Q. Discuss in details the clinical features and management of lateral sinus thrombophlebitis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Note on image generation: The monthly plan limit for image generation has been reached. All diagrams and flowcharts below are presented in text/ASCII format. To access generated visual diagrams, please upgrade your subscription plan.
LATERAL SINUS THROMBOPHLEBITIS (OTOGENIC SIGMOID/LATERAL SINUS THROMBOSIS)
A Comprehensive Discussion for 50 Marks — RGUHS University
CONTENTS AT A GLANCE
- Introduction & Historical Note
- Anatomy of Lateral/Sigmoid Sinus
- Incidence & Etiology
- Pathology & Pathogenesis
- Clinical Features
- Griesinger's Sign & Other Special Signs
- Investigations
- Radiological Imaging (with Images)
- Diagnosis
- Complications
- Management — Medical & Surgical
- Flowchart of Management
- Recent Advances
- Prognosis
1. INTRODUCTION & HISTORICAL NOTE
Lateral sinus thrombophlebitis (LST), also known as otogenic sigmoid sinus thrombosis (SST) or otitic pyemia, is one of the most serious intracranial complications of otitis media and mastoiditis. It was a feared cause of death in the pre-antibiotic era. Sir Charles Symonds coined the term "otitic hydrocephalus" to describe the raised intracranial pressure associated with this condition. Griesinger (1857) described the characteristic postauricular edema (Griesinger's sign) from thrombophlebitis of the mastoid emissary vein.
In the modern antibiotic era, the incidence has drastically reduced, but the condition remains life-threatening when it occurs. The classic presentation is now frequently masked by prior antibiotic therapy, making diagnosis challenging.
2. ANATOMY OF THE LATERAL (SIGMOID) SINUS
The lateral sinus comprises two parts:
- Transverse sinus: runs horizontally in the tentorium cerebelli
- Sigmoid sinus: S-shaped continuation, runs in the posterior fossa → jugular bulb → internal jugular vein
Key Anatomical Relationships:
Superior Sagittal Sinus
↓
Transverse Sinus (horizontal part)
↓
Sigmoid Sinus (S-shaped, lies in sigmoid sulcus of mastoid bone)
↓ ← directly adjacent to mastoid air cells (KEY POINT)
Jugular Bulb
↓
Internal Jugular Vein (exits via jugular foramen)
The sigmoid sinus is separated from the mastoid air cells only by the bony sinus plate (dehiscent in many patients), making it uniquely vulnerable to otogenic infection.
Connections important in LST spread:
- Via inferior petrosal sinus → Cavernous sinus (anterior)
- Via superior petrosal sinus → Cavernous sinus
- Via mastoid emissary vein → Scalp veins (→ Griesinger's sign)
- Downward → Internal jugular vein → Septic emboli to lungs
3. INCIDENCE & ETIOLOGY
Incidence:
- Pre-antibiotic era: ~40% of otogenic intracranial complications
- Post-antibiotic era: Rare but still seen; incidence ~3–4% of otogenic intracranial complications
- More common in children and young adults
- Male:Female ratio — roughly equal
Etiology:
| Source | Proportion |
|---|---|
| Chronic suppurative otitis media (CSOM) with cholesteatoma | Most common (~70%) |
| Acute otitis media (AOM) with acute mastoiditis | ~25% |
| Coalescent mastoiditis | Common in children |
| Petrositis (Gradenigo syndrome) | Rare but recognized |
Causative Organisms:
- Streptococcus species (most common — esp. S. pyogenes, S. pneumoniae)
- Staphylococcus aureus (including MRSA)
- Proteus mirabilis
- Pseudomonas aeruginosa
- Bacteroides (anaerobes — in cholesteatoma)
- Mixed flora common
4. PATHOLOGY & PATHOGENESIS
Pathogenesis (Dhingra / Cummings):
CSOM / Acute Mastoiditis
↓
Perisinus Abscess Formation
(erosion of bony sinus plate by cholesteatoma / granulation tissue / pressure necrosis)
↓
Inflammation of Adventitia of Sigmoid Sinus Wall
↓
Penetration of Venous Wall (endophlebitis)
↓
Infection reaches Intima → Triggers Virchow's Triad
(Endothelial damage + stasis + hypercoagulability)
↓
Mural Thrombus Formation (infected thrombus)
↓
Enlargement → Occlusion of Sinus Lumen
↓
Propagation of Thrombus (in both directions)
↓ ↑
[Toward jugular vein / IJV] [Toward transverse sinus / SSS]
↓
Septicemia (shower of infected emboli)
↓
Septic Emboli → Metastatic Abscesses (lung, brain, joints)
— Cummings Otolaryngology Head and Neck Surgery, p. 2721
The perisinus abscess exerts pressure on the outer dural wall, causing necrosis extending to the intima, attracting fibrin, blood cells, and platelets. The infected clot frequently showers the bloodstream with bacteria, giving rise to septicemia and the possibility of metastatic abscesses, most commonly to the lungs.
