Anaphylaxis management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced content. Let me compile the full management guide.
Anaphylaxis Management
Algorithm
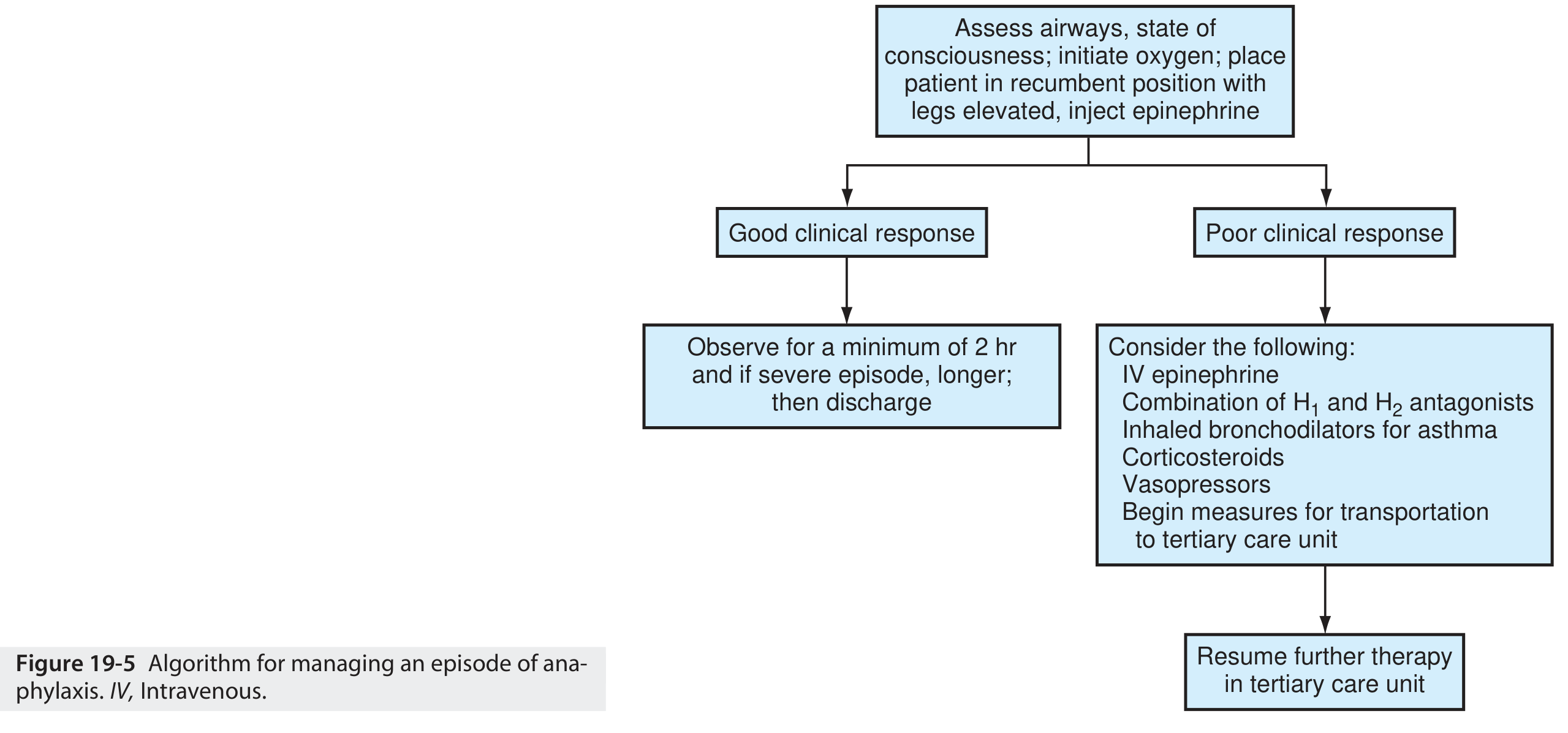
1. Immediate Recognition
Anaphylaxis is a life-threatening systemic reaction of acute onset with multiorgan involvement. The diagnosis is clinical — do not delay treatment waiting for labs.
Key triggers to remove: insect stingers, stop infusing offending medications.
