Tb meningitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of tuberculous (TB) meningitis based on authoritative neurology and clinical textbooks.
Tuberculous Meningitis
Epidemiology & Risk Factors
TB meningitis parallels systemic tuberculosis in incidence. In the US, cases declined markedly post-WWII but increased ~16% annually after 1985, largely driven by HIV. Among patients with full-blown HIV, the incidence of tuberculosis is almost 500 times that of the general population. In developing countries (sub-Saharan Africa, Asia, India), tuberculosis is ~25 times more frequent than in the US. High-risk groups include:
- HIV-positive individuals
- Alcoholics
- Immigrants from high-prevalence regions (Asia, Africa, India, former Soviet Union)
- Children (historically)
— Adams and Victor's Principles of Neurology, 12th Edition
Causative Organism
Primarily Mycobacterium tuberculosis. Rarely: M. bovis, M. avian, M. kansasii, M. fortuitum (the latter post-neurosurgical procedures). HIV has increased cases caused by atypical mycobacteria.
Pathogenesis
Two stages:
- Hematogenous seeding of the meninges and subpial brain regions → formation of tubercles (granulomas)
- Rupture of tubercles → discharge of bacteria into the subarachnoid space → inflammatory cascade
The process is not confined to the subarachnoid space — it frequently invades the underlying brain, making this a true meningoencephalitis.
— Adams and Victor's Principles of Neurology, 12th Edition
Pathological Findings
- Basal exudate: thick, gelatinous exudate at the base of the brain — obliterates pontine and interpeduncular cisterns, extends to optic chiasm, medulla, floor of third ventricle, and temporal lobes
- Microscopy: central caseation surrounded by epithelioid cells, giant cells, lymphocytes, plasma cells, and connective tissue
- Cranial nerve involvement: far more common than in typical bacterial meningitis, due to involvement as nerves traverse the inflamed subarachnoid space
- Vascular involvement: arteritis → occlusion → brain infarction
- Hydrocephalus: from blockage of basal cisterns (most common) or ependymitis blocking the aqueduct/4th ventricle
- Spinal cord: exudate can surround the cord → multiple radiculopathies, cord compression
Clinical Features
Onset: Subacute — evolving over 1–2 weeks (slower than bacterial meningitis)
Early symptoms:
- Fever (low-grade)
- Malaise
- Headache (>50% of cases)
- Lethargy, confusion
- Stiff neck (75% of cases), Kernig and Brudzinski signs
Later/advanced features:
- Cranial nerve palsies (20% at presentation) — typically ocular palsies (CN III, VI), facial palsy, deafness
- Papilledema (raised ICP)
- Focal neurologic deficits from hemorrhagic infarction
- Hypothermia, hyponatremia (SIADH or adrenal tuberculosis)
- Seizures (especially in children)
Systemic TB: In ~2/3 of patients, active TB is found elsewhere — most often lungs, occasionally small bowel, bone, kidney, or ear.
Untreated course: Progressive confusion → stupor → coma → decerebrate posturing → death in 4–8 weeks
British Medical Research Council (MRC) Staging
| Stage | Description |
|---|---|
| I | GCS 15, no focal signs |
| II | GCS 11–14, OR mild focal signs |
| III | GCS ≤10, OR dense focal deficits |
CSF Findings (Lumbar Puncture)
| Parameter | Finding |
|---|---|
| Pressure | Elevated |
| Cells | 50–500/mm³, lymphocytic predominance (PMNs early, then lymphocytes) |
| Protein | Elevated — typically 100–200 mg/dL, higher if spinal block |
| Glucose | Reduced (<40 mg/dL); falls slowly, may only appear after days |
| Serum sodium | Often reduced (SIADH or Addisonian state) |
Note: M. tuberculosis can occasionally cause a persistent PMN pleocytosis (like Nocardia, Aspergillus, Actinomyces).