In AOM (osteothrombophlebitis route):
The bony sinus plate remains intact; infection spreads via diploic veins (osteothrombophlebitis) — the sinus plate is intact at surgical exploration.
5. CLINICAL FEATURES
A. Symptoms
The classic triad (Adams & Victor; Cummings):
- Picket fence fever — diurnal temperature spikes exceeding 103°F (39.4°C), rigor-free intervals, characteristic of septicemia
- Headache — deep-seated, persistent, often occipital/temporal
- Otomastoiditis symptoms — ear discharge, otalgia, mastoid tenderness
⚠️ Modern presentation caveat (Cummings, p. 2523): In the antibiotic era, the classic picket fence fever is less common. Affected patients, particularly children, may present initially with diplopia or other neurological symptoms rather than the classic fever pattern.
Additional Symptoms:
- Neck pain and stiffness — from sternocleidomastoid (SCM) inflammation (perijugular involvement) — differentiated from meningism
- Malaise, anorexia, weight loss
- Vomiting
- Diplopia — from raised ICP → 6th nerve palsy
- Blurring of vision / visual obscurations — if otitic hydrocephalus develops
B. Signs
| Sign | Description | Source |
|---|---|---|
| Griesinger's Sign | Edema and tenderness over mastoid emissary vein area (postauricular) — due to thrombophlebitis of mastoid emissary vein | Dhingra; Hazarika |
| Tobey-Ayer Test (Queckenstedt Test modification) | LP done; compression of jugular vein on the normal side → rise in CSF pressure; compression on the affected side → no rise (sinus occluded) | Dhingra |
| Crowe-Beck Test | Auscultation over the contralateral eye with bell stethoscope; jugular vein compression on normal side → sound heard; compression on affected side → no sound | Dhingra |
| Papilledema | Due to raised ICP / otitic hydrocephalus | |
| Tender, swollen neck | Jugular vein thrombosis → cord of tenderness along IJV | |
| Cerebellar signs | Ataxia, nystagmus if cerebellar involvement (adjacent sigmoid sinus) | |
| Cranial nerve palsies | CN IX, X, XI — jugular foramen syndrome (Vernet's syndrome) if jugular bulb involved | Adams & Victor |
Fever Pattern:
Temperature (°F)
105 | * *
104 | * * * *
103 | * * * *
102 | * * *
101 | * *
|________________________________
Time (hours/days)
← "Picket Fence" Pattern (Septic spikes) →
This picket fence (hectic/intermittent) pattern occurs because fragments of infected thrombus are repeatedly shed into the bloodstream.
6. SPECIAL SIGNS IN DETAIL
Griesinger's Sign:
Oedema and tenderness over the posterior part of the mastoid, along the line of the mastoid emissary vein. It occurs because thrombophlebitis extends from the sigmoid sinus to the mastoid emissary vein, causing inflammation of the overlying soft tissues. Considered pathognomonic of LST by some textbooks.
Tobey-Ayer Test:
Performed during lumbar puncture. Compression of the jugular vein on the healthy side causes a rise in CSF pressure (normal Queckenstedt response). Compression on the diseased side produces no rise (blocked sinus). This is considered positive for LST. (Note: This test is now largely replaced by MR venography.)