2. First-Line: Epinephrine (No Absolute Contraindications)
Epinephrine is the sole first-line agent. Delay is associated with hypoxic encephalopathy and death. Antihistamines and corticosteroids are adjuncts only — they must never precede or replace epinephrine.
| Patient | Dose | Route |
|---|---|---|
| Adult | 0.3–0.5 mg (0.3–0.5 mL of 1 mg/mL = 1:1000) | IM, lateral thigh (vastus lateralis) |
| Child | 0.01 mg/kg (1:1000 solution), max 0.5 mg | IM, lateral thigh |
- Repeat every 5–10 minutes — up to 30% require more than one dose
- IM thigh provides peak plasma concentration in ~8 min vs. ~34 min for subcutaneous; SC route is no longer recommended
- For refractory/protracted cases: IV epinephrine infusion titrated to BP
- Beta-blocker patients: glucagon 1–5 mg IV bolus over 5 min, then infusion at 5–15 µg/min (reverses refractory bronchospasm and hypotension)
3. Simultaneous Supportive Measures
| Action | Detail |
|---|---|
| Position | Supine with legs elevated (promotes venous return); if vomiting/airway compromise, allow comfortable position with legs elevated; pregnant patients: left lateral decubitus |
| Oxygen | High-flow 100% O₂ via non-rebreather mask |
| IV access | Establish immediately |
| Monitoring | Continuous cardiac monitoring + pulse oximetry |
| IV fluids | Aggressive fluid resuscitation for hypotension (distributive shock) |
4. Airway Management
A priority alongside epinephrine:
- Endotracheal intubation may be needed
- If laryngeal edema is not rapidly responsive to epinephrine → cricothyroidotomy or tracheotomy
- Inhaled β-agonists (e.g., salbutamol) for persistent bronchospasm
5. Second- and Third-Line Adjuncts
These are adjuncts only and must not delay or replace epinephrine:
| Drug | Dose / Route | Role |
|---|---|---|
| H1 antihistamine (diphenhydramine) | 25–50 mg IV/IM | Relieves urticaria/pruritus; no effect on hemodynamics |
| H2 antihistamine (ranitidine/famotidine) | IV | Used in combination with H1 blocker |
| Corticosteroids (methylprednisolone/hydrocortisone) | IV | May prevent biphasic reaction; limited acute benefit due to slow onset |
| Inhaled bronchodilator | Nebulized salbutamol | Refractory bronchospasm |
| Glucagon | 1–5 mg IV bolus, then 5–15 µg/min infusion | Patients on beta-blockers |
| Vasopressors (norepinephrine, vasopressin) | IV | Refractory hypotension despite epinephrine and fluids |
6. Biphasic Anaphylaxis
A second wave of symptoms can occur 1–72 hours after the initial reaction (typically within 8 hours) without re-exposure to the trigger. Incidence is ~5%. Risk factors include:
- Protracted initial reaction
- Hypotension or airway involvement
- Unknown trigger
- Receiving IV epinephrine or >1 dose of IM epinephrine
- Poor outpatient social support
7. Observation and Disposition
| Scenario | Recommendation |
|---|---|
| Good response to single IM epi | Observe minimum 2–4 hours |
| Severe episode, airway involvement, hypotension | Observe >4–8 hours or admit |
| IV epinephrine or >1 IM dose required | Strong consideration for admission |
| Protracted/unknown trigger/poor social support | Admit |
8. Discharge Instructions
All patients discharged after anaphylaxis must receive:
- Prescription for self-injectable epinephrine (EpiPen) × 2 devices — with demonstrated training
- Written emergency action plan
- Allergen avoidance counseling
- Referral to allergist/immunologist for formal evaluation, trigger identification (skin testing, specific IgE), and consideration of immunotherapy
Diagnostic Notes
- Anaphylaxis remains a clinical diagnosis
- Serum tryptase: peaks at ~1 hour, detectable up to 4 hours — most useful in hymenoptera-induced cases (may be normal in food-induced)
- Serum histamine: peaks within 1 hour
- Labs are not required before treatment
— ROSEN's Emergency Medicine: Concepts and Clinical Practice; The Washington Manual of Medical Therapeutics
Anaphylaxis
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
anaphylaxis pathophysiology IgE mast cell mediators
I have rich, comprehensive material from multiple authoritative sources. Let me compile the full guide.
Anaphylaxis — Comprehensive Overview
Definition
Anaphylaxis is a life-threatening, systemic hypersensitivity reaction of acute onset with multiorgan involvement. It arises when mast cells and basophils secrete potent mediators affecting vasculature, smooth muscle, mucous glands, and nerves. The principal target organs are the cardiovascular, cutaneous, respiratory, and gastrointestinal systems — where mast cells are most abundant.
