i want ppt of golmerularnephritis
Create a PowerPoint presentation (.pptx) file on **Glomerulonephritis** for medical students at an overview/basic level. Save it to `/home/user/Glomerulonephritis.pptx`. Use the `python-pptx` library to generate the file programmatically. Write and execute a Python script to create the PPTX. Here is the full content to include across slides: --- **SLIDE 1 – Title Slide** Title: Glomerulonephritis (GN) Subtitle: An Overview for Medical Students Footer: Sources: Harrison's Principles of Internal Medicine 22E; Comprehensive Clinical Nephrology, 7th Ed. --- **SLIDE 2 – What is Glomerulonephritis?** - Inflammation of the glomeruli — the filtering units of the kidney - Leads to impaired filtration, proteinuria, hematuria, and renal dysfunction - Can be primary (idiopathic) or secondary (due to systemic disease, infection, autoimmune) - Presents as acute, subacute (days–weeks), or chronic (months–years) disease - Early diagnosis is critical to prevent progression to chronic kidney failure --- **SLIDE 3 – Glomerular Anatomy (Quick Review)** - Each kidney contains ~1 million nephrons - Glomerulus = a tuft of capillaries enclosed in Bowman's capsule - Key cell types: Endothelial cells, Mesangial cells, Podocytes - Glomerular Basement Membrane (GBM) — made of Type IV collagen (α3:α4:α5) - Slit-pore membrane (nephrin, podocin) acts as a protein filter - Damage to any of these components → glomerular disease --- **SLIDE 4 – Clinical Presentation** Two main syndromes: **Nephritic Syndrome:** - Hematuria (cola/tea-colored urine — "macroscopic hematuria") - Hypertension - Oliguria / Anuria - Mild-to-moderate proteinuria - Edema - Dysmorphic RBCs and RBC casts on urinalysis — hallmark finding **Nephrotic Syndrome:** - Heavy proteinuria (>3.5 g/day) - Hypoalbuminemia - Edema - Hyperlipidemia / Lipiduria --- **SLIDE 5 – Urinalysis in GN** - Spun urinary sediment is essential to diagnose active GN - Key findings: • Hematuria — microscopic or macroscopic • Dysmorphic red blood cells (RBCs cross glomerular membrane → misshapen) • RBC casts → strongly suggest glomerular origin of hematuria • Pyuria (WBCs) • Proteinuria - Macroscopic hematuria: "cola" or "tea-colored" urine from hematin formation in acid urine - IgA nephropathy: may show gross red hematuria --- **SLIDE 6 – Classification of GN** **By Onset:** - Acute GN — sudden onset (e.g., Postinfectious GN) - Rapidly Progressive GN (RPGN) — rapid decline in renal function over days–weeks - Chronic GN — gradual progression over months–years **By Pathogenesis (3 major categories of RPGN):** 1. ANCA-positive vasculitis (pauci-immune) 2. Anti-GBM antibody disease (Goodpasture disease) 3. Immune complex-mediated (low C3) — IgA nephropathy, PSGN, SLE, MPGN --- **SLIDE 7 – Postinfectious GN (PSGN)** - Classic example of acute GN - Caused by nephritogenic strains of Group A β-hemolytic Streptococcus - Occurs 10 days–3 weeks after pharyngeal or skin (impetigo) infection - Mechanism: Immune complex deposition → complement activation → inflammation - Mostly affects children (5–15 years) - Clinical: Hematuria, hypertension, edema, oliguria, ↓C3 - Investigations: ↑ASO titer, ↓C3, positive throat/skin culture - Prognosis: Most children recover fully; worse prognosis in adults --- **SLIDE 8 – IgA Nephropathy (Berger Disease)** - Most common primary GN worldwide - Pathology: Mesangial IgA deposits - Trigger: Mucosal infections (respiratory, GI) → episodes of gross hematuria - Presents: Recurrent macroscopic hematuria (often after URTI, within 1–2 days) - Urinalysis: Dysmorphic RBCs, RBC casts - Diagnosis: Renal biopsy (mesangial IgA on immunofluorescence) - Treatment: ACE inhibitors, corticosteroids in progressive cases - Course: 20–40% progress to ESRD over 20 years --- **SLIDE 9 – Rapidly Progressive GN (RPGN)** - Medical emergency — rapid loss of renal function over days to weeks - Pathology: Crescents in >50% of glomeruli (crescentic GN) - Three types: 1. Type I — Anti-GBM (linear IgG on IF) — Goodpasture disease 2. Type II — Immune complex (granular IgG on IF) — SLE, PSGN, IgA 3. Type III — Pauci-immune (ANCA-positive) — GPA, MPA - Treatment: Urgent high-dose steroids ± cyclophosphamide; plasmapheresis for Type I --- **SLIDE 10 – Secondary Causes of GN** | Cause | Type of GN | |---|---| | SLE | Lupus nephritis (Class III/IV most severe) | | Hepatitis B | Membranous GN, MPGN | | Hepatitis C | MPGN, Cryoglobulinemic GN | | Diabetes | Diabetic nephropathy | | ANCA vasculitis | Crescentic (Pauci-immune) GN | | Anti-GBM | Goodpasture disease | --- **SLIDE 11 – Investigations** | Test | Finding/Purpose | |---|---| | Urinalysis + Microscopy | RBCs, RBC casts, proteinuria | | 24h urine protein | Quantify proteinuria | | Serum creatinine/BUN | Assess renal function | | Complement (C3, C4) | Low in PSGN, SLE, MPGN | | ASO titer | Post-streptococcal GN | | ANA, anti-dsDNA | SLE | | ANCA (c-ANCA, p-ANCA) | Vasculitis | | Anti-GBM antibodies | Goodpasture disease | | Renal Biopsy | Gold standard for diagnosis | --- **SLIDE 12 – Management Overview** **General measures:** - Blood pressure control (ACE inhibitors / ARBs) - Salt and fluid restriction - Treat underlying cause **Specific:** - PSGN: Antibiotics for active infection; supportive care (most self-limiting) - IgA nephropathy: ACE-I/ARB; steroids for persistent proteinuria - RPGN: Pulse IV methylprednisolone + cyclophosphamide; plasmapheresis (anti-GBM) - Lupus nephritis: Steroids + MMF or cyclophosphamide **Dialysis** if ESRD develops --- **SLIDE 13 – Summary** - GN = glomerular inflammation → hematuria, proteinuria, hypertension, ↓GFR - Hallmark urinalysis: RBC casts + dysmorphic RBCs - Main categories: Postinfectious, IgA, RPGN, Lupus nephritis - RPGN is a medical emergency — crescents on biopsy - Three RPGN types: Anti-GBM | Immune complex | Pauci-immune (ANCA) - Treatment depends on type: Steroids, cyclophosphamide, plasmapheresis - Renal biopsy = gold standard for diagnosis --- **SLIDE 14 – References** - Harrison's Principles of Internal Medicine, 22nd Edition (2025), McGraw Hill - Comprehensive Clinical Nephrology, 7th Edition — Elsevier - Swanson's Family Medicine Review --- **Design instructions:** - Use a clean, professional medical theme with a blue/navy color scheme - Title slide: dark blue background, white text - Content slides: white background, dark blue headings, black body text - Use bullet points clearly with adequate font size (28–32pt for headings, 18–20pt for body) - Use tables where indicated - Add slide numbers to all slides - The presentation should have 14 slides total Save the file as `/home/user/Glomerulonephritis.pptx` After creating the file, confirm its path and file size.
/home/user/make_gn_ppt.py
from pptx import Presentation
from pptx.util import Inches, Pt, Emu
from pptx.dml.color import RGBColor
from pptx.enum.text import PP_ALIGN
from pptx.util import Inches, Pt
from pptx.oxml.ns import qn
from lxml import etree
import copy
prs = Presentation()
prs.slide_width = Inches(13.33)
prs.slide_height = Inches(7.5)
NAVY = RGBColor(0x00, 0x33, 0x6A)
WHITE = RGBColor(0xFF, 0xFF, 0xFF)
LIGHT_BLUE = RGBColor(0xD6, 0xE4, 0xF0)
BLACK = RGBColor(0x1A, 0x1A, 0x2E)
ACCENT = RGBColor(0x00, 0x86, 0xC8)
blank_layout = prs.slide_layouts[6] # blank
def add_rect(slide, left, top, width, height, fill_color=None, line_color=None):
shape = slide.shapes.add_shape(1, Inches(left), Inches(top), Inches(width), Inches(height))
if fill_color:
shape.fill.solid()
shape.fill.fore_color.rgb = fill_color
else:
shape.fill.background()
if line_color:
shape.line.color.rgb = line_color
shape.line.width = Pt(1)
else:
shape.line.fill.background()
return shape
def add_textbox(slide, text, left, top, width, height, font_size=18, bold=False,
color=BLACK, align=PP_ALIGN.LEFT, wrap=True):
txBox = slide.shapes.add_textbox(Inches(left), Inches(top), Inches(width), Inches(height))
tf = txBox.text_frame
tf.word_wrap = wrap
p = tf.paragraphs[0]
p.alignment = align
run = p.add_run()
run.text = text
run.font.size = Pt(font_size)
run.font.bold = bold
run.font.color.rgb = color
