Macular function tests
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Macular Function Tests
Macular function tests assess the integrity of the central 20° of the visual field and the fovea specifically. They are used to screen for macular disease, differentiate macular from optic nerve pathology, and monitor disease progression.
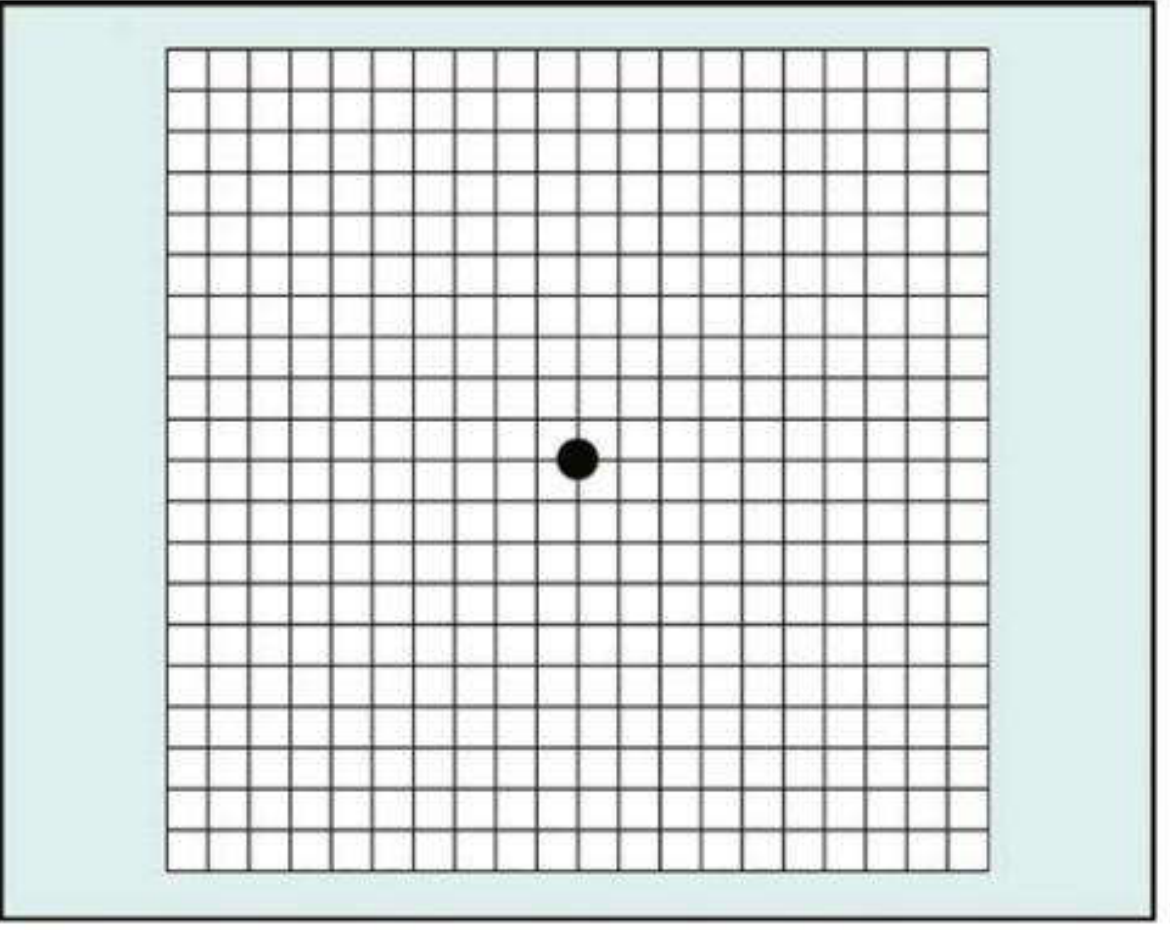
1. Amsler Grid
The most commonly used bedside test for macular function.
Principle: Evaluates the central 20° of the visual field centred on fixation. It detects scotomas, metamorphopsia (distortion), and missing areas caused by macular disease.