— Goldman-Cecil Medicine
Epidemiology
- Lifetime incidence in adults: 2–8%; higher in children (food allergy is more prevalent)
- ~1,500–2,000 deaths/year in the United States
- Fatal anaphylaxis is rare (<1% of cases), but medication-induced fatalities are rising
- ~50% of reactions occur at home; 15% at a medical facility
- Only ~30% of patients receive epinephrine in the prehospital setting; 50–70% receive it in the ED
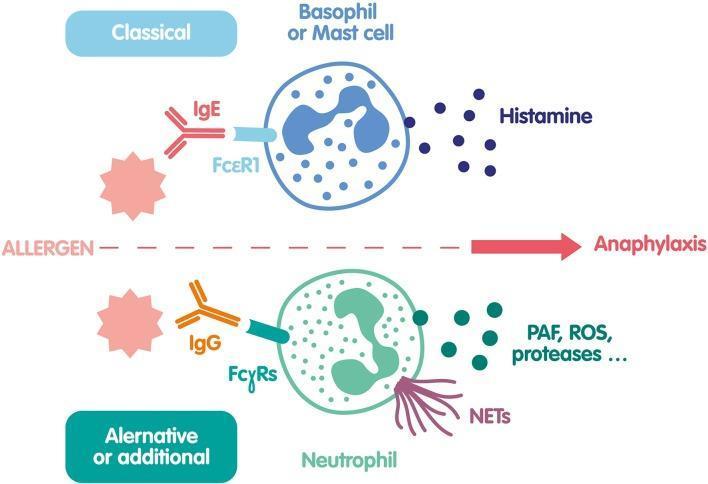
Pathophysiology
Classical (IgE-Mediated) Pathway
- Sensitization: Initial allergen exposure → antigen-presenting cells activate Th2 lymphocytes → IL-4/IL-13 drive B-cell class switching → allergen-specific IgE produced
- Sensitized state: IgE binds high-affinity receptors (FcεRI) on mast cells and basophils — patient is now sensitized
- Re-exposure: Multivalent allergen cross-links IgE–FcεRI complexes → receptor aggregation → mast cell degranulation
- Mediator release:
- Pre-formed (immediate): histamine, tryptase, chymase, heparin
- Newly synthesized (minutes): prostaglandin D₂, leukotriene C₄, platelet-activating factor (PAF)
- Late-phase (hours): cytokines/chemokines (IL-4, IL-5, IL-13, TNF-α)
Non-IgE-Mediated (Anaphylactoid) Pathway
Direct mast cell activation without prior sensitization:
- NSAIDs/aspirin: arachidonic acid pathway disruption → excess leukotrienes
- Radiocontrast media, opioids, vancomycin: direct mast cell degranulation (complement activation or MRGPRX2 receptor)
- Complement activation (C3a, C5a → anaphylatoxins) — can trigger identical clinical picture
Net Effect of Mediators
| Mediator | Effect |
|---|---|
| Histamine | Vasodilation, increased vascular permeability, bronchospasm, urticaria |
| Leukotrienes (C₄, D₄) | Potent bronchospasm, mucus secretion |
| Prostaglandin D₂ | Bronchospasm, vasodilation |
| PAF | Bronchospasm, hypotension, neutrophil activation |
| Tryptase | Marker of mast cell activation (diagnostic use) |
Triggers (Causes)
IgE-Mediated
| Category | Examples |
|---|---|
| Foods (most common overall, esp. children) | Peanuts, tree nuts, shellfish, fish, milk, eggs, soy; alpha-gal (mammalian meat after tick bite — delayed 3–6 h) |
| Drugs (most common in adults; highest fatality) | Beta-lactam antibiotics (penicillin = most common antibiotic cause), NMBAs, chemotherapy, monoclonal antibodies |
| Insect stings | Hymenoptera (wasps, bees, ants); 1–3% of stings cause anaphylaxis |
| Latex | Especially patients with multiple surgeries, healthcare workers |
| Allergen immunotherapy | Subcutaneous injections |
Non-IgE-Mediated
| Category | Examples |
|---|---|
| NSAIDs/aspirin | Most common trigger in EDs (COX-1 inhibition pathway) |
| Radiocontrast media | Direct mast cell activation |
| Opioids, vancomycin | Direct degranulation |
| Exercise-induced | Often food + exercise co-trigger |
| Idiopathic | No identifiable cause found |
Note on penicillin: <10% of those with a reported penicillin allergy are truly allergic on skin testing. Cross-reactivity with cephalosporins exists but is low (1–8%).
Risk Factors for Severity and Mortality
- Extremes of age (infants: under-recognition; elderly: reduced physiologic reserve)
- Cardiovascular disease, asthma, mastocytosis
- Beta-blocker or ACE inhibitor use (blunts epinephrine response; ACE inhibitors impair bradykinin degradation)
- Hereditary α-tryptasemia (increased mast cell burden; present in ~5% of population)
- Upright posture at symptom onset (reduces venous return — "empty ventricle" syndrome → cardiac arrest)
- Delayed epinephrine administration
- Previous anaphylactic episode
Clinical Features
Symptoms typically occur within minutes of exposure (more rapid = more severe); food reactions may be delayed up to 30 min, alpha-gal reactions 3–6 hours.
| System | Manifestations |
|---|---|
| Cutaneous (most common, ~90%) | Urticaria, angioedema, flushing, pruritus |
| Respiratory | Throat tightness, stridor (laryngeal edema), bronchospasm, wheezing, hypoxia |
| Cardiovascular | Hypotension, tachycardia, distributive shock, arrhythmia |
| GI | Nausea, vomiting, diarrhea, cramping |
| Neurological | Anxiety, altered consciousness, seizure, syncope |
Absence of skin findings does not exclude anaphylaxis — and these cases (no urticaria/flushing) are associated with higher fatality.