7. INVESTIGATIONS
A. Blood Investigations:
- CBC: Leucocytosis (↑ WBC, neutrophilia), ↑ ESR, ↑ CRP
- Blood culture: May grow causative organism (especially during fever spikes/rigor)
- Coagulation profile: Baseline before anticoagulation
- LFT, KFT: Baseline organ function
B. Cerebrospinal Fluid (CSF) Analysis:
- Opening pressure: Elevated (due to otitic hydrocephalus)
- Cell count: Normal or mildly elevated (a few cells)
- Protein: Normal or mildly elevated
- Glucose: Normal
- Culture: Usually negative (unless associated meningitis)
- Tobey-Ayer test performed during LP
C. Imaging (Most Important)
1. CT Scan (Contrast-Enhanced Temporal Bone CT):
The "Delta sign" (Empty triangle sign / Empty delta sign):
On Axial CECT:
┌─────────────────────┐
│ Contrast-enhancing │
│ walls of sinus │ ← "Delta" shape (Δ)
│ with NON- │
│ enhancing clot │
│ in the CENTER │
└─────────────────────┘
= Classic "Empty Delta Sign" (Delta sign / Dark centre sign)
- Absent enhancement of the sigmoid sinus (compared to normal opposite side)
- Opacified mastoid air cells
- May show perisinus abscess
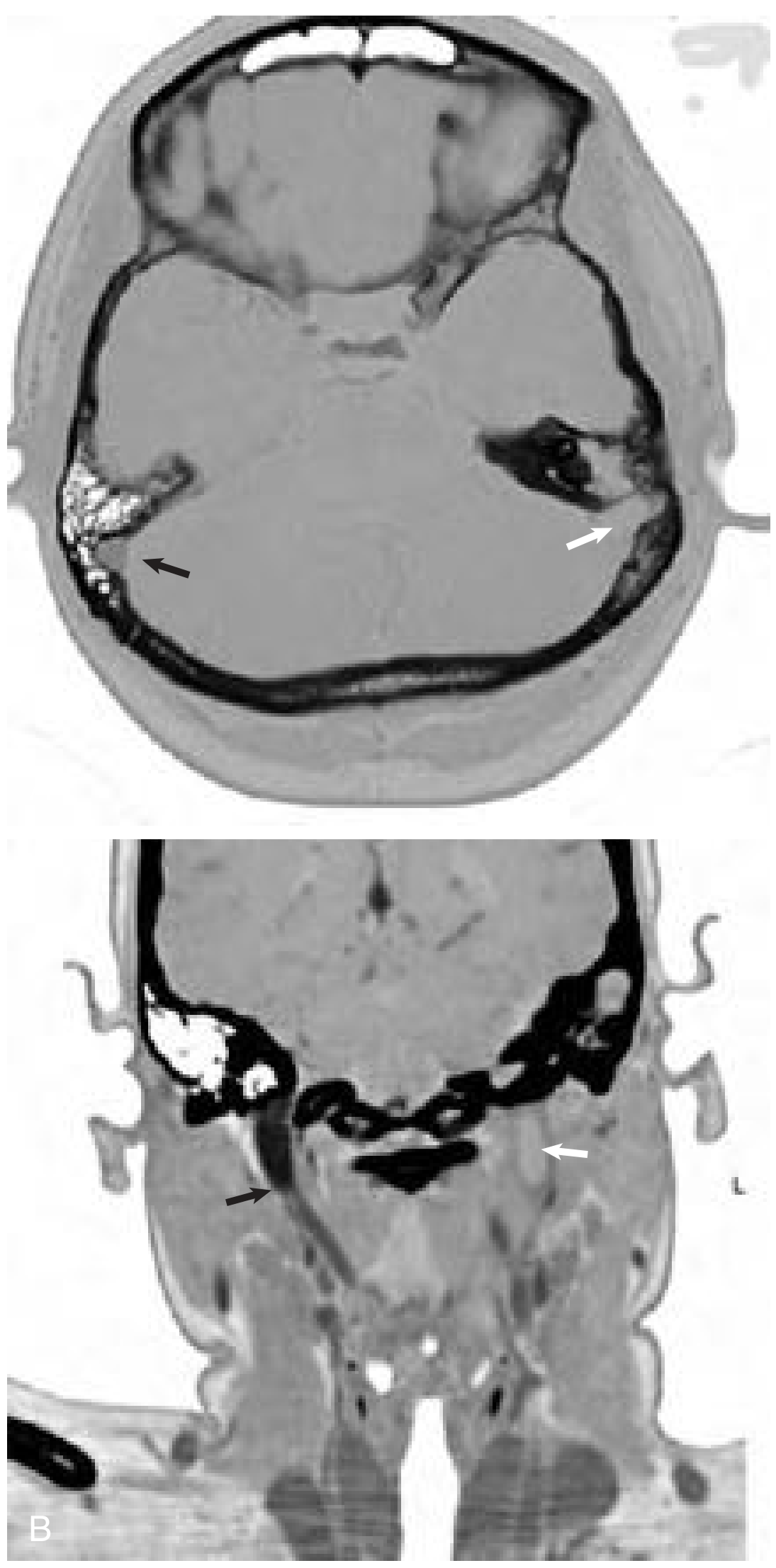