return txBox
def add_slide_number(slide, num):
txBox = slide.shapes.add_textbox(Inches(12.5), Inches(7.1), Inches(0.7), Inches(0.3))
tf = txBox.text_frame
p = tf.paragraphs[0]
p.alignment = PP_ALIGN.RIGHT
run = p.add_run()
run.text = str(num)
run.font.size = Pt(12)
run.font.color.rgb = RGBColor(0x88, 0x88, 0x88)
def add_header_bar(slide, title_text, slide_num):
# Top navy bar
bar = add_rect(slide, 0, 0, 13.33, 1.1, fill_color=NAVY)
# Title text
txBox = slide.shapes.add_textbox(Inches(0.3), Inches(0.1), Inches(12.7), Inches(0.9))
tf = txBox.text_frame
tf.word_wrap = True
p = tf.paragraphs[0]
p.alignment = PP_ALIGN.LEFT
run = p.add_run()
run.text = title_text
run.font.size = Pt(30)
run.font.bold = True
run.font.color.rgb = WHITE
add_slide_number(slide, slide_num)
def add_bullet_slide(slide, title, bullets, slide_num, cols=1):
add_header_bar(slide, title, slide_num)
# White background
bg = add_rect(slide, 0, 0, 13.33, 7.5, fill_color=WHITE)
bg.zorder = 0
add_header_bar(slide, title, slide_num)
top = 1.25
for bullet in bullets:
indent = bullet.get('indent', 0)
text = bullet.get('text', '')
is_header = bullet.get('header', False)
left = 0.4 + indent * 0.35
width = 12.5 - indent * 0.35
if is_header:
txBox = slide.shapes.add_textbox(Inches(left), Inches(top), Inches(width), Inches(0.45))
tf = txBox.text_frame
tf.word_wrap = True
p = tf.paragraphs[0]
run = p.add_run()
run.text = text
run.font.size = Pt(20)
run.font.bold = True
run.font.color.rgb = ACCENT
top += 0.42
else:
# bullet point
prefix = " " * indent + ("• " if indent == 0 else "◦ ")
txBox = slide.shapes.add_textbox(Inches(left), Inches(top), Inches(width), Inches(0.38))
tf = txBox.text_frame
tf.word_wrap = True
p = tf.paragraphs[0]
run = p.add_run()
run.text = prefix + text
run.font.size = Pt(18)
run.font.bold = False
run.font.color.rgb = BLACK
top += 0.36
return slide
def add_table_slide(slide, title, headers, rows, slide_num):
add_header_bar(slide, title, slide_num)
bg = add_rect(slide, 0, 0, 13.33, 7.5, fill_color=WHITE)
bg.zorder = 0
add_header_bar(slide, title, slide_num)
cols = len(headers)
num_rows = len(rows) + 1
table = slide.shapes.add_table(num_rows, cols, Inches(0.4), Inches(1.3), Inches(12.5), Inches(0.45 * num_rows)).table
# Header row
for ci, h in enumerate(headers):
cell = table.cell(0, ci)
cell.fill.solid()
cell.fill.fore_color.rgb = NAVY
p = cell.text_frame.paragraphs[0]
run = p.add_run()
run.text = h
run.font.size = Pt(17)
run.font.bold = True
run.font.color.rgb = WHITE
for ri, row in enumerate(rows):
for ci, val in enumerate(row):
cell = table.cell(ri + 1, ci)
if ri % 2 == 0:
cell.fill.solid()
cell.fill.fore_color.rgb = LIGHT_BLUE
else:
cell.fill.solid()
cell.fill.fore_color.rgb = WHITE
p = cell.text_frame.paragraphs[0]
run = p.add_run()
run.text = val
run.font.size = Pt(15)
run.font.color.rgb = BLACK
# ─── SLIDE 1: Title ───────────────────────────────────────────────────────────
slide1 = prs.slides.add_slide(blank_layout)
bg1 = add_rect(slide1, 0, 0, 13.33, 7.5, fill_color=NAVY)
# Decorative accent
add_rect(slide1, 0, 5.8, 13.33, 0.12, fill_color=ACCENT)
add_rect(slide1, 0, 5.92, 13.33, 1.58, fill_color=RGBColor(0x00, 0x1A, 0x40))
txBox = slide1.shapes.add_textbox(Inches(1), Inches(1.5), Inches(11), Inches(2.2))
tf = txBox.text_frame
tf.word_wrap = True
p = tf.paragraphs[0]
p.alignment = PP_ALIGN.CENTER
run = p.add_run()
run.text = "Glomerulonephritis (GN)"
run.font.size = Pt(52)
run.font.bold = True
run.font.color.rgb = WHITE
txBox2 = slide1.shapes.add_textbox(Inches(1), Inches(3.5), Inches(11), Inches(0.6))
tf2 = txBox2.text_frame
p2 = tf2.paragraphs[0]
p2.alignment = PP_ALIGN.CENTER
run2 = p2.add_run()
run2.text = "An Overview for Medical Students"
run2.font.size = Pt(26)
run2.font.color.rgb = LIGHT_BLUE
txBox3 = slide1.shapes.add_textbox(Inches(1), Inches(6.1), Inches(11), Inches(0.5))
tf3 = txBox3.text_frame
p3 = tf3.paragraphs[0]
p3.alignment = PP_ALIGN.CENTER
run3 = p3.add_run()
run3.text = "Sources: Harrison's Principles of Internal Medicine 22E | Comprehensive Clinical Nephrology, 7th Ed."