Diagnostic Criteria (NIAID/FAAN)
Anaphylaxis is likely if any one of three criteria is met:
- Acute onset of skin/mucosal involvement PLUS respiratory compromise or hypotension
- Two or more of the following after allergen exposure: skin/mucosal involvement, respiratory compromise, hypotension, persistent GI symptoms
- Hypotension alone after exposure to a known allergen for that patient
Diagnosis
Primarily clinical — do not delay treatment for labs.
- Serum tryptase: peaks ~1 hour after onset, detectable up to 4 hours; best yield in hymenoptera-induced; may be normal in food-induced anaphylaxis
- Serum histamine: peaks within 1 hour (narrow window)
- Specific IgE / skin testing: performed after the acute episode, not in the acute setting
Differential Diagnosis
- Vasovagal syncope (bradycardia; no urticaria/angioedema)
- Flushing syndromes: carcinoid, red-man syndrome, pheochromocytoma
- Non-histaminergic angioedema: hereditary angioedema (HAE), ACE inhibitor-induced angioedema
- Airway obstruction: epiglottitis, foreign body, croup
- Other shock states: cardiogenic, septic, hemorrhagic
- Panic attack, vocal cord dysfunction
Management
Algorithm
Step 1 — Immediate Actions (Simultaneous)
- Remove/stop the trigger (stop infusion, remove stinger)
- Call for help; activate emergency response
- Position: supine + legs elevated; if vomiting/airway compromise → comfortable position; pregnancy → left lateral decubitus
- IV access, continuous cardiac monitoring + pulse oximetry
- High-flow 100% oxygen
Step 2 — Epinephrine (First-Line, No Absolute Contraindications)
| Patient | Dose | Route |
|---|---|---|
| Adult | 0.3–0.5 mg of 1 mg/mL (1:1000) | IM — lateral thigh (vastus lateralis) |
| Child | 0.01 mg/kg, max 0.5 mg, of 1:1000 | IM — lateral thigh |
- Repeat every 5–10 min (up to 30% need >1 dose)
- IM lateral thigh: peak plasma in ~8 min vs. ~34 min subcutaneously — SC route no longer recommended
- There are no absolute contraindications to epinephrine in anaphylaxis
Step 3 — Fluids
- Aggressive IV crystalloid bolus for hypotension/distributive shock
Step 4 — Refractory Cases
| Situation | Intervention |
|---|---|
| Persistent hypotension after ≥2 IM doses + fluids | IV epinephrine infusion: 1 µg/mL concentration; adults 1–10 µg/min, titrated; central access preferred (extravasation risk) |
| Beta-blocker patient (epinephrine resistance) | Glucagon 1–5 mg IV over 5 min → infusion 5–15 µg/min |
| Ongoing bronchospasm | Nebulized albuterol 2.5 mg ± ipratropium 0.5 mg |
| Vasopressor-dependent shock | Norepinephrine, vasopressin, dopamine, phenylephrine |
| Laryngeal edema not responding to epi | Cricothyroidotomy or tracheotomy |
Step 5 — Adjuncts (Second/Third Line — Do NOT Delay Epinephrine)
| Drug | Adult Dose | Purpose |
|---|---|---|
| Diphenhydramine (H1) | 50 mg IV/IM | Urticaria, pruritus — no hemodynamic benefit |
| Famotidine (H2) | 40 mg IV | Adjunct to H1 blocker |
| Methylprednisolone | 125–250 mg IV | Possible prevention of biphasic reaction; no acute benefit |
| Prednisone (discharge) | 40–60 mg oral | Continued steroid coverage |
Biphasic Reaction
- A second anaphylactic wave without re-exposure, occurring 1–72 hours after resolution (most within 8 hours)
- Incidence ~5%
- More likely with: protracted initial reaction, hypotension, airway involvement, unknown trigger, delayed epinephrine, >1 epi dose required
Disposition
| Scenario | Observation |
|---|---|
| Single IM epi, rapid good response | Minimum 2–4 hours |
| Severe episode (airway, hypotension) | >4–8 hours, consider admission |
| IV epi or >1 IM epi required | Admit |
| Unknown trigger, poor social support | Admit |
Discharge Planning
Every patient discharged after anaphylaxis must receive:
- Self-injectable epinephrine (EpiPen) × 2 devices + demonstrated training on use
- Written emergency action plan
- Allergen avoidance education
- Referral to allergist/immunologist for:
- Skin testing / specific IgE to identify trigger
- Consideration of allergen immunotherapy (especially venom-induced)
Special Situations
Hereditary Angioedema (non-histaminergic — does NOT respond to epi/antihistamines)
Bradykinin-mediated; treat with:
| Drug | Mechanism | Dose |
|---|---|---|
| Berinert (C1-INH, human) | C1 inhibitor replacement | 20 units/kg IV |
| Ruconest (C1-INH, recombinant) | C1 inhibitor replacement | 50 units/kg IV |
| Ecallantide | Kallikrein inhibitor | 30 mg SC |
| Icatibant | Bradykinin B₂ receptor antagonist | 30 mg SC |
| Fresh frozen plasma | Contains C1-INH | Variable |
ACE Inhibitor–Induced Angioedema
- Bradykinin-mediated (impaired degradation)
- Treatment mainly supportive; consider HAE agents if airway threatened
— ROSEN's Emergency Medicine: Concepts and Clinical Practice | Goldman-Cecil Medicine | The Washington Manual of Medical Therapeutics
Anaphylaxis
Asking for Preferences
Here's the full overview from the previous session — no need to re-query the textbooks since the content is unchanged:
Anaphylaxis — Comprehensive Overview
Definition
Anaphylaxis is a life-threatening, systemic hypersensitivity reaction of acute onset with multiorgan involvement. It arises when mast cells and basophils secrete potent mediators affecting vasculature, smooth muscle, mucous glands, and nerves. The principal target organs are the cardiovascular, cutaneous, respiratory, and gastrointestinal systems.