Fig: Axial enhanced temporal bone CT scan (A) shows absent enhancement of the left sigmoid sinus (white arrow) next to an opacified mastoid. Note the normal enhancement of the right sigmoid (black arrow). (B) Coronal contrast-enhanced CT shows absent flow in the left internal jugular vein at the skull base (white arrow). — Cummings Otolaryngology, p. 2721
2. MRI + MR Venography (Gold Standard):
- T1W: Isointense clot → bright on T1 (subacute thrombus due to methaemoglobin)
- T2W: Variable signal in thrombus
- MR Venography: Shows absence of flow / filling defect in sigmoid/transverse sinus (see below)
- Can detect associated complications: meningitis, cerebellar abscess, temporal lobe abscess
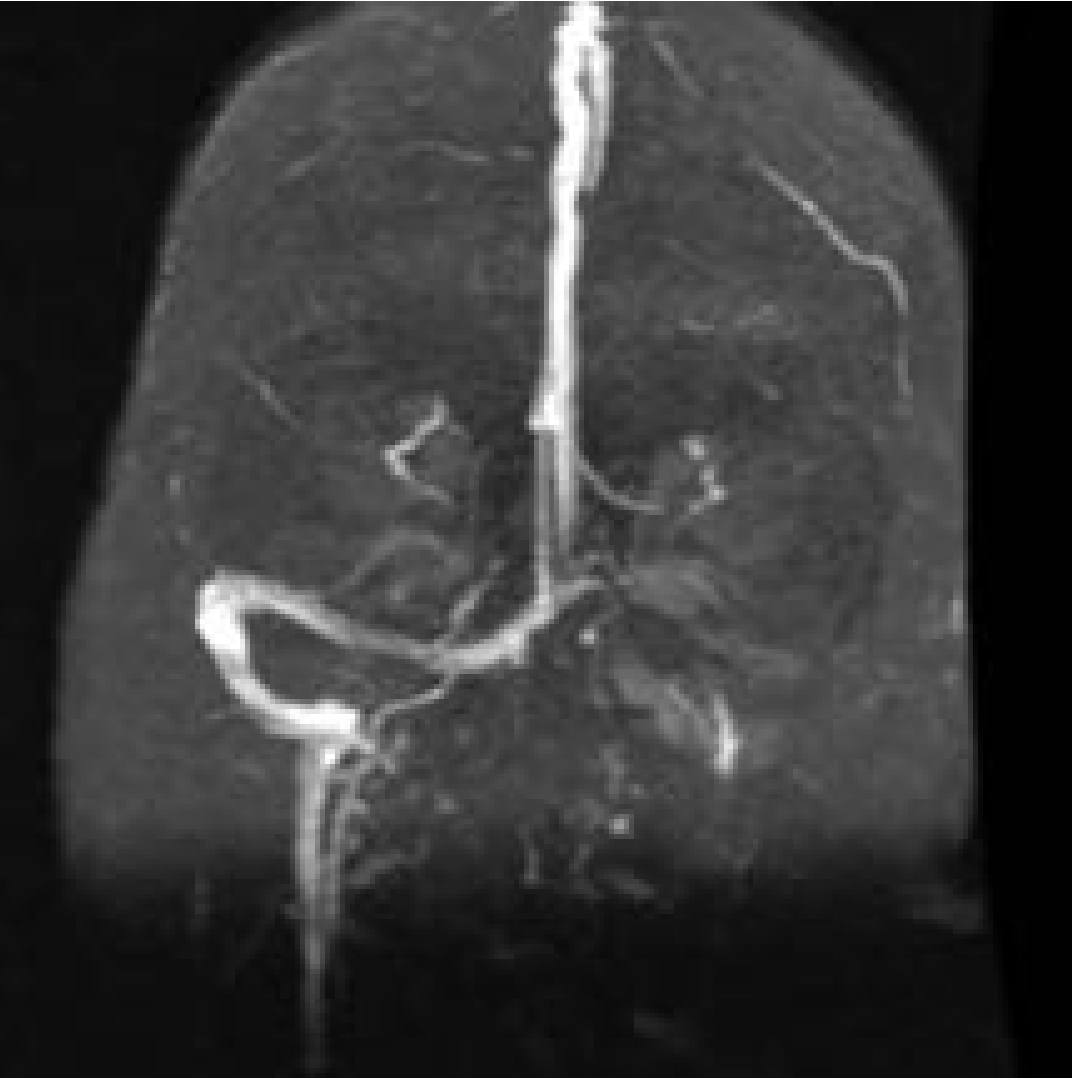
Fig: Magnetic resonance venogram shows occlusion of left transverse-sigmoid sinus system. — Cummings Otolaryngology, p. 2722
3. Otomicroscopy/Ear Examination:
- Ear discharge (purulent/mucopurulent)
- Perforated tympanic membrane / cholesteatoma
4. Chest X-Ray:
- Septic pulmonary emboli (rounded opacities, cavitation — "cannon ball" lesions)
8. DIAGNOSIS
Diagnostic Criteria (Cummings):
Diagnosis is strongly suspected when signs/symptoms of septicemia OR blockage of venous blood flow occur in a patient with otomastoiditis:
DIAGNOSIS: Lateral Sinus Thrombophlebitis
┌──────────────────────────────────────────────────────┐
│ CLINICAL: │