run3.font.size = Pt(13)
run3.font.color.rgb = RGBColor(0xAA, 0xCC, 0xEE)
add_slide_number(slide1, 1)
# ─── SLIDE 2: What is GN ─────────────────────────────────────────────────────
slide2 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide2, "What is Glomerulonephritis?", [
{'text': 'Inflammation of the glomeruli — the microscopic filtering units of the kidney'},
{'text': 'Results in impaired filtration → proteinuria, hematuria, and renal dysfunction'},
{'text': 'Can be primary (idiopathic) or secondary (systemic disease, infection, autoimmune)'},
{'text': 'Presentation:'},
{'text': 'Acute (sudden onset)', 'indent': 1},
{'text': 'Subacute (days to weeks)', 'indent': 1},
{'text': 'Chronic (months to years — progressive)', 'indent': 1},
{'text': 'Early diagnosis is critical to prevent progression to chronic kidney failure'},
{'text': 'Volume expansion → edema, hypertension; oliguria/anuria common'},
], 2)
# ─── SLIDE 3: Glomerular Anatomy ─────────────────────────────────────────────
slide3 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide3, "Glomerular Anatomy — Quick Review", [
{'text': 'Each kidney has ~1 million nephrons'},
{'text': 'Glomerulus = tuft of capillaries enclosed in Bowman's capsule'},
{'text': 'Key cell types:'},
{'text': 'Endothelial cells (fenestrated) — allow fluid filtration', 'indent': 1},
{'text': 'Mesangial cells — structural support, phagocytic function', 'indent': 1},
{'text': 'Podocytes — wrap around capillaries; form slit-pore membrane', 'indent': 1},
{'text': 'Glomerular Basement Membrane (GBM): Type IV collagen (α3:α4:α5)'},
{'text': 'Slit-pore membrane proteins: Nephrin, Podocin — act as protein size filter'},
{'text': 'Damage to any component → glomerular disease (proteinuria, hematuria)'},
], 3)
# ─── SLIDE 4: Clinical Presentation ─────────────────────────────────────────
slide4 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide4, "Clinical Presentation", [
{'text': 'Nephritic Syndrome', 'header': True},
{'text': 'Hematuria (cola/tea-colored urine — macroscopic hematuria)'},
{'text': 'Hypertension, Oliguria/Anuria'},
{'text': 'Mild-to-moderate proteinuria'},
{'text': 'Edema (periorbital, peripheral, ascites in children)'},
{'text': 'Dysmorphic RBCs and RBC casts on urinalysis — hallmark'},
{'text': 'Nephrotic Syndrome', 'header': True},
{'text': 'Heavy proteinuria (>3.5 g/day)'},
{'text': 'Hypoalbuminemia → edema'},
{'text': 'Hyperlipidemia and lipiduria'},
{'text': 'Note: Some GN presents with overlapping features (nephritic-nephrotic)'},
], 4)
# ─── SLIDE 5: Urinalysis ─────────────────────────────────────────────────────
slide5 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide5, "Urinalysis in GN", [
{'text': 'Spun urinary sediment is ESSENTIAL to diagnose active GN'},
{'text': 'Key findings:'},
{'text': 'Hematuria — microscopic or macroscopic', 'indent': 1},
{'text': 'Dysmorphic RBCs — RBCs distorted as they cross damaged GBM', 'indent': 1},
{'text': 'RBC casts — strongly suggest glomerular origin of hematuria ★', 'indent': 1},
{'text': 'Pyuria (WBCs) — mixed inflammatory cells', 'indent': 1},
{'text': 'Proteinuria', 'indent': 1},
{'text': 'Macroscopic hematuria: "cola" or "tea-colored" urine'},
{'text': ' → Hematin forms when hemoglobin enters acidic urine'},
{'text': 'IgA nephropathy: gross RED hematuria (RBCs cross diseased GBM)'},
{'text': 'Blood clots or grossly red urine → consider lower urinary tract cause'},
], 5)
# ─── SLIDE 6: Classification ─────────────────────────────────────────────────
slide6 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide6, "Classification of GN", [
{'text': 'By Onset / Course', 'header': True},