Charts (7 available):
| Chart | Description | Use |
|---|---|---|
| 1 | White grid on black background, 400 small squares (each 5 mm = 1° at 33 cm) | Standard |
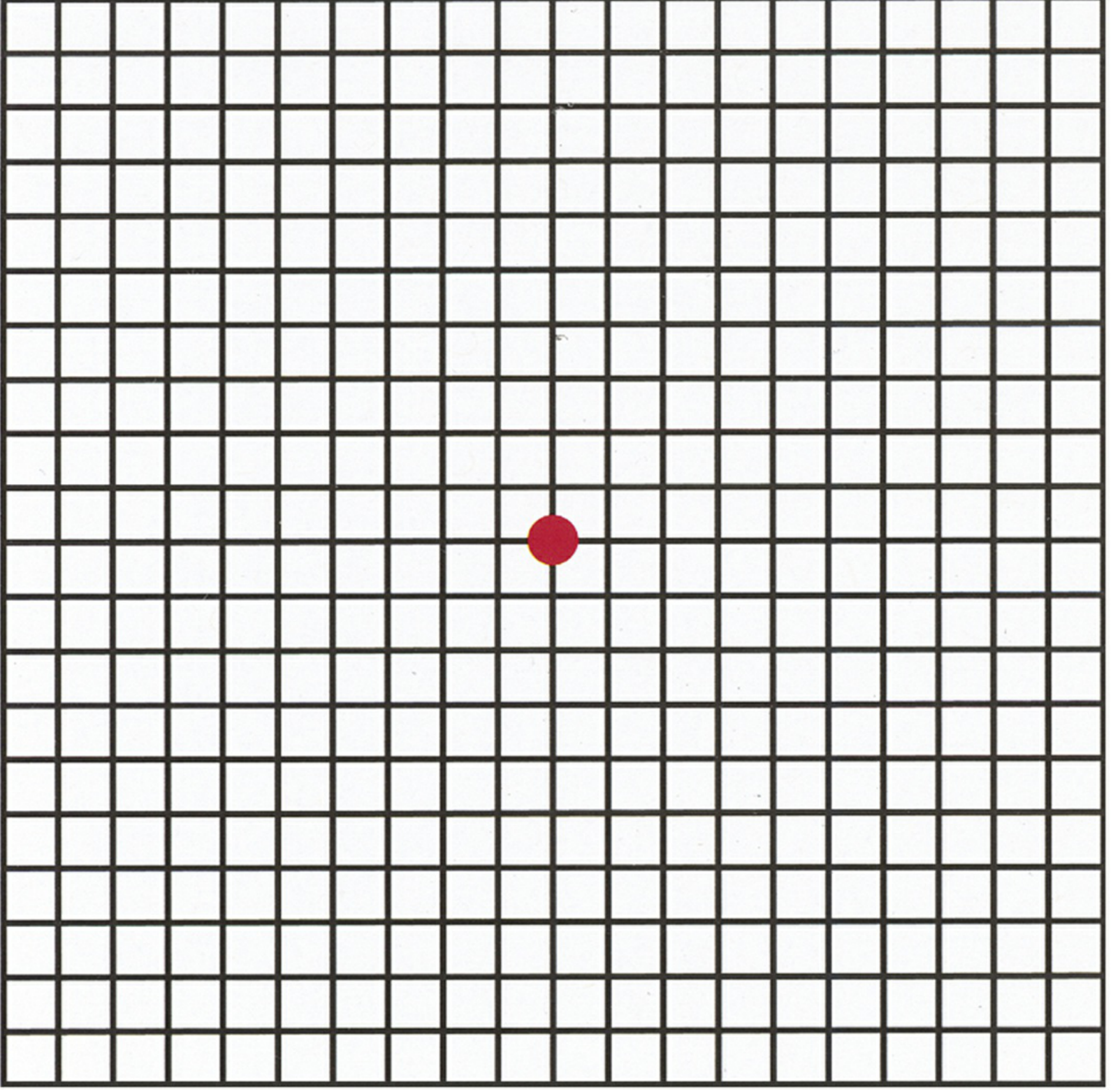
| 2 | Same as Chart 1 with diagonal lines | For patients with central scotoma (aids fixation) |
| 3 | Red squares on black background | Detects subtle colour scotomas, toxic maculopathy, optic neuropathy, chiasmal lesions |
| 4 | Random dots only | Distinguishes scotoma from metamorphopsia (no form to distort) |
| 5 | Horizontal lines | Detects metamorphopsia along specific meridians; useful in reading difficulty |
| 6 | White background, closer lines | More detailed metamorphopsia evaluation |
| 7 | Fine central grid (each square = 0.5°) | More sensitive for subtle central changes |
Technique:
- Pupils not dilated; performed before slit-lamp examination (to avoid photostress effect)
- Appropriate reading correction worn; chart held ~33 cm in good illumination
- One eye covered at a time
- Patient fixates the central dot and reports any distortion, waviness, blurring, or missing areas
- Patient outlines abnormal areas on the grid with a pencil
Interpretation:
- Metamorphopsia (wavy/distorted lines) → macular disease (e.g., AMD, epiretinal membrane, central serous retinopathy)
- Scotoma (missing area) → macular hole, choroidal neovascularisation
- Patients at risk of macular neovascularisation (MNV) should use an Amsler grid at home for regular self-monitoring
2. Photostress Test (Macular Dazzle Test)
A gross test of dark adaptation at the foveal level.
