22/F High grade fever since 7 days with vomiting Irritable behaviour since 2 days Csf protein 300 Csf glucose -12 Ada-15
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching PubMed
tuberculous meningitis treatment dexamethasone
Loading Image
Now I have all the information needed for a comprehensive clinical response.
Clinical Assessment: Tuberculous Meningitis (TBM)
Diagnosis: Tuberculous Meningitis - strongly supported by all three clinical and lab parameters.
CSF Analysis - Interpretation
| Parameter | This Patient | Typical TBM Range | Interpretation |
|---|---|---|---|
| Protein | 300 mg/dL | 100-500 mg/dL (often >200) | Markedly elevated - hallmark of TBM |
| Glucose | 12 mg/dL | <40 mg/dL (reduced, but rarely as low as pyogenic) | Significantly low - supports TBM |
| ADA | 15 U/L | Elevated above normal in TBM | Elevated; supports mycobacterial/lymphocytic etiology |
Key point on glucose: A CSF glucose of 12 mg/dL is markedly low, but TBM characteristically does NOT produce the near-zero glucose levels seen in pyogenic bacterial meningitis. The glucose falls slowly in TBM and may become very low as disease progresses. Always compare with simultaneous serum glucose - CSF:serum glucose ratio <0.5 is the defining criterion.
Key point on ADA: ADA is elevated in TBM because it is abundant in T-lymphocytes, which are the dominant cell type in the tuberculous inflammatory response. According to Henry's Clinical Diagnosis and Management by Laboratory Methods, "ADA levels are significantly higher in tuberculous meningitis than in other types of meningitis and CNS disorders." A CSF ADA of 15 U/L, while seemingly modest, should be interpreted with the assay-specific cutoff - values >10 U/L in CSF are generally considered elevated and supportive of TBM.
Why This Case Points to TBM and Not Other Causes
Clinical clues supporting TBM over pyogenic meningitis:
- Subacute onset - 7 days of fever is characteristic; pyogenic meningitis typically presents more acutely (hours to 1-2 days)
- Irritability at day 2 of a 7-day illness - gradual neurological deterioration is the TBM pattern
- CSF glucose 12 - very low but not "zero" - fits TBM better than viral (viral rarely drops glucose this severely)
- Protein 300 - markedly elevated, consistent with TBM where thick basal exudate forms
Why not viral (aseptic) meningitis?
- Viral meningitis rarely drops CSF glucose this low (usually normal or mildly reduced)
- Protein of 300 is too high for most viral causes
- ADA elevation points away from viral etiology
Why not pyogenic bacterial meningitis?
- Pyogenic meningitis has a more acute/fulminant onset
- CSF glucose is usually near-zero in pyogenic; here it is 12 (very low but not zero)
- ADA is elevated in both TBM and bacterial meningitis, but the subacute course strongly favors TB
Pathogenesis
M. tuberculosis reaches the CNS via hematogenous spread (often after primary pulmonary TB or miliary dissemination). It forms cortical/meningeal tubercles; when these rupture into the subarachnoid space, an intense basal meningitis develops. A thick gelatinous exudate accumulates around the basal cisterns, obliterating the pontine and interpeduncular cisterns. This causes:
- Cranial nerve palsies (especially CN III, VI, VII)
- Communicating or obstructive hydrocephalus
- Vasculitis leading to cerebral infarction
- Progressive stupor and coma if untreated
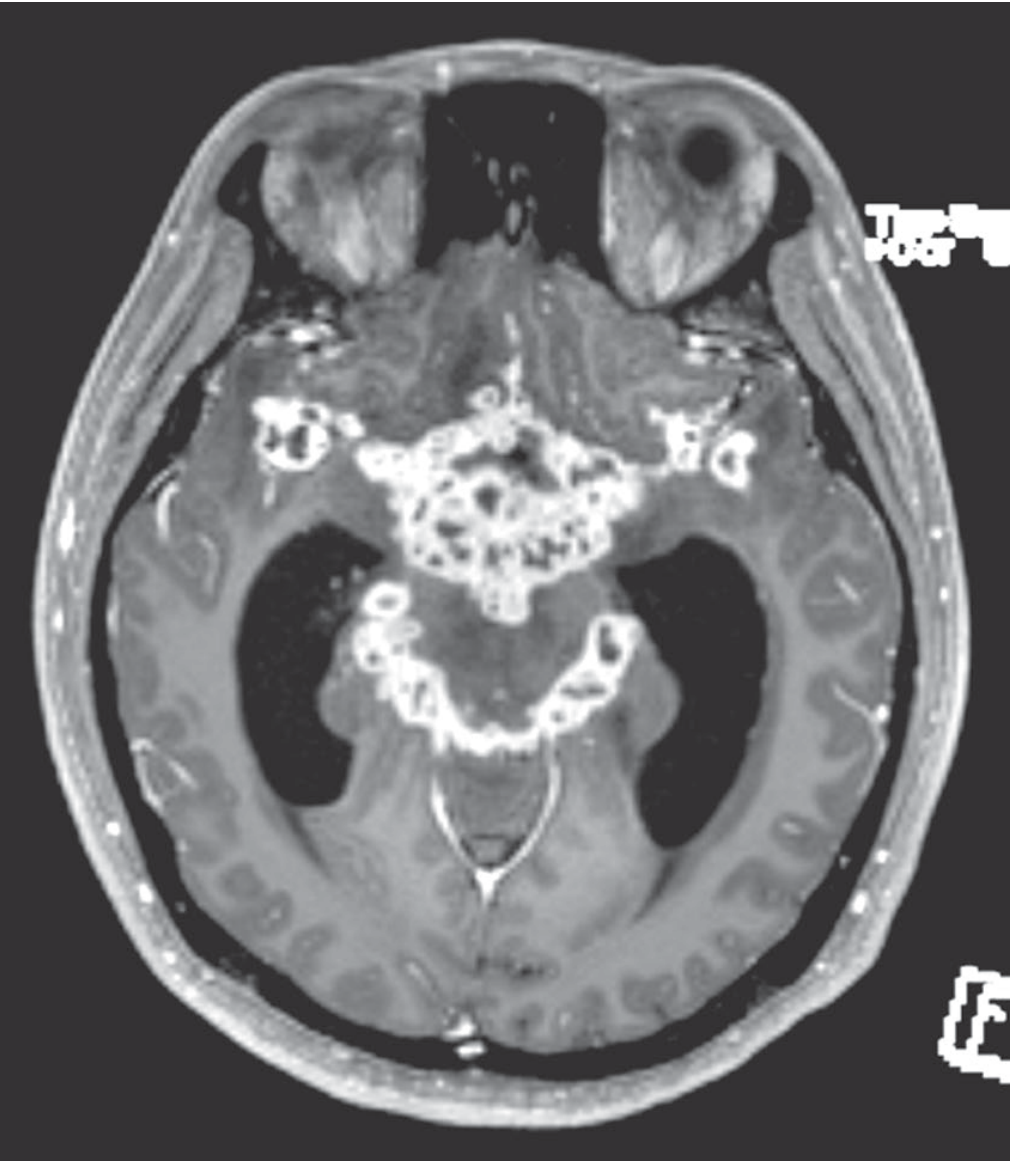
MRI in TBM - gadolinium enhancement of the basal meninges, with multiple abscesses and hydrocephalus:
Staging (British Medical Research Council)
| Stage | Features |
|---|---|
| Stage I | Conscious, no focal deficits, no hydrocephalus |
| Stage II | Confusion OR focal deficit |
| Stage III | Stupor, coma, or severe neurological deficit |
This patient with irritability and a 7-day fever is likely Stage I-II - early intervention is critical.
Investigations to Order
- CSF AFB smear and culture - sensitivity is low (10-50%) but specificity is high; repeat LPs increase yield
- CSF PCR for M. tuberculosis - sensitivity ~80%; rapid result; preferred over culture alone
- Chest X-ray / HRCT chest - look for primary pulmonary focus, miliary pattern
- Tuberculin skin test / IGRA (QuantiFERON-TB Gold) - positive in ~40-60% of adults with TBM
- MRI brain with gadolinium - basal meningeal enhancement, hydrocephalus, tuberculomas, infarcts
- Serum sodium - hyponatremia is common (SIADH or Addisonian state)
- HIV serology - mandatory; HIV dramatically increases TBM risk and alters outcomes
- Fundoscopy - for choroidal tubercles (pathognomonic if present), papilledema
- CSF adenosine deaminase - already done; supportive
Treatment
Anti-tubercular Therapy (ATT)
Intensive phase (2 months) - 4-drug regimen:
| Drug | Adult Dose | Key Toxicity |
|---|---|---|
| Isoniazid (H) | 5 mg/kg/day (max 300 mg) | Hepatitis, peripheral neuropathy |
| Rifampicin (R) | 10 mg/kg/day (max 600 mg) | Hepatitis, drug interactions, orange discoloration of secretions |
| Pyrazinamide (Z) | 25 mg/kg/day | Hepatotoxicity, hyperuricemia |
| Ethambutol (E) | 15 mg/kg/day | Optic neuritis (check visual acuity/color vision regularly) |
Continuation phase (10 months) - 2-drug regimen:
- Isoniazid + Rifampicin
- Total duration for TBM: 12 months (longer than pulmonary TB due to poor CNS penetration)
Add Pyridoxine (Vitamin B6) 25-50 mg/day to prevent INH-induced neuropathy.
Corticosteroids (Adjunctive - Mandatory in TBM)
- Dexamethasone IV: 0.4 mg/kg/day for 1 week, then tapering doses over 3-6 weeks
- Evidence: A landmark randomized trial (Thwaites et al., Vietnam) showed dexamethasone reduced mortality from 41% to 32% without increasing residual disability
- A 2024 meta-analysis (PMID: 38858618) further supports intrathecal dexamethasone + isoniazid as beneficial in select cases
- A 2026 network meta-analysis (PMID: 42112729) evaluates comparative efficacy of drug therapies in TBM
Supportive Care
- Monitor for hydrocephalus - may require ventriculoperitoneal shunting (needed in ~25% of cases)
- Treat hyponatremia cautiously (fluid restrict if SIADH; replace if Addisonian)
- Seizure management if needed
- Nutritional support
Prognosis
- Overall mortality with treatment: ~10% in HIV-negative patients; up to 21% in HIV-positive
- If untreated: fatal within 4-8 weeks
- 20-30% of survivors have residual neurological deficits: cognitive impairment, seizures, hemiparesis, cranial nerve palsies, deafness
- Early diagnosis and treatment are the strongest determinants of outcome
Sources:
- Adams and Victor's Principles of Neurology, 12th Edition
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Tintinalli's Emergency Medicine - A Comprehensive Study
- ROSEN's Emergency Medicine: Concepts and Clinical Practice
- Recent evidence: PMID 38858618 (2024 meta-analysis on intrathecal dexamethasone in TBM); PMID 42112729 (2026 network meta-analysis on TBM drug therapies)
This is a shared conversation. Sign in to Orris to start your own chat.