{'text': 'Acute GN — sudden onset (e.g., Post-streptococcal GN)'},
{'text': 'Rapidly Progressive GN (RPGN) — rapid decline over days–weeks'},
{'text': 'Chronic GN — gradual progression over months–years'},
{'text': '3 Major Pathogenic Categories (RPGN)', 'header': True},
{'text': 'Type I — Anti-GBM antibody disease (Goodpasture disease)'},
{'text': 'Type II — Immune complex-mediated (low C3) — IgA, PSGN, SLE, MPGN'},
{'text': 'Type III — Pauci-immune / ANCA-positive — GPA (Wegener), MPA'},
{'text': 'Primary vs Secondary', 'header': True},
{'text': 'Primary: Idiopathic — IgA nephropathy, FSGS, Minimal change'},
{'text': 'Secondary: SLE, Diabetes, Vasculitis, Infections (Hep B/C, HIV)'},
], 6)
# ─── SLIDE 7: PSGN ───────────────────────────────────────────────────────────
slide7 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide7, "Postinfectious GN (PSGN)", [
{'text': 'Classic example of acute GN'},
{'text': 'Cause: Nephritogenic strains of Group A β-hemolytic Streptococcus'},
{'text': 'Latent period: 10 days–3 weeks after pharyngeal or skin (impetigo) infection'},
{'text': 'Mechanism: Immune complex (Ag-Ab) deposition → complement activation → inflammation'},
{'text': 'Mainly affects children (5–15 years)'},
{'text': 'Clinical features:'},
{'text': 'Hematuria, hypertension, periorbital edema, oliguria', 'indent': 1},
{'text': 'Investigations:'},
{'text': '↑ ASO titer (pharyngeal infection)', 'indent': 1},
{'text': '↓ C3 complement', 'indent': 1},
{'text': 'Positive throat / skin culture', 'indent': 1},
{'text': 'Prognosis: Children — excellent recovery; Adults — worse prognosis'},
], 7)
# ─── SLIDE 8: IgA Nephropathy ────────────────────────────────────────────────
slide8 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide8, "IgA Nephropathy (Berger Disease)", [
{'text': 'Most common primary GN worldwide'},
{'text': 'Pathology: Mesangial IgA immune complex deposits'},
{'text': 'Trigger: Mucosal infections (respiratory, GI) → IgA overproduction'},
{'text': 'Presentation: Recurrent GROSS hematuria, typically 1–2 days after URTI'},
{'text': 'Urinalysis: Dysmorphic RBCs, RBC casts'},
{'text': 'Diagnosis: Renal biopsy — mesangial IgA on immunofluorescence (gold standard)'},
{'text': 'Treatment:'},
{'text': 'ACE inhibitors / ARBs — first line (proteinuria reduction)', 'indent': 1},
{'text': 'Corticosteroids for persistent significant proteinuria', 'indent': 1},
{'text': 'Course: 20–40% progress to ESRD over 20 years'},
], 8)
# ─── SLIDE 9: RPGN ───────────────────────────────────────────────────────────
slide9 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide9, "Rapidly Progressive GN (RPGN)", [
{'text': '⚠ Medical emergency — rapid loss of renal function over days to weeks'},
{'text': 'Pathology: Crescents in >50% of glomeruli (crescentic GN) on biopsy'},
{'text': 'Three Types:', 'header': True},
{'text': 'Type I — Anti-GBM (Goodpasture disease)'},
{'text': ' Linear IgG deposition on immunofluorescence'},
{'text': ' May have lung hemorrhage (pulmonary-renal syndrome)'},
{'text': 'Type II — Immune Complex (SLE, PSGN, IgA, MPGN)'},
{'text': ' Granular IgG deposition on immunofluorescence'},
{'text': 'Type III — Pauci-immune (ANCA vasculitis — GPA, MPA)'},
{'text': ' Negative/scant IF, ANCA positive in blood'},
{'text': 'Treatment:', 'header': True},
{'text': 'High-dose IV methylprednisolone + cyclophosphamide'},
{'text': 'Plasmapheresis for Type I (anti-GBM) and severe ANCA'},
], 9)
# ─── SLIDE 10: Secondary Causes — TABLE ──────────────────────────────────────
slide10 = prs.slides.add_slide(blank_layout)
add_table_slide(slide10,
"Secondary Causes of GN",
["Underlying Cause", "Type of GN"],
[