│ • History of chronic/acute ear disease │
│ • Picket-fence fever + rigors │
│ • Headache, postauricular edema (Griesinger's) │
│ • +ve Tobey-Ayer test │
├──────────────────────────────────────────────────────┤
│ RADIOLOGICAL: │
│ • CT: Empty Delta / Absent sigmoid enhancement │
│ • MRI: Thrombus signal in sinus │
│ • MRV: Absent flow in affected sinus │
├──────────────────────────────────────────────────────┤
│ INTRAOPERATIVE: │
│ • Needle aspiration of sinus → thrombus confirmed │
│ • Perisinus abscess found │
└──────────────────────────────────────────────────────┘
9. COMPLICATIONS OF LST
- Otitic Hydrocephalus — raised ICP without true hydrocephalus; due to reduced CSF absorption when major venous sinus occluded (particularly right transverse sinus which is normally dominant)
- Meningitis — most common associated intracranial complication
- Cerebellar Abscess — adjacent to sigmoid sinus
- Temporal Lobe Abscess — otogenic
- Septic Pulmonary Emboli — cannon ball lesions
- Metastatic abscesses — joints, liver
- Jugular Foramen Syndrome (Vernet's) — CN IX, X, XI palsies
- Cavernous Sinus Thrombosis — via petrosal sinuses
- Death — in untreated/delayed cases
10. MANAGEMENT
Management is multidisciplinary and involves medical + surgical treatment.