Epidemiology
- Lifetime incidence in adults: 2–8%
- ~1,500–2,000 deaths/year in the United States; foods and insect stings each account for ~100 deaths/year
- Fatal anaphylaxis is rare (<1% of cases)
- ~50% of reactions occur at home; 15% at a medical facility
- Only ~30% of patients receive epinephrine prehospital; 50–70% receive it in the ED
Pathophysiology
Classical — IgE-Mediated
- Sensitization: Allergen exposure → Th2 activation → B-cell class switching → allergen-specific IgE produced and bound to FcεRI on mast cells/basophils
- Re-exposure: Multivalent allergen cross-links IgE–FcεRI → receptor aggregation → mast cell degranulation
- Mediator release:
| Wave | Mediators | Onset |
|---|---|---|
| Pre-formed | Histamine, tryptase, heparin | Immediate (seconds) |
| Newly synthesized | Prostaglandin D₂, leukotriene C₄, PAF | Minutes |
| Late-phase | IL-4, IL-5, IL-13, TNF-α | Hours |
Non-IgE-Mediated (Anaphylactoid)
Direct mast cell activation without prior sensitization — clinically identical:
- NSAIDs/aspirin: COX-1 inhibition → arachidonic acid shunting → excess leukotrienes
- Radiocontrast media, opioids, vancomycin: direct MRGPRX2 receptor activation or complement (C3a/C5a)
- Exercise-induced: often requires co-trigger (food)
Net Mediator Effects
| Mediator | Systemic Effect |
|---|---|
| Histamine | Vasodilation, ↑ vascular permeability, bronchospasm, urticaria |
| Leukotrienes (C₄, D₄) | Potent bronchospasm, mucus hypersecretion |
| Prostaglandin D₂ | Bronchospasm, vasodilation |
| PAF | Bronchospasm, hypotension, neutrophil activation |
| Tryptase | Diagnostic marker of mast cell activation |
Triggers
IgE-Mediated
| Category | Key Examples |
|---|---|
| Foods (most common overall, esp. children) | Peanuts, tree nuts, shellfish, fish, milk, eggs; alpha-gal (mammalian meat — delayed 3–6 h after tick bite) |
| Drugs (leading cause in adults; highest fatality rate) | Penicillin (most common antibiotic), NMBAs, chemotherapy, monoclonal antibodies |
| Insect stings | Hymenoptera (bees, wasps, ants); anaphylaxis in 1–3% of stings |
| Latex | Multiple surgical exposures; healthcare workers |
Non-IgE-Mediated
| Category | Key Examples |
|---|---|
| NSAIDs/aspirin | Most common ED drug trigger |
| Radiocontrast media | Most common hospital trigger alongside antibiotics |
| Opioids, vancomycin | Direct degranulation |
| Idiopathic | No identifiable cause |
Penicillin allergy is over-reported — <10% of patients with a reported history are truly allergic on skin testing.
Risk Factors for Severity & Mortality
- Beta-blocker or ACE inhibitor use (epinephrine resistance; impaired bradykinin clearance)
- Asthma, mastocytosis, hereditary α-tryptasemia (~5% of population)
- Extremes of age; cardiovascular disease
- Upright posture at onset → reduced venous return → "empty ventricle" cardiac arrest
- Delayed epinephrine, previous anaphylactic episode
- Unknown trigger
Clinical Features
Onset typically within minutes; more rapid = more severe. Alpha-gal reactions delayed 3–6 h.
| System | Manifestations |
|---|---|
| Cutaneous (~90%) | Urticaria, angioedema, flushing, pruritus |
| Respiratory | Throat tightness, stridor (laryngeal edema), wheezing, bronchospasm, hypoxia |
| Cardiovascular | Hypotension, tachycardia, distributive shock, arrhythmia |
| GI | Nausea, vomiting, diarrhea, cramping |
| Neurological | Anxiety, dizziness, altered consciousness, syncope |
Absence of skin findings does not exclude anaphylaxis — and cases without urticaria carry higher fatality.