["Systemic Lupus Erythematosus (SLE)", "Lupus nephritis (Class III/IV most severe)"],
["Hepatitis B", "Membranous GN, MPGN"],
["Hepatitis C", "MPGN, Cryoglobulinemic GN"],
["Diabetes Mellitus", "Diabetic nephropathy"],
["ANCA-associated vasculitis (GPA, MPA)", "Crescentic (Pauci-immune) GN"],
["Anti-GBM antibodies", "Goodpasture disease"],
["Schistosomiasis", "Immune-mediated GN, AA amyloidosis"],
["Post-streptococcal infection", "Proliferative / Endocapillary GN"],
],
10
)
# ─── SLIDE 11: Investigations — TABLE ────────────────────────────────────────
slide11 = prs.slides.add_slide(blank_layout)
add_table_slide(slide11,
"Investigations",
["Test", "Finding / Purpose"],
[
["Urinalysis + Microscopy", "RBCs, RBC casts, proteinuria — diagnose active GN"],
["24-hour urine protein", "Quantify proteinuria"],
["Serum creatinine / BUN", "Assess renal function"],
["Complement (C3, C4)", "↓ in PSGN, SLE, MPGN"],
["ASO titer", "Post-streptococcal GN"],
["ANA, Anti-dsDNA", "SLE / Lupus nephritis"],
["ANCA (c-ANCA, p-ANCA)", "ANCA vasculitis (GPA, MPA)"],
["Anti-GBM antibodies", "Goodpasture disease"],
["Renal Biopsy", "Gold standard — definitive diagnosis and classification"],
],
11
)
# ─── SLIDE 12: Management ─────────────────────────────────────────────────────
slide12 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide12, "Management Overview", [
{'text': 'General Measures', 'header': True},
{'text': 'Blood pressure control — ACE inhibitors / ARBs (renoprotective)'},
{'text': 'Salt and fluid restriction'},
{'text': 'Treat underlying cause'},
{'text': 'Specific Treatment by Type', 'header': True},
{'text': 'PSGN: Antibiotics for active infection; supportive (mostly self-limiting)'},
{'text': 'IgA nephropathy: ACE-I/ARB; corticosteroids for persistent proteinuria'},
{'text': 'RPGN: Pulse IV methylprednisolone + cyclophosphamide'},
{'text': 'Anti-GBM (Type I RPGN): + Plasmapheresis to remove circulating antibodies'},
{'text': 'Lupus nephritis: Steroids + MMF or cyclophosphamide'},
{'text': 'Dialysis / Renal replacement therapy if ESRD develops'},
], 12)
# ─── SLIDE 13: Summary ────────────────────────────────────────────────────────
slide13 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide13, "Summary", [
{'text': 'GN = glomerular inflammation → hematuria, proteinuria, hypertension, ↓ GFR'},
{'text': 'Hallmark urinalysis: RBC casts + dysmorphic RBCs'},
{'text': 'Main syndromes: Nephritic vs Nephrotic (can overlap)'},
{'text': 'Key types: Postinfectious GN | IgA Nephropathy | RPGN | Lupus nephritis'},
{'text': 'RPGN = medical emergency — crescents on biopsy'},
{'text': 'Three RPGN types:'},
{'text': 'Anti-GBM (Type I)', 'indent': 1},
{'text': 'Immune complex (Type II)', 'indent': 1},
{'text': 'Pauci-immune / ANCA (Type III)', 'indent': 1},
{'text': 'Renal biopsy = gold standard for diagnosis'},
{'text': 'Treatment: Steroids ± cyclophosphamide ± plasmapheresis (based on type)'},
], 13)
# ─── SLIDE 14: References ────────────────────────────────────────────────────
slide14 = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide14, "References", [
{'text': 'Harrison\'s Principles of Internal Medicine, 22nd Edition (2025)'},
{'text': ' McGraw Hill Medical — Chapter 319: Glomerulonephritis'},
{'text': 'Comprehensive Clinical Nephrology, 7th Edition'},
{'text': ' Elsevier — Chapters 25, 57'},
{'text': 'Swanson\'s Family Medicine Review (2021), Elsevier'},
{'text': 'Campbell Walsh Wein Urology, 3-Volume Set — Elsevier'},
{'text': 'Brenner and Rector\'s The Kidney, 2-Volume Set — Elsevier'},
], 14)
# Save
path = '/home/user/Glomerulonephritis.pptx'
prs.save(path)
import os
size = os.path.getsize(path)
print(f"Saved: {path} ({size:,} bytes)")