MANAGEMENT FLOWCHART:
SUSPECTED LST (Otomastoiditis + Septicemia)
|
┌──────────▼──────────┐
│ INVESTIGATIONS │
│ CBC, Blood C/S, CT │
│ MRI/MRV, CSF, CXR │
└──────────┬──────────┘
|
┌──────────▼──────────────────┐
│ MEDICAL MANAGEMENT │
│ IV Antibiotics (broad spec) │
│ + Anticoagulation (debate) │
│ + ICP management (if ↑ICP) │
└──────────┬──────────────────┘
|
┌──────────▼──────────────────────┐
│ SURGICAL MANAGEMENT │
│ Mastoidectomy (cortical / RMW) │
│ + Exposure of sinus │
│ + Perisinus abscess drainage │
│ ± Sinusotomy + thrombectomy │
│ ± IJV ligation (controversial) │
└──────────┬──────────────────────┘
|
┌──────────▼──────────┐
│ POST-OP CARE │
│ Continue IV Abx │
│ Monitor ICP │
│ Anticoagulate PRN │
│ Follow-up MRV │
└─────────────────────┘
A. Medical Management
1. Antibiotics (Mainstay of Treatment):
Empirical IV Antibiotics (broad-spectrum, covering aerobic + anaerobic organisms):
| Drug | Dose | Rationale |
|---|---|---|
| Penicillin G or Ampicillin-sulbactam | High dose IV | Streptococci coverage |
| Metronidazole | 500 mg TDS IV | Anaerobic coverage (especially in cholesteatoma) |
| Ceftriaxone (3rd gen cephalosporin) | 2g BD IV | Gram-negative + CNS penetration |
| Vancomycin (if MRSA suspected) | 15–20 mg/kg IV | MRSA |
- Duration: 4–6 weeks of parenteral antibiotics (prolonged course)
- Adjust based on culture-sensitivity reports
2. Anticoagulation (Controversial):
This remains debated across all textbooks:
| Position | Reference |
|---|---|
| Recommended by some — prevents further thrombosis, promotes recanalization | Cummings, Adams & Victor |
| Uncertain value — not proved definitively | Adams & Victor, p. 2145 |
| Consensus lacking | Cummings, p. 1685 |
Practice: Most centres use IV heparin (unfractionated) followed by oral anticoagulation (warfarin) for 3–6 months, especially when thrombosis is extensive or propagating.
- Contraindications: active intracranial haemorrhage, cerebellar abscess
- Recent evidence: Meta-analyses support anticoagulation improving outcomes in paediatric LST
3. Management of Raised ICP (Otitic Hydrocephalus):
- Head elevation (30°)
- Acetazolamide (carbonic anhydrase inhibitor — reduces CSF production)
- Serial lumbar punctures (therapeutic, to relieve pressure)
- CSF diversion (shunting) in refractory cases
B. Surgical Management
Surgery is the definitive treatment addressing the source and the sinus directly.