Diagnostic Criteria (NIAID/FAAN)
Anaphylaxis is likely if any one of three criteria is met:
- Acute onset of skin/mucosal involvement + respiratory compromise or hypotension
- Two or more of: skin/mucosal involvement, respiratory compromise, hypotension, persistent GI symptoms — after allergen exposure
- Hypotension alone after exposure to a known allergen for that patient
Labs
- Serum tryptase: peaks ~1 h, detectable up to 4 h; best for hymenoptera-induced; may be normal in food-induced
- Serum histamine: peaks within 1 h (narrow window)
- Labs are never required before starting treatment
Differential Diagnosis
- Vasovagal syncope (bradycardia, no urticaria)
- Non-histaminergic angioedema: HAE, ACE inhibitor–induced
- Flushing syndromes: carcinoid, pheochromocytoma, red-man syndrome
- Airway obstruction: epiglottitis, foreign body
- Other shock states: cardiogenic, septic, hemorrhagic
- Panic attack, vocal cord dysfunction
Management
Algorithm
Step 1 — Simultaneous Immediate Actions
- Remove/stop the trigger
- Supine + legs elevated (left lateral decubitus if pregnant)
- IV access, cardiac monitoring, pulse oximetry
- High-flow 100% O₂
Step 2 — Epinephrine (First-Line; No Absolute Contraindications)
| Patient | Dose | Route |
|---|---|---|
| Adult | 0.3–0.5 mg of 1:1000 (1 mg/mL) | IM — lateral thigh (vastus lateralis) |
| Child | 0.01 mg/kg, max 0.5 mg | IM — lateral thigh |
- Repeat every 5–10 min — up to 30% need >1 dose
- IM lateral thigh: peak plasma ~8 min vs. ~34 min SC — SC route no longer recommended
- Antihistamines and corticosteroids must never precede or replace epinephrine
Step 3 — IV Fluids
- Aggressive crystalloid bolus for hypotension
Step 4 — Refractory Management
| Situation | Intervention |
|---|---|
| Persistent hypotension after ≥2 IM doses + fluids | IV epinephrine infusion: 1 µg/mL; adults 1–10 µg/min, titrated (central access preferred) |
| Beta-blocker patient | Glucagon 1–5 mg IV over 5 min → 5–15 µg/min infusion |
| Bronchospasm | Nebulized albuterol 2.5 mg ± ipratropium 0.5 mg |
| Vasopressor-dependent | Norepinephrine, vasopressin, dopamine |
| Laryngeal edema not responding | Cricothyroidotomy or surgical airway |
Step 5 — Adjuncts (Do NOT delay epinephrine for these)
| Drug | Adult Dose | Role |
|---|---|---|
| Diphenhydramine (H1) | 50 mg IV/IM | Urticaria/pruritus — no hemodynamic benefit |
| Famotidine (H2) | 40 mg IV | Adjunct to H1 |
| Methylprednisolone | 125–250 mg IV | Possible biphasic prevention; no acute benefit |
Biphasic Anaphylaxis
- Second reaction without re-exposure, occurring 1–72 hours after initial resolution (most within 8 h)
- Incidence ~5%
- Higher risk with: protracted initial episode, hypotension or airway involvement, unknown trigger, >1 epinephrine dose, delayed initial treatment
Disposition
| Scenario | Recommendation |
|---|---|
| Good response to single IM epi | Observe minimum 2–4 hours |
| Severe episode (airway/hypotension) | Observe >4–8 hours or admit |
| IV epi or >1 IM dose required | Admit |
| Unknown trigger or poor social support | Admit |
Discharge Planning
All discharged patients must receive:
- Self-injectable epinephrine (EpiPen) ×2 + training
- Written emergency action plan
- Allergen avoidance counseling
- Referral to allergist/immunologist (skin testing, specific IgE, possible immunotherapy)
Special Topic: Non-Histaminergic Angioedema (HAE)
Does not respond to epinephrine or antihistamines (bradykinin-mediated):
| Drug | Mechanism | Dose |
|---|---|---|
| Berinert (C1-INH, human) | C1 inhibitor replacement | 20 units/kg IV |
| Ruconest (C1-INH, recombinant) | C1 inhibitor replacement | 50 units/kg IV |
| Ecallantide | Kallikrein inhibitor | 30 mg SC |
| Icatibant | Bradykinin B₂ receptor antagonist | 30 mg SC |
| FFP | Contains C1-INH | Variable |
— ROSEN's Emergency Medicine | Goldman-Cecil Medicine | The Washington Manual of Medical Therapeutics
Heat stroke
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent — I have comprehensive content. Let me now synthesize the full guide.