*.py in /home/user
disease overview or introduction to glomerulonephritis
Glomerulonephritis (GN) — Disease Overview & Introduction
1. Definition
2. The Glomerulus — What Is Being Inflamed?
| Component | Structure & Role |
|---|---|
| Fenestrated endothelium | Lines capillaries; allows fluid filtration |
| Glomerular Basement Membrane (GBM) | Type IV collagen network (α3:α4:α5); structural scaffold |
| Podocytes | Epithelial cells with foot processes; form the slit-pore membrane |
| Mesangial cells | Structural support; phagocytic; contractile |
3. How GN Presents Clinically
Hypertension + Volume expansion + Abnormal urinalysis
Volume expansion manifestations:
- Adults: Edema (peripheral, periorbital), hypertension, orthopnea, dyspnea on exertion
- Children: Ascites may develop
- Elderly: Restlessness and anxiety may be the first signs of incipient acute pulmonary edema
Urinary findings:
- Oliguria (low urine output) or rarely anuria
- Low urine sodium + concentrated urine → salt and water retention
- Spun urinary sediment examination is ESSENTIAL to diagnose active GN
- Hematuria (microscopic or macroscopic)
- Proteinuria
- Dysmorphic red blood cells — RBCs become misshapen as they cross the damaged GBM
- RBC casts — the hallmark of glomerular origin of bleeding
- Mixed inflammatory cells including PMN leukocytes (pyuria)
Macroscopic hematuria: described as "cola" or "tea-colored" urine — hemoglobin enters acid urine and forms hematin. This is classic in post-streptococcal GN and IgA nephropathy (IgA can produce frank red blood-red urine).
4. Primary vs Secondary GN
- IgA Nephropathy (most common worldwide)
- Minimal Change Disease
- Focal Segmental Glomerulosclerosis (FSGS)
- Membranous Nephropathy
- MPGN (Membranoproliferative GN)
- Autoimmune: SLE (lupus nephritis), vasculitis (ANCA-associated)
- Infections: Post-streptococcal, hepatitis B/C, HIV, endocarditis
- Metabolic: Diabetes mellitus, amyloidosis
- Malignancy: Lung/breast/GI adenocarcinoma → membranous nephropathy; Hodgkin disease → minimal change; Non-Hodgkin lymphoma → MPGN
- Drugs/toxins: NSAIDs, penicillamine, pamidronate, heroin, cyclosporine
- Genetic: Alport syndrome, mutations in podocin/nephrin (FSGS)
- Obesity: Morbid obesity → secondary FSGS
5. Classification by Course
| Type | Onset | Timeframe | Example |
|---|---|---|---|
| Acute GN | Sudden | Days to weeks | Post-streptococcal GN |
| Rapidly Progressive GN (RPGN) | Rapid deterioration | Days to weeks | Crescentic GN, Goodpasture |