— Adams and Victor's Principles of Neurology, 12th Edition
Microbiological Diagnosis
| Test | Details |
|---|---|
| Acid-fast smear (Ziehl-Neelsen) | Sensitivity 10–50%; improves with large volumes and repeat LPs |
| Culture | Gold standard but slow — 3–4 weeks for growth |
| PCR (nucleic acid amplification) | Rapid; single primer PCR has low sensitivity; multiplex PCR is significantly more sensitive |
| ADA (adenosine deaminase) | Significantly elevated in TB meningitis vs. other meningitides |
| Dot-ELISA (TB antigens/antibodies in CSF) | Positive in 86% of suspected cases; only 5% false positive |
| Tuberculin skin test | Positive in 85% of children; only 40–60% of adults |
| IGRA (interferon-gamma release assay) | ~90% specific for active TB; caution in endemic areas |
— Henry's Clinical Diagnosis and Management by Laboratory Methods; Adams and Victor
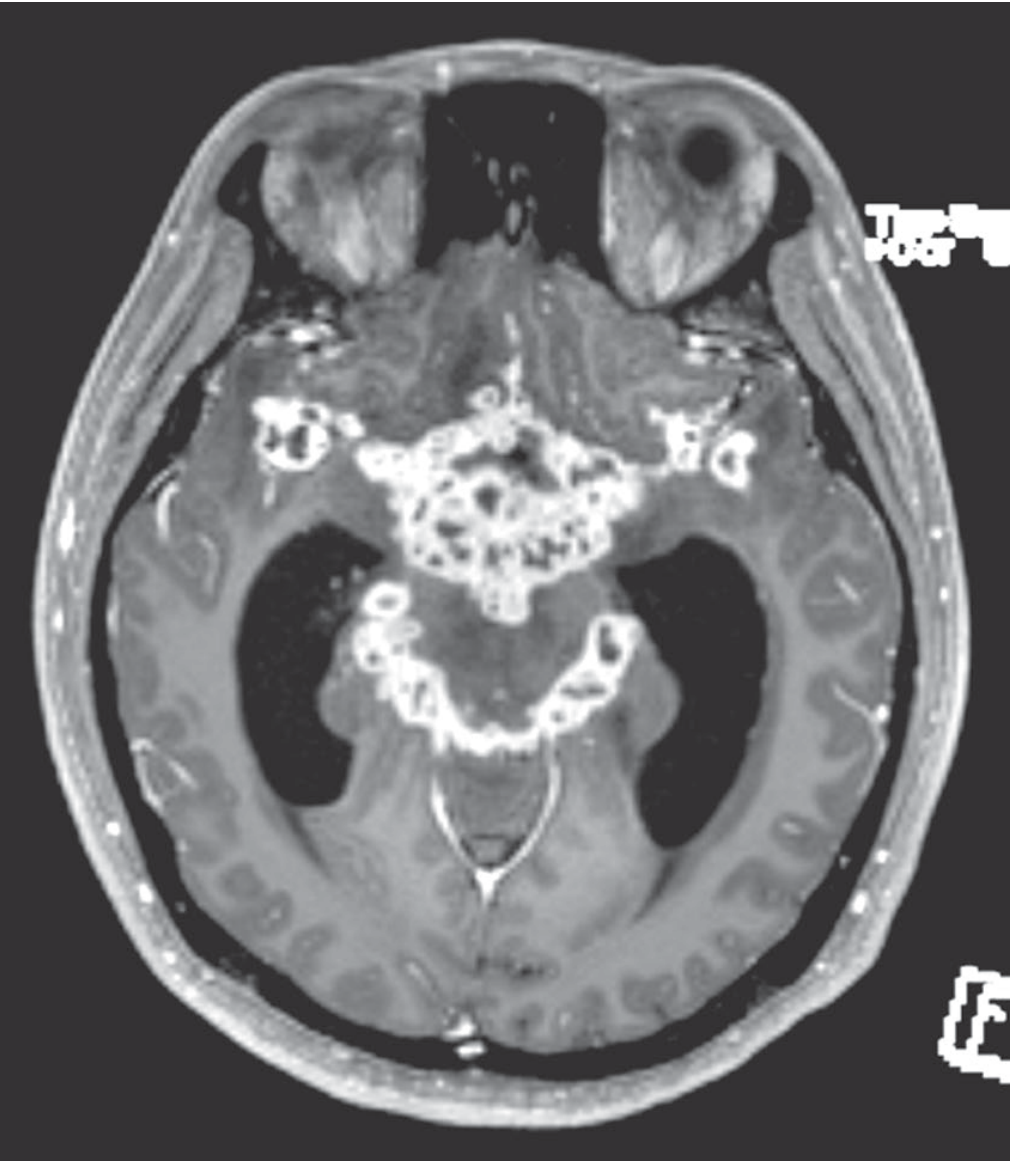
Imaging
- CT/MRI: Gadolinium enhancement of basal meninges is characteristic
- Hydrocephalus
- Deep cerebral infarctions (basal ganglia, internal capsule) from vasculitis of circle of Willis branches
- Tuberculomas: enhancing ring lesions (2–12 mm), may be multiple
- MR/CT angiography: can demonstrate vasculitic occlusions
Treatment
First-line Regimen (Intensive Phase — 2 months)
4-drug combination: Isoniazid (INH) + Rifampicin (RMP) + Ethambutol (EMB) + Pyrazinamide (PZA)
| Drug | Adult Dose | Key Toxicities |
|---|---|---|
| INH | 5 mg/kg/day | Peripheral neuropathy (give pyridoxine 50 mg/day), hepatitis |
| Rifampicin | 10 mg/kg/day | Hepatitis, drug interactions |
| Ethambutol | 15 mg/kg/day | Optic neuropathy (monitor visual acuity + red-green color) |
| Pyrazinamide | 20–35 mg/kg/day | Rash, GI disturbance, hepatitis |
Alternative: INH + PZA + high-dose RMP + moxifloxacin
Continuation Phase
All four (or three) drugs continued for total 9–12 months