Heat Stroke — Comprehensive Overview
Definition
Heat stroke is an acute, life-threatening emergency defined by the triad of:
- Core temperature >40°C (>104°F)
- Central nervous system dysfunction (altered mental status, seizures, coma)
- Multiorgan involvement
It is fatal if untreated. A delay in cooling directly increases mortality.
Classification: Two Types
| Feature | Classic (Non-Exertional) Heat Stroke (CHS) | Exertional Heat Stroke (EHS) |
|---|---|---|
| Population | Elderly, debilitated, fixed-income, psychiatric patients | Young, healthy — athletes, military recruits |
| Mechanism | Passive exposure (heat waves, poor ventilation, no AC) | Endogenous heat overproduction exceeds dissipation |
| Sweating | Absent in most | Present in ~50% |
| CVP | Usually elevated; high-output cardiac failure | Variable |
| Rhabdomyolysis | Rare | Common |
| Hypoglycemia | Uncommon | Common (↑ glucose metabolism + hepatic damage) |
| Coagulopathy/DIC | Present | Common |
| Pulmonary edema | May be present | Less common |
| Acid-base | Respiratory alkalosis | Lactic acidosis |
Pathophysiology
- Heat generation overwhelms heat dissipation (radiation, conduction, convection, evaporation)
- Core temperature rises → direct cellular thermotoxicity to brain, liver, kidneys, endothelium
- Cerebellum is highly sensitive to heat (ataxia is an early sign)
- High temperature → endothelial injury → DIC cascade, increased vascular permeability, capillary leak
- Liver: centrilobular necrosis (enzyme peaks 24–72 h after insult; usually reversible)
- Rhabdomyolysis (especially EHS) → myoglobinuria → acute renal failure
- Neurologic injury is proportional to peak temperature × duration of exposure
Cardiovascular Effects
- Hyperdynamic circulation: tachycardia (up to 180 bpm), low peripheral vascular resistance, high cardiac output
- Skin vasodilation to dissipate heat → elevated CVP with right-sided cardiac dilation → high-output heart failure
- Hypotension in severe cases
Risk Factors & Precipitating Medications
Patient risk factors:
- Advanced age, extremes of age
- Cardiovascular disease, diabetes, obesity
- Prior heat illness, dehydration, skin disorders (reduced sweating)
- Alcohol/drug use
- Acclimatization failure
Medications that impair heat tolerance:
| Drug Class | Examples |
|---|---|
| Anticholinergics | Atropine, oxybutynin, scopolamine, benztropine |
| Antipsychotics (all) | Haloperidol, chlorpromazine |
| Antidepressants | Tricyclics |
| Antihistamines (all) | |
| Diuretics | Furosemide, HCTZ, spironolactone |
| Antihypertensives | Beta-blockers, calcium channel blockers |
| Sympathomimetics | Amphetamines, cocaine, methylphenidate |
| Antiepileptics | Topiramate, zonisamide |
| Ergogenic aids | Anabolic steroids, creatine, ephedra |
Clinical Features
Cardinal features (both required):
- Core temperature >40°C (>104°F)
- CNS dysfunction — can range from confusion, irritability, bizarre behaviour, hallucinations, ataxia → combativeness, seizures, decerebrate posturing, coma
Other features:
- Tachycardia (up to 180 bpm), hypotension
- Hot skin — absence of sweating is not a required criterion (sweating present in >50% of cases)
- Tachypnoea, hyperventilation → pCO₂ often <20 mmHg
- Signs of end-organ damage: jaundice, oliguria, bleeding
Note: Ataxia is an early neurologic sign due to cerebellar heat sensitivity.
Diagnosis
Primarily clinical — diagnosis based on history, presentation, and exclusion of other causes. No diagnostic test confirms heat stroke.
Workup (directed at end-organ damage & excluding differentials)
- CBC — thrombocytopenia (DIC)
- CMP — electrolytes (hypo/hypernatremia, hypokalemia, hyperkalemia in ARF), glucose, LFTs (centrilobular necrosis), creatinine
- ABG — respiratory alkalosis; lactic acidosis in EHS
- Coagulation panel (PT/PTT/fibrinogen) — DIC
- CPK + myoglobin — rhabdomyolysis
- Urinalysis — myoglobinuria, proteinuria
- ECG — arrhythmia
- CT head / LP — to exclude meningitis, CVA, intracranial haemorrhage if diagnosis unclear
Differential Diagnosis
| Category | Examples |
|---|---|
| Infection | Sepsis, meningitis, encephalitis, malaria, typhoid, tetanus |
| Neurologic | Hypothalamic haemorrhage/infarct, CVA, status epilepticus |
| Endocrine | Thyroid storm, phaeochromocytoma, DKA |
| Toxicologic | Anticholinergic toxidrome, sympathomimetic OD, salicylate OD, serotonin syndrome, malignant hyperthermia, neuroleptic malignant syndrome, alcohol/benzodiazepine withdrawal |
Management
Prehospital
- Remove from hot environment immediately
- Remove clothing
- Check point-of-care glucose
- Begin cooling (spray water + fan, or wet towels/ice packs)
- IV normal saline bolus 1–2 L if hypotensive
- Transport urgently
ED Resuscitation
Primary goal: Immediate cooling to ≤39°C (102.2°F)
A delay in cooling = increased mortality. Cooling and resuscitation occur simultaneously.