| Chronic GN | Smoldering, insidious | Months to years | IgA nephropathy, Lupus nephritis |
6. RPGN — Classification by Immunopathology
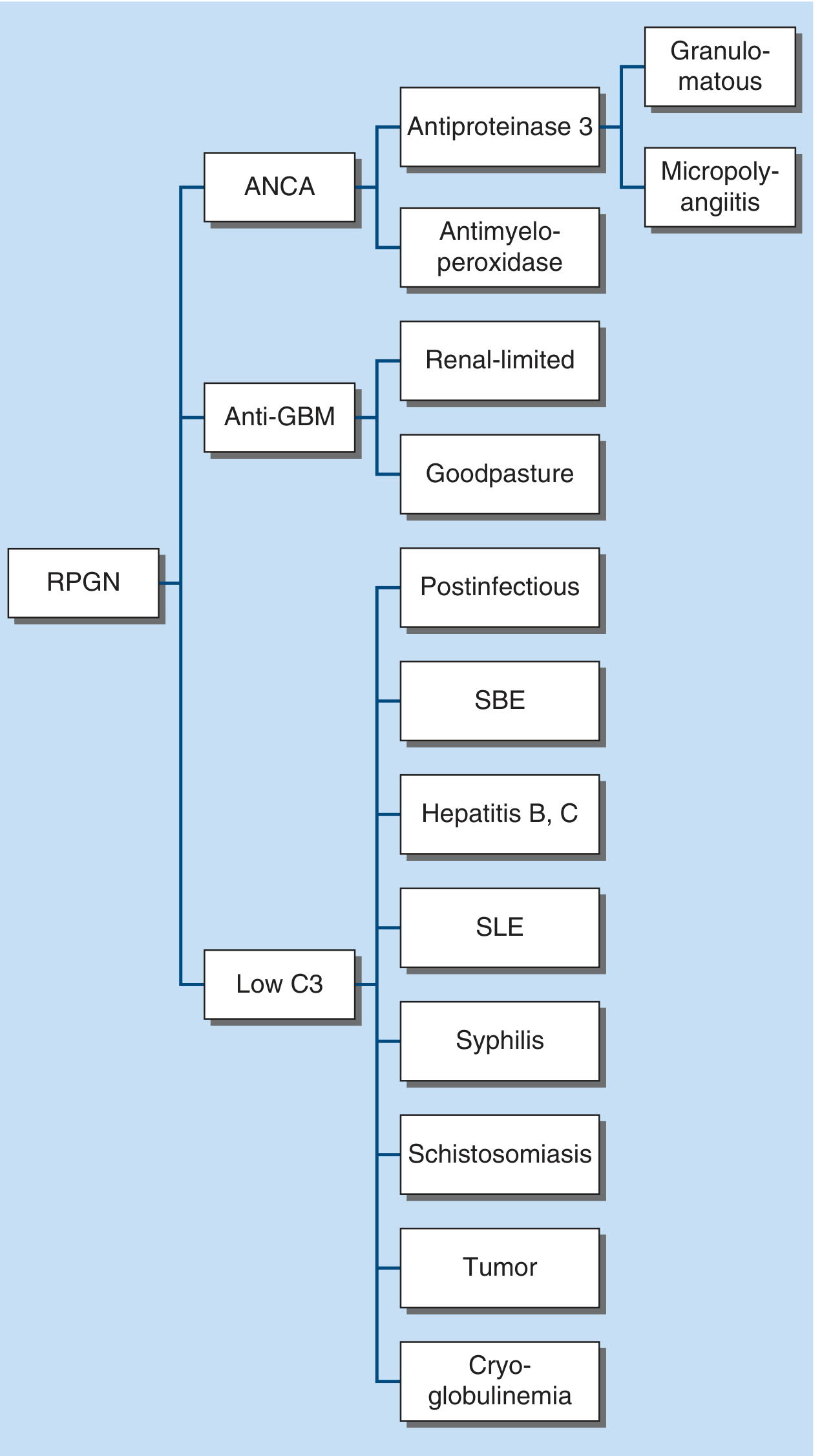
| Type | Mechanism | IF Pattern | Examples |
|---|---|---|---|
| Type I | Anti-GBM antibodies | Linear IgG | Goodpasture disease (renal-limited or with lung hemorrhage) |
| Type II | Immune complex | Granular IgG | PSGN, SLE, IgA nephropathy, MPGN, SBE, Hepatitis B/C |
| Type III | Pauci-immune (ANCA+) | Scant/negative | GPA (Granulomatosis with polyangiitis), Microscopic polyangiitis |
7. Clinical Evaluation Framework
- Exclude non-glomerular disease (e.g., UTI, lower tract bleeding)
- Find evidence of associated multisystem disease (diabetes, SLE, vasculitis, amyloid)
- Establish kidney function (creatinine, eGFR, urinalysis)
- Hearing loss → Alport syndrome
- Recent URTI + hematuria within 1–2 days → IgA nephropathy
- Hematuria 2–3 weeks after throat/skin infection → Post-streptococcal GN
- Hemoptysis + hematuria → Goodpasture disease or ANCA vasculitis
- Butterfly rash + joint pains → SLE/lupus nephritis
- Foamy urine + edema → Heavy proteinuria / nephrotic component
8. The Two Major Clinical Syndromes
| Feature | Nephritic Syndrome | Nephrotic Syndrome |
|---|---|---|
| Hematuria | Yes (prominent) | Mild or absent |
| Proteinuria | Mild–moderate | Heavy (>3.5 g/day) |
| Hypertension | Common | Variable |
| Edema | Yes | Yes (severe) |
| Hypoalbuminemia | Mild | Severe |
| Hyperlipidemia / Lipiduria | No | Yes |
| Hallmark | RBC casts, dysmorphic RBCs | Frothy urine, anasarca |
Many forms of GN present with overlapping nephritic-nephrotic features, particularly IgA nephropathy and lupus nephritis.
9. Why Classification Is Challenging
Summary Table
| Feature | Detail |
|---|---|
| Definition | Glomerular inflammation → impaired filtration |
| Hallmark urine finding | RBC casts + dysmorphic RBCs |
| Core clinical triad | Hematuria + Proteinuria + Hypertension |
| Pathology gold standard | Renal biopsy (LM + IF + EM) |
| Main clinical syndromes | Nephritic vs Nephrotic (can overlap) |
| Acute emergency | RPGN — crescents on biopsy |
| Most common primary GN | IgA nephropathy (worldwide) |
| Classic acute GN | Post-streptococcal GN |
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) — Chapter 319: Glomerulonephritis
- Comprehensive Clinical Nephrology, 7th Edition — Chapter 16: Introduction to Glomerular Disease: Clinical Presentations