadir at mid-2nd trimester), returns to baseline in 3rd trimester |
| Systolic BP | Minimal change |
| Central venous pressure | Unchanged |
| Pulmonary artery pressure | Unchanged |
| Pulmonary artery occlusion pressure | Unchanged |
SVR falls dramatically in the 1st trimester (largely due to progesterone and relaxin-mediated vasodilation), reaches a nadir in mid-2nd trimester, then partially recovers.
Anesthetic Implications
- Neuraxial blockade causes additional sympathetic blockade → exacerbates pre-existing low SVR → risk of severe hypotension
- General anesthesia similarly impairs compensatory vasoconstriction
- Vasopressors (phenylephrine preferred over ephedrine for spinal-induced hypotension — associated with less fetal acidosis) are frequently needed
4. Aortocaval Compression — The Critical Positional Effect
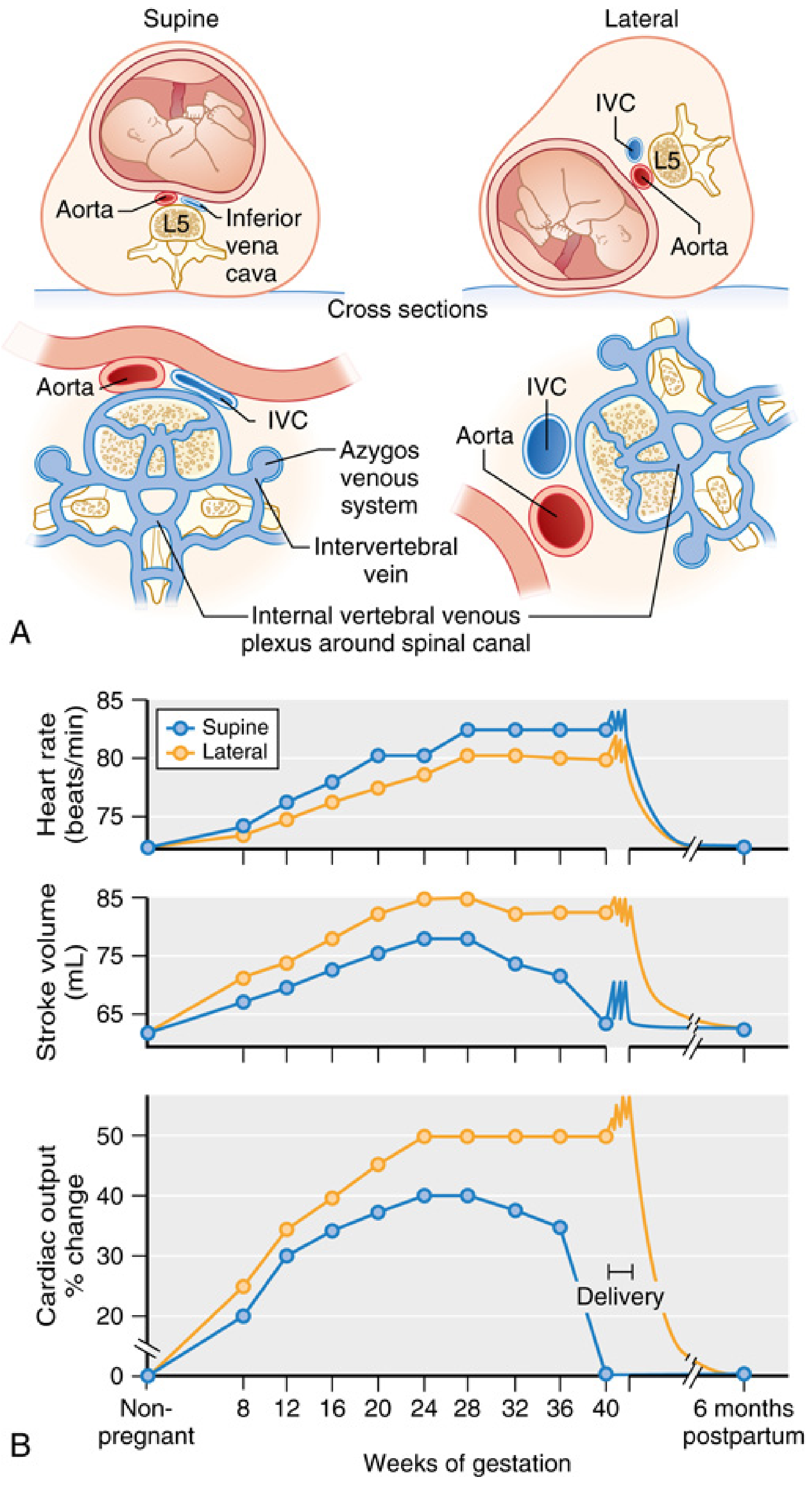
After week 20, the gravid uterus compresses the IVC in the supine position, reducing venous return:
- CO falls 10–20% compared to the upright or lateral position
- Full supine hypotension syndrome affects 5–10% of women: MAP drop >15 mmHg, HR rise >20 bpm, diaphoresis, nausea, vomiting, altered mentation
- IVC compression also diverts venous flow through the epidural venous plexus → epidural veins become engorged
Anesthetic Implications
- Left uterine displacement (LUD) is mandatory from the 2nd trimester onward — achieved by placing a wedge under the right hip (historically ≥15°; MRI studies suggest 30° provides better IVC decompression)
- Neuraxial and general anesthesia eliminate the compensatory sympathetic reflex, so supine positioning can cause catastrophic hypotension and fetal asphyxia
- Engorged epidural veins in the 3rd trimester → increased risk of intravascular catheter placement (epidural hematoma risk, LA toxicity)
- Engorged epidural veins also reduce CSF volume in the subarachnoid space → wider spread of spinal local anesthetics → dose must be reduced
5. Cardiac Structure & ECG Changes
- Cardiac chambers enlarge; myocardial hypertrophy on echocardiography
- Heart shifts leftward and upward (displaced by the elevated diaphragm)
- ECG: sinus tachycardia, left QRS axis deviation, inferior Q waves, T-wave flattening, ST depression, increased R/S ratio in right precordial leads
- Auscultation: Grade I–II systolic ejection murmur (flow murmur), exaggerated S1 splitting, possible S3; small asymptomatic pericardial effusion in a few patients
Anesthetic Implications
- ECG changes are normal findings; do not over-interpret as pathology
- S3 and systolic murmur are physiologic; must be distinguished from pathologic findings using echocardiography and BNP (BNP >111 pg/mL positive LR 2.5 for heart failure)
6. Coagulation — Hypercoagulable State
