Lactose intolerance with images easy to understand Notes
Reading File
Finding Sources
Finding Sources
Searching the Web
lactose intolerance pathophysiology mechanism simple explanation 2025
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have excellent content from multiple medical textbooks and three clear diagrams. Let me now generate a comprehensive, easy-to-understand set of notes.
🥛 Lactose Intolerance - Easy Notes
1. What Is Lactose?
Lactose is the main sugar found in milk and dairy products. It is a disaccharide - meaning it is made of TWO smaller sugars joined together:
- Glucose + Galactose = Lactose
To absorb lactose, your small intestine must first break it apart using an enzyme called lactase.
2. What Is Lactose Intolerance?
Lactose intolerance is when your body does not have enough lactase to digest lactose properly. The undigested lactose then causes uncomfortable symptoms.
"Lactose intolerance refers to a condition of pain, nausea, and flatulence after the ingestion of foods containing lactose, most notably dairy products."
- Basic Medical Biochemistry: A Clinical Approach, 6th ed.
3. How Does It Work? (The Mechanism)
Normal digestion (with enough lactase):
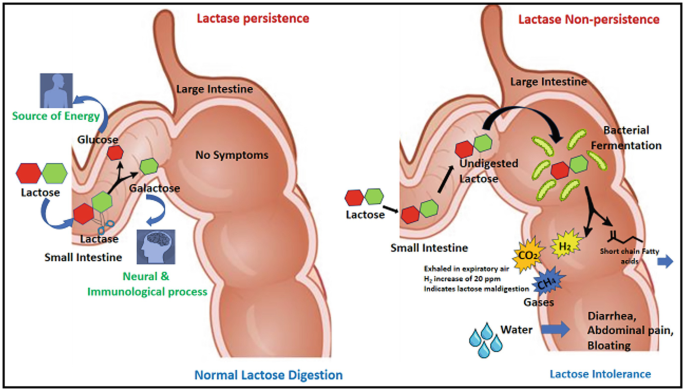
In normal digestion (left): Lactase in the small intestine breaks lactose into glucose + galactose, which are absorbed into the blood. No symptoms result.
In lactose intolerance (without enough lactase):
- Lactose is NOT broken down in the small intestine
- Undigested lactose travels to the large intestine (colon)
- Two bad things happen in the colon:
- Osmotic effect: Lactose draws water into the gut → diarrhea
- Bacterial fermentation: Colonic bacteria ferment the lactose → produce CO₂, CH₄ (methane), and H₂ (hydrogen) gas → bloating, gas, abdominal pain
4. Simple Diagram of the Mechanism
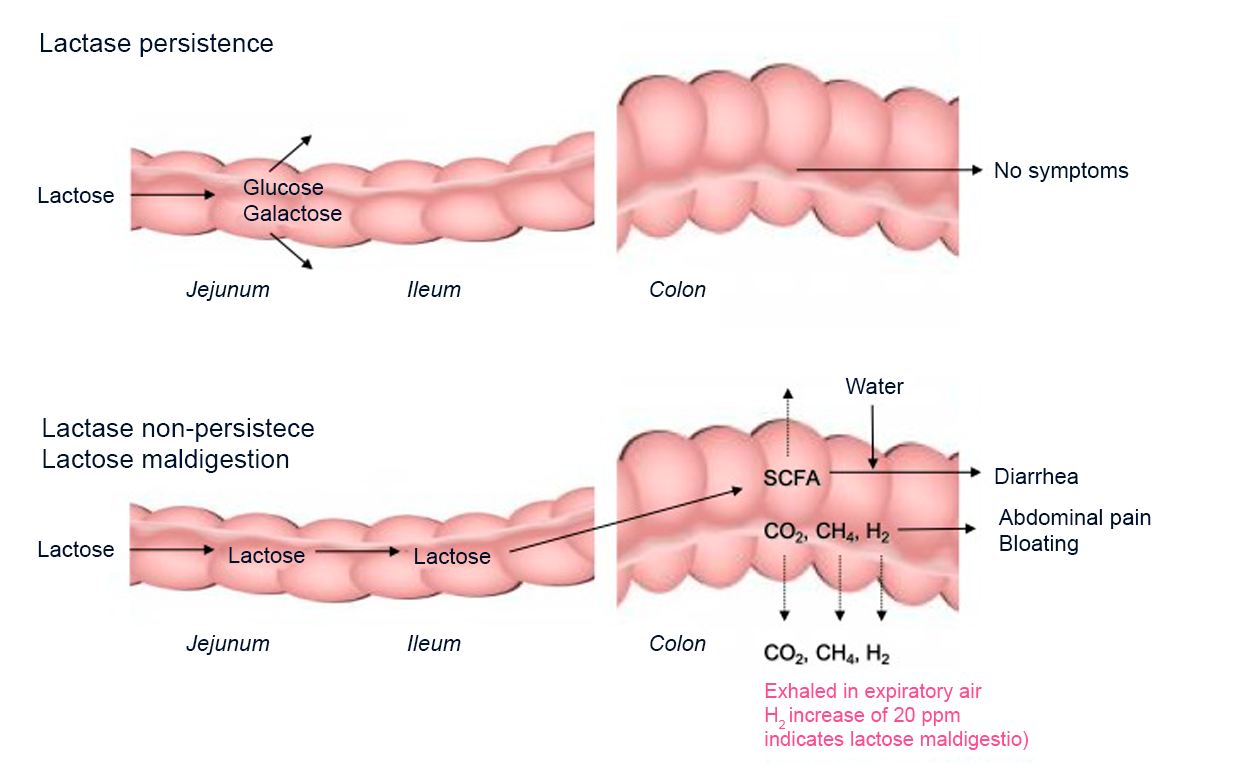
Top row (Lactase persistence = normal): Lactose is split in the jejunum/ileum into glucose + galactose and absorbed. The colon receives nothing problematic.
Bottom row (Lactase non-persistence = lactose intolerance): Lactose passes undigested into the colon, where bacteria ferment it to short-chain fatty acids (SCFA) + gases (CO₂, CH₄, H₂). This causes diarrhea, abdominal pain, and bloating. The exhaled H₂ is what the Hydrogen Breath Test detects (a rise of ≥20 ppm confirms maldigestion).
5. What Is Lactase? Where Is It?