Principle: Bright light bleaches foveal visual pigments, producing a temporary scotoma. Recovery depends on the ability of the retinal pigment epithelium (RPE) and photoreceptors to re-synthesise visual pigment. Since this process is metabolically dependent on RPE function, it is slowed in macular disease but not in optic nerve disease — making it a key differentiating test.
Indications:
- Maculopathy with equivocal ophthalmoscopic signs (e.g., mild cystoid macular oedema, central serous retinopathy)
- Differentiating macular disease from optic neuropathy as the cause of visual loss
Technique:
- Measure best-corrected distance visual acuity (BCVA) first
- Patient fixates on the light of a pen torch or indirect ophthalmoscope held ~3 cm from the eye for ~10 seconds
- Start timing immediately
- Photostress Recovery Time (PSRT) = time taken to read any 3 letters on the pre-test acuity line
- Repeat on the fellow (normal) eye for comparison
Interpretation:
| Finding | PSRT |
|---|---|
| Normal | 15–50 seconds |
| Macular disease | Prolonged (often >50 s, sometimes much longer) |
| Optic neuropathy | Normal / not significantly prolonged |
PSRT is prolonged in macular lesions but not in optic neuropathy — this is the key clinical distinguisher.
3. Light Brightness Comparison Test
Principle: Assesses relative afferent pupillary pathway function and perceived luminance asymmetry.
Technique:
- A bright light is shone into each eye alternately
- Patient rates the brightness in the affected eye relative to the normal eye (scale 1–5)
- In optic neuropathy, the light appears less bright in the affected eye
- Purely macular lesions cause minimal brightness asymmetry
4. Contrast Sensitivity Testing
Tests the ability to detect differences in luminance between an object and its background at various spatial frequencies.
- Assessed using the Pelli-Robson chart (rows of letters of decreasing contrast) or sinusoidal grating patterns
- More sensitive than standard Snellen acuity for detecting subtle macular or optic nerve dysfunction
- Reduced in macular disease, glaucoma, optic neuritis, and media opacity
5. Colour Vision Testing
Though primarily a test of optic nerve and cone function, colour vision tests are relevant to macular assessment:
- Ishihara plates: screen for red-green deficiency; mainly reflect macular function (as noted in Localization in Clinical Neurology)
- Farnsworth-Munsell 100 Hue and D-15: quantify the axis and severity of dyschromatopsia
- Acquired dyschromatopsia (especially red-green or blue-yellow) occurs in macular dystrophies, toxic maculopathy, and optic neuropathy
- Amsler Chart 3 (red squares) specifically targets colour scotomas in the macular region
6. Potential Acuity Meter (PAM) / Laser Interferometry
Used to estimate potential post-operative visual acuity when a cataract or other media opacity obscures the view of the macula.
- Projects a Snellen chart or grating directly onto the retina through a clear portion of the lens
- Useful when cataract surgery is being considered in an eye with possible posterior segment disease
- Limitation: PAM and laser interferometry overestimate visual potential in macular holes, pigment epithelial detachments, and amblyopia
- Near vision testing may be the most accurate method of evaluating macular function when the cataract is not too dense
7. Multifocal Electroretinogram (mfERG)
An electrophysiological test for objective assessment of macular function.