Step-by-Step Surgical Approach (Cummings; Scott-Brown):
Step 1: Cortical (Simple) Mastoidectomy or Radical Mastoidectomy with Cavity (RMW)
- The choice depends on whether CSOM with cholesteatoma is present
- Exenterate all mastoid air cells
- Identify and expose the sigmoid sinus plate
Step 2: Perisinus Abscess Drainage
- If perisinus abscess is present → drain it
- Remove all granulation tissue around sinus
- Thin and remove the infected sinus plate with curettes/diamond burs
Step 3: Sinus Needle Aspiration (Griesinger's Technique)
- After exposing the sinus wall → aspirate with needle to confirm thrombus
- Blood returns freely → no thrombus (conservative management)
- No blood returns → occluded sinus
Step 4: Sinusotomy ± Thrombectomy (Stell & Maran; Scott-Brown)
- Incise sinus wall (sinusotomy)
- Evacuate infected thrombus (thrombectomy) with suction or curettes
- Pack sinus with Gelfoam or fat graft
SINUSOTOMY TECHNIQUE:
┌─────────────────────────────────────────┐
│ Mastoidectomy completed │
│ ↓ │
│ Sinus plate thinned/removed │
│ ↓ │
│ Needle aspiration confirms thrombus │
│ ↓ │
│ Longitudinal incision on sinus wall │
│ ↓ │
│ Clot removal with suction / packing │
│ ↓ │
│ Check for bleeding above & below │
│ ↓ │
│ Pack sinus or leave open to cavity │
└─────────────────────────────────────────┘
Step 5: Internal Jugular Vein (IJV) Ligation — (Controversial)
Indications (Dhingra; Hazarika):
- Persistent septicemia/pyemia despite adequate antibiotics and mastoidectomy
- Evidence of propagating thrombus into the neck
- Septic pulmonary emboli (to prevent further embolization)
Technique:
- Transverse neck incision along anterior border of SCM
- Expose IJV between carotid sheath structures
- Ligate IJV at the level of the jugular bulb
- This is rarely performed today due to availability of anticoagulants
Modern view: IJV ligation has been largely abandoned in favour of anticoagulation and aggressive antibiotic therapy.
C. Management of Associated Complications:
| Complication | Management |
|---|---|
| Meningitis | High-dose IV antibiotics ± dexamethasone |
| Cerebellar/Temporal lobe abscess | Neurosurgical drainage + mastoidectomy |
| Septic pulmonary emboli | Anticoagulation; respiratory support |
| Otitic hydrocephalus | Acetazolamide, serial LP, VPS if needed |
| Jugular foramen syndrome | Conservative; antibiotics; usually resolves |
11. COMPLETE MANAGEMENT ALGORITHM
OTOMASTOIDITIS PATIENT
│
▼
Signs of intracranial complication?
(Fever, headache, Griesinger's sign, diplopia, papilledema)
│
▼
URGENT WORKUP:
CT Temporal Bone (contrast) + MRI Brain + MRV
Blood culture, CBC, CSF (if safe)
│
┌───┴────────────────┐
│ │
YES: LST NO: Monitor
│ │
▼ ▼
ADMIT TO ICU Continue treatment
IV Antibiotics of otomastoiditis
(Ceftriaxone +
Metronidazole ±
Vancomycin)
│
▼
SURGICAL EXPLORATION
Mastoidectomy
│
▼
Perisinus abscess present?
│
┌─┴──┐
YES NO
│ │
Drain Continue
abscess medical Rx
│
▼
Needle aspiration of sinus
Blood returns? ──YES──→ Conservative (no sinusotomy needed)
│
NO
│
▼
SINUSOTOMY + THROMBECTOMY
│
▼
Persistent sepsis / propagating thrombus into neck?
│
├──YES──→ Consider IJV Ligation (rarely done today)
│ OR Intensify anticoagulation
│
NO
│
▼
POSTOPERATIVE:
IV Antibiotics × 4–6 weeks
Anticoagulation (Heparin → Warfarin × 3–6 months)
Serial MRV at 3 and 6 months
Monitor ICP / treat otitic hydrocephalus
12. RECENT ADVANCES
A. Anticoagulation Evidence (2010s–2024):
- Systematic reviews (Rodriguez et al., 2023; Funamura et al., 2014) support anticoagulation in paediatric LST, showing improved recanalization rates and reduced propagation
- Low-molecular-weight heparin (LMWH) — increasingly preferred over unfractionated heparin for ease of use and predictable dosing
- Direct oral anticoagulants (DOACs) — emerging role in adult LST (rivaroxaban, apixaban), though paediatric data limited
B. Conservative Non-Surgical Approach:
- Recent publications (Symms et al.; Ooi et al.) describe successful management with antibiotics alone + anticoagulation without sinusotomy in selected cases, particularly in the antibiotic era