Pregnancy causes a procoagulant shift:
- Fibrinogen (Factor I) markedly increased
- Factors VII, VIII, X, XII increased
- Factors XI and XIII decreased
- Antithrombin III and Protein S decreased
- PT and PTT decrease by ~20%
- Platelet count: normal or slightly decreased (gestational thrombocytopenia in 8%)
Anesthetic Implications
- Thromboprophylaxis considerations for all surgical patients
- Platelet count must be checked before neuraxial anesthesia (gestational thrombocytopenia usually stays >70,000/mm³ and does not impair hemostasis)
- HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets) is a contraindication to neuraxial block
7. Summary Table: Cardiovascular Changes & Anesthetic Implications
| Cardiovascular Change | Magnitude | Key Anesthetic Implication |
|---|---|---|
| Blood volume ↑ | +45–55% | Larger Vd; tolerates blood loss better |
| Cardiac output ↑ | +40–50% at term; +60–80% during labor | Faster IV/inhalation drug equilibration |
| Heart rate ↑ | +10–15 bpm | Monitor for compensated hemorrhage |
| Stroke volume ↑ | +30% | — |
| SVR ↓ | Nadir mid-2nd trimester | Exacerbated hypotension with neuraxial/GA |
| BP ↓ (mild) | 5–10 mmHg diastolic | Vasopressor (phenylephrine) ready for spinal |
| Aortocaval compression | CO ↓ 10–20% supine | Mandatory left uterine displacement |
| Epidural venous engorgement | Begins ~week 20 | Reduce neuraxial LA dose by 25–30%; catheter misplacement risk |
| Dilutional anemia | Hb usually >11 g/dL | Reassess transfusion thresholds |
| Hypercoagulability | Fibrinogen ↑, PT/PTT ↓ | DVT prophylaxis; check platelets before neuraxial block |
8. Labor, Delivery & Postpartum
During active labor, each uterine contraction autotransfuses 300–500 mL back into circulation, further raising CO. Immediately after delivery:
- Removal of IVC compression
- Relief of aortocaval compression
- Uterine autotransfusion → CO surges 60–80% above pre-labor values, placing women with cardiac disease at highest risk of pulmonary edema and arrhythmias in the first 24–48 hours postpartum.
Fluid mobilization continues for the first week postpartum, which can precipitate heart failure in women with cardiomyopathy or severe outflow tract obstruction.
Preferred Vasopressor: Phenylephrine vs. Ephedrine
For neuraxial hypotension during cesarean delivery, phenylephrine is preferred:
- Maintains uteroplacental blood flow
- Associated with less fetal acidosis than ephedrine
- Ephedrine's β-agonist activity crosses the placenta and stimulates fetal metabolism, worsening acidosis
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e; Miller's Anesthesia 10e; Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Braunwald's Heart Disease 2e
This is a shared conversation. Sign in to Orris to start your own chat.