- Records retinal responses simultaneously from multiple locations across the macular region while the patient fixates a central target
- Generates a topographic map of retinal sensitivity across the central ~20–25°
- Detects focal areas of macular dysfunction not visible clinically
- Used in monitoring drug toxicity (e.g., hydroxychloroquine), macular dystrophies, and unexplained central visual loss
Summary Table
| Test | What it Measures | Key Use |
|---|---|---|
| Amsler Grid | Metamorphopsia, scotoma | Macular disease screening & monitoring |
| Photostress (PSRT) | RPE/photoreceptor recovery | Differentiates macular disease from optic neuropathy |
| Light Brightness Comparison | Perceived luminance symmetry | Optic neuropathy detection |
| Contrast Sensitivity | Luminance discrimination | Subtle macular or optic nerve dysfunction |
| Colour Vision | Cone/optic nerve function | Dyschromatopsia, toxic maculopathy |
| PAM / Laser Interferometry | Potential acuity through media opacity | Pre-cataract surgery macular assessment |
| mfERG | Topographic retinal electrical activity | Objective focal macular dysfunction |
Sources: Kanski's Clinical Ophthalmology, 10e; The Wills Eye Manual, 8e; Adams & Victor's Principles of Neurology, 12e; Localization in Clinical Neurology, 8e
Low vision aids in ophthal
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I've used my database query budget. I have enough content from the searches and my medical knowledge to provide a comprehensive answer. Let me synthesize the information now.
Low Vision Aids in Ophthalmology
Low vision is defined as best-corrected visual acuity (BCVA) < 6/18 (20/60) in the better eye, or significant visual field loss, that cannot be corrected by conventional spectacles, contact lenses, or surgery, but in which some useful vision remains. Low vision aids (LVAs) exploit remaining vision to maximise functional independence.
Definition & WHO Classification
| Category | Visual Acuity (Better Eye) |
|---|---|
| Mild low vision | < 6/18 to 6/60 |
| Moderate low vision | < 6/60 to 3/60 |
| Severe low vision | < 3/60 to 1/60 |
| Blindness | < 1/60 or visual field < 10° |
Principles of Low Vision Aids
All LVAs work on one or more of the following principles:
- Magnification — enlarging the retinal image
- Illumination enhancement — improving contrast and reducing glare
- Field expansion — widening the usable visual field
- Non-optical support — adaptive devices and environmental modification
Types of Magnification
| Type | Mechanism | Example |
|---|---|---|
| Relative size magnification | Physically enlarging the object | Large-print books |
| Relative distance magnification | Bringing object closer | Reading closer to the eye |
| Angular magnification | Optical lenses or prisms | Magnifiers, telescopes |
| Electronic magnification | CCTV / digital systems | Closed-circuit TV (CCTV) |
Classification of Low Vision Aids
A. Optical LVAs
1. Spectacle-Mounted (Near) Magnifiers
- High-plus reading spectacles (e.g., +4D to +40D)
- Work on the principle that a higher plus lens brings the focal point closer, effectively magnifying the image
- Both hands are free — ideal for sustained reading tasks
- Must be held at the correct (short) focal distance
- High powers cause reduced field of view and require very close working distance
- Bifocal/prismatic half-eye spectacles: incorporate base-in prisms to compensate for convergence demand at very short reading distances (especially for binocular use)
2. Hand Magnifiers
- Convex lenses mounted in a frame, held by the patient
- Portable, flexible, easy to use — best for spot tasks (price tags, menus)
- Working distance more flexible than spectacle magnifiers
- Require steady hand; can cause fatigue
- Available in powers from ~+4D to +60D
- Illuminated versions available
3. Stand Magnifiers
- Lens mounted on a fixed stand resting on the reading material
- Object-to-lens distance fixed (within the focal length)
- Produce a virtual, magnified, erect image at a finite distance — used with slight plus reading addition
- Hands-free; ideal for tremor, arthritis
- Available in illuminated versions
- Working distance is fixed, limiting use for some tasks
4. Telescopes (Distance LVAs)
- Based on Galilean (concave eyepiece + convex objective) or Keplerian (two convex lenses + erecting prism) designs
- Galilean telescopes: compact, lightweight, erect image without prism; lower magnification (up to ~4×)
- Keplerian telescopes: higher magnification, wider field, but longer and heavier
- Used for distance tasks: watching TV, reading boards, recognising faces
- Bioptic telescopes: mounted in the superior portion of spectacle lenses; patient views through the carrier lens most of the time, tilts head to use the telescope for specific distance tasks
- Reduced field of view; not suitable for mobility
5. Loupe
- Small, single-lens or compound magnifier used close to the eye (like a jeweller's eyeglass)