Multidrug-Resistant TB (MDR-TB)
Add ethionamide (ETA) as fifth drug; ETA dose: 15–25 mg/kg/day in divided doses after meals (GI irritation); also causes optic neuropathy.
Corticosteroids
Dexamethasone IV 0.4 mg/kg/day for 1 week, then taper over 3–6 weeks — used for:
- Threatened subarachnoid block
- Raised ICP
- Reduces mortality from 41% → 32% (RCT in Vietnam, Thwaites et al.), but no effect on residual disability
HIV Co-infection
- Start antiretroviral therapy within 2 weeks of initiating anti-TB therapy
Neurosurgical Indications
- Hydrocephalus → ventriculoperitoneal shunt or drainage
- Up to 25% of advanced cases require neurosurgical intervention (Rosen's Emergency Medicine)
- Tuberculoma with mass effect → excision if no response to antibiotics
Prognosis
- Overall mortality: ~10% (higher in infants and elderly)
- HIV-infected patients: ~21% mortality (higher due to diagnostic delays and drug resistance)
- Approximately half of patients develop severe disability or death (Rosen's Emergency Medicine)
- Favorable prognostic factors: early diagnosis, MRC Stage I at presentation, younger age, no drug resistance
Other CNS Tuberculosis Syndromes
| Syndrome | Features |
|---|---|
| Tuberculous serous meningitis | Self-limited; modest pleocytosis, normal glucose — adjacent tuberculous focus rather than frank meningitis |
| Tuberculoma | Space-occupying lesion; 5–30% of intracranial masses in developing countries; ring-enhancing on MRI |
| Myeloradiculitis | Spinal cord/root involvement from meningeal exudate |
| Pott disease | Tuberculous osteomyelitis of spine → kyphosis, "Pott paraplegia" |
Sources: Adams and Victor's Principles of Neurology, 12th Edition | Henry's Clinical Diagnosis and Management by Laboratory Methods | Rosen's Emergency Medicine, 9th Edition
This is a shared conversation. Sign in to Orris to start your own chat.