- Standard ABCs — airway management, oxygen
- IV access × 2, continuous monitoring
- Electronic rectal thermometer / oesophageal thermometer / urinary catheter thermistor for accurate core temperature monitoring
- IV fluids: rate titrated to maintain adequate urine output; use invasive monitoring in elderly/cardiac patients
- Check glucose — treat hypoglycaemia
Cooling Techniques
Target: Reduce core temperature to ~39°C (102.2°F) — stop cooling at this point to avoid hypothermic overshoot. No single method is proven superior.
| Method | Description | Advantages | Disadvantages |
|---|---|---|---|
| Evaporative cooling | Spray cool water (~15°C) on body + fan | Practical, effective, good patient access, widely available | Shivering in low humidity; ECG electrode adhesion problems |
| Ice water immersion | Place undressed patient in ice water tub covering trunk + extremities | Highly effective (especially EHS); well-documented | Shivering, displaced monitoring leads, unable to defibrillate, need large tub |
| Ice packs to groin/axillae/neck | Applied to high-flow vascular areas | Readily available | Less efficient alone |
| Cold IV fluids | 4°C normal saline | Adjunct; easily available | Limited cooling capacity alone |
| Intravascular cooling catheters | Endovascular heat exchange | Precise temperature control | Invasive, limited availability |
| Peritoneal/gastric lavage | Cold fluids via NG or peritoneal catheter | Reserve for refractory cases | Invasive |
Shivering management (which counterproduces heat):
- First-line: short-acting benzodiazepines
- Second-line: phenothiazines (use cautiously — lower seizure threshold, anticholinergic effects impair sweating, cause hypotension)
Managing Complications
Hypotension
- First: IV fluid bolus 20 mL/kg
- If CVP reaches 12–14 mmHg and hypotension persists → dopamine or dobutamine
- Avoid norepinephrine (α-adrenergic vasoconstriction redirects blood away from skin → impairs cooling)
Seizures
- Benzodiazepines (first-line)
- Cooling itself reduces seizure threshold
- Barbiturates (phenobarbital) for refractory seizures
Rhabdomyolysis / Renal Failure
- Aggressive IV fluid hydration
- Target urine output >1 mL/kg/hr (>200–300 mL/hr)
- Alkalinise urine with sodium bicarbonate (controversial) to prevent myoglobin precipitation
- Dialysis for severe ARF
DIC / Coagulopathy
- FFP, cryoprecipitate, platelets as indicated
- Treat underlying heat stroke (cooling is primary therapy)
Complications Summary Table
| Timing | System | Complication |
|---|---|---|
| Early | Neurologic | Delirium, coma, seizures |
| Cardiovascular | Hypotension, heart failure | |
| Metabolic | Hypokalemia, hypernatremia, hyponatremia | |
| Muscular | Rhabdomyolysis | |
| Renal | Oliguria | |
| Pulmonary | Pulmonary oedema | |
| Late | Neurologic | Cerebral oedema, encephalopathy, persistent neurologic deficit |
| Cardiac | Myocardial injury | |
| Renal | ARF | |
| GI | Intestinal ischaemia, hepatic dysfunction, pancreatitis | |
| Haematologic | Thrombocytopenia, DIC | |
| Metabolic | Hyperkalemia (ARF), hypocalcaemia, hyperuricaemia |
Prognosis
Poor outcome predictors:
- Hypotension on arrival
- Altered coagulation
- Lactic acidosis
- Need for endotracheal intubation on arrival
- Advanced age
- Delayed cooling
Persistent neurologic deficits can occur even after successful cooling. Hepatic injury is almost always reversible.
Prevention
- Acclimatisation (10–14 days of gradual heat exposure)
- Adequate hydration before and during exertion
- Avoid exercise during peak heat hours
- Light-coloured, loose-fitting clothing
- Awareness of high-risk medications (see table above)
- Cooling stations and buddy systems in high-risk settings (military, endurance sports, elderly in heatwaves)
— Tintinalli's Emergency Medicine: A Comprehensive Study Guide | ROSEN's Emergency Medicine: Concepts and Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.