- High magnification with relatively large field
- Monocular; used for detailed near work
6. Absorptive/Tinted Lenses (Optical Filters)
- Reduce glare and enhance contrast
- Amber/yellow filters improve contrast in low-light conditions
- Useful in conditions like albinism, aniridia, rod dystrophies, and macular degeneration
- NoIR filters, Corning CPF filters: block short-wavelength light; reduce photophobia and improve contrast
B. Electronic / Electro-Optical LVAs
1. Closed-Circuit Television (CCTV) / Video Magnifiers
- Camera projects magnified image on a monitor
- Magnification up to 60× or more
- Adjustable contrast (positive/negative), brightness, and colour
- Large field of view; no need to hold anything steady
- Bulky; not portable (desktop units); expensive
- Portable/handheld video magnifiers now available (e.g., tablet-sized or pocket-sized)
- Ideal for sustained reading tasks
2. Screen Readers / Computer-Based Systems
- Text-to-speech software (e.g., JAWS, NVDA)
- Screen magnification software (e.g., ZoomText)
- Useful for those who need to use computers for work
3. Head-Mounted Displays (HMDs)
- Camera captures scene; displays magnified image on screens within the headset
- Wearable; allows both near and distance magnification
- Examples: eSight, OrCam, NuEyes
- Increasingly sophisticated with AI-based text reading
C. Non-Optical LVAs
These complement optical aids and address daily living needs:
| Aid | Purpose |
|---|---|
| Large-print books, newspapers, watches | Relative size magnification |
| Talking books / audiobooks | Bypass visual reading entirely |
| Talking clocks, calculators, smartphones | Independence in daily tasks |
| Bold-line writing guides | Assist with writing |
| Typoscopes (black card with slit) | Reduce glare; isolate lines of text |
| Reading stands | Maintain correct working distance |
| High-contrast items (dark cup on white mat) | Improve visibility by contrast |
| Tactile markers | Mark appliance controls (cooker, washing machine) |
| Illuminated keyboard / large-print keyboard | Computer access |
D. Lighting and Environmental Modifications
- Adequate, directed illumination is critical — many patients benefit from a flexible-arm reading lamp positioned over the shoulder
- Avoid glare from windows; use anti-glare screens
- Contrast enhancement in home environment (e.g., stair edges, light switches)
Selection of Appropriate LVA
The choice depends on:
| Factor | Consideration |
|---|---|
| Visual acuity | Higher power aids needed for lower acuity |
| Task requirement | Near (reading) vs distance (TV/board) |
| Monocular vs binocular vision | Binocular aids possible for mild loss |
| Visual field defect | Central scotoma → eccentric viewing training; peripheral loss → field expanders |
| Patient age and manual dexterity | Stand magnifiers for elderly/tremor; hand magnifiers for younger |
| Motivation and cognition | Complex devices need training and motivation |
| Lighting needs | Illuminated aids for those with contrast sensitivity loss |
Eccentric Viewing Training
Patients with a central scotoma (e.g., AMD, Stargardt disease) are taught to use a preferred retinal locus (PRL) — an intact para-foveal area used for fixation instead of the damaged fovea. This is trained by low vision specialists and is essential for effective use of optical aids in these patients.
Low Vision Assessment Process
- History — Tasks the patient needs/wants to perform; motivation
- Visual acuity at near and distance (logMAR charts preferred)
- Contrast sensitivity assessment
- Visual field testing (confrontation or Humphrey)
- Refraction — ensure optimal refractive correction first
- Trial of aids — patient tries various aids in clinic
- Prescription and training — patient trained in use at home/work
- Referral — to social services, RNIB (or equivalent), vocational rehabilitation, orientation & mobility training
Common Conditions Requiring LVAs
- Age-related macular degeneration (AMD) — most common in elderly
- Diabetic maculopathy
- Glaucoma (advanced)
- Stargardt disease / other macular dystrophies
- Optic atrophy
- Albinism / aniridia
- Retinitis pigmentosa (field expansion aids particularly useful)
- Amblyopia (in children)
Summary
| Aid Type | Best For | Key Feature |
|---|---|---|
| High-plus spectacles | Sustained near reading | Hands-free |
| Hand magnifier | Spot near tasks | Portable |
| Stand magnifier | Near reading (tremor/arthritis) | Stable, hands-free |
| Galilean telescope | Distance tasks | Lightweight |
| Keplerian telescope | Distance tasks | Higher power |
| CCTV / video magnifier | Sustained reading | Highest magnification, contrast control |
| Tinted/absorptive filters | Glare/photophobia | Contrast enhancement |
| Non-optical aids | Daily living | Auditory, tactile, contrast-based |
Sources: Kanski's Clinical Ophthalmology, 10e; The Wills Eye Manual, 8e
This is a shared conversation. Sign in to Orris to start your own chat.