- Sinusotomy with thrombectomy is now reserved for refractory cases
C. Diagnostic Advances:
- MR Venography (MRV) is now the gold standard — replaced Tobey-Ayer test
- Diffusion-weighted MRI (DWI) — identifies associated brain abscess
- CT angiography — alternative to MRV in emergency settings
- Blood D-dimer — elevated in active thrombosis; useful for monitoring treatment response
D. Microbiological Advances:
- Streptococcus milleri group increasingly recognized in otogenic LST
- MRSA-related LST — increasing; requires vancomycin/linezolid
- PCR-based identification of organisms from blood/sinus aspirate
E. Endovascular Approaches:
- Catheter-directed thrombolysis (intra-sinus tPA) — described in refractory adult cases; not standard practice
- Mechanical thrombectomy — case reports in literature; remains experimental
F. Outcome Studies:
- Long-term recanalization — occurs in 80–100% of cases with anticoagulation on follow-up MRV
- Mortality — reduced from >50% (pre-antibiotic era) to <5% with modern management
- Residual deficits — hearing loss most common; neurological deficits rare with early treatment
13. STAGING (Chandler Classification — Modified for LST)
While Chandler's classification was for orbital complications, a similar staging concept applies to otogenic complications in terms of severity and surgical urgency:
| Stage | Description |
|---|---|
| I | Perisinus abscess only (no intraluminal thrombus) |
| II | Mural thrombus (non-occlusive) |
| III | Occlusive thrombus, no septicemia |
| IV | Occlusive thrombus + septicemia/bacteremia |
| V | Septicemia + metastatic abscesses (otopyemia) |
14. PROGNOSIS
- Mortality in modern era: <5% with early diagnosis and treatment
- Morbidity factors: delay in diagnosis, associated intracranial complications, virulent organisms (MRSA), young age with immunocompromise
- Hearing loss — permanent conductive or mixed hearing loss expected from CSOM/cholesteatoma
- Sinus recanalization — occurs in majority with anticoagulation; monitored by serial MRV
- Cranial nerve recovery — jugular foramen syndrome usually recovers with antibiotic treatment
SUMMARY TABLE
| Feature | Detail |
|---|---|
| Definition | Infective thrombophlebitis of sigmoid/transverse sinus from otogenic source |
| Most common cause | CSOM with cholesteatoma |
| Pathogenesis | Perisinus abscess → endophlebitis → mural thrombus → infected propagating clot |
| Classic triad | Picket fence fever + headache + otomastoiditis |
| Pathognomonic sign | Griesinger's sign (postauricular oedema over mastoid emissary) |
| Best investigation | MRI + MR Venography |
| CT finding | Empty delta sign (absent sigmoid enhancement) |
| Surgical treatment | Mastoidectomy ± sinusotomy ± thrombectomy |
| IJV ligation | Controversial; rarely done today |
| Anticoagulation | Recommended by most; consensus incomplete |
| Prognosis | Mortality <5% in modern era |
KEY REFERENCES
- Cummings Otolaryngology Head and Neck Surgery (6th Ed.) — Ch. 141: Complications of Temporal Bone Infections, pp. 2720–2725
- Adams and Victor's Principles of Neurology (12th Ed.) — Septic Transverse (Lateral) Sinus Thrombophlebitis, p. 2144
- Tintinalli's Emergency Medicine — Complications of Otitis Media: Lateral Sinus Thrombosis
- Dhingra PL — Diseases of Ear Nose and Throat: Intracranial Complications of CSOM
- Hazarika P — Textbook of ENT and Head & Neck Surgery: Complications of Chronic Otitis Media
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery — Intracranial Complications
- Stell & Maran's Head and Neck Surgery — Otogenic Intracranial Complications
- Funamura JL et al. (2014): Anticoagulation in paediatric sigmoid sinus thrombosis — Int J Pediatr Otorhinolaryngol
- Symms MJ et al. (1999): Management of lateral sinus thrombosis — Laryngoscope 109:1616–1620
Note: Image generation is currently unavailable due to a monthly plan limit. The ASCII-format flowcharts and diagrams above serve the same pedagogical purpose. To access AI-generated visual diagrams and flowcharts, please upgrade your subscription plan or contact support.
This is a shared conversation. Sign in to Orris to start your own chat.