- Lactase (full name: lactase-phlorizin hydrolase / LPH) is an enzyme on the brush border of the small intestinal lining (mainly the jejunum)
- It breaks the bond between glucose and galactose in lactose
- Lactase is abundant in newborns (needed for breast milk)
- In most people worldwide, lactase activity naturally declines after weaning (by age 5-10 years, it drops to ~10% of the newborn level)
6. Types of Lactose Intolerance
| Type | Cause | Notes |
|---|---|---|
| Primary (Most common) | Genetically programmed decline in lactase after childhood | Normal aging process in most of the world's population |
| Secondary | Gut injury destroys lactase-producing cells | Caused by gastroenteritis, Crohn's disease, celiac disease, etc. Usually reversible |
| Congenital (Very rare) | Born with no lactase at all | Genetic defect; symptoms from birth |
7. Who Gets It? (Epidemiology)
Lactase deficiency affects up to 60% of adults with non-Northern-European ancestry.
- High prevalence: Asian, African, Middle Eastern, Mediterranean, Native American populations
- Low prevalence: Northern European populations (evolved "lactase persistence" due to long history of dairy farming)
"Lactase persistence evolved in populations where milking livestock was important for survival - it was a positive selective advantage."
- Yamada's Textbook of Gastroenterology, 7th ed.
8. Symptoms
After eating dairy, symptoms typically appear within 30 minutes to 2 hours:
| Symptom | Why It Happens |
|---|---|
| Diarrhea | Osmotic effect - lactose pulls water into the colon |
| Bloating & Distension | Gas produced by bacterial fermentation |
| Flatulence (Gas) | CO₂, CH₄, H₂ from fermentation |
| Abdominal cramping/pain | Gut distension from water and gas |
| Nausea | Bowel irritation |
| Borborygmi (gurgling) | Fluid + gas moving through the gut |
Severity depends on:
- Amount of lactose eaten
- Remaining lactase activity
- Gut bacteria composition
- Speed of gastric emptying
- Individual sensitivity
"Skim milk and low-fat dairy tend to cause the MOST symptoms because low fat delivers lactose to the small intestine faster."
- Symptom to Diagnosis, 4th ed.
9. Easy Visual Summary

10. Diagnosis
A. Clinical (Most Common)
- Symptoms consistently occur after dairy
- Symptoms go away on a lactose-free diet for 2 weeks - this is the simplest diagnostic test
B. Hydrogen Breath Test (Gold Standard)
- Patient drinks a lactose solution
- Undigested lactose → bacteria ferment it → H₂ exhaled
- Rise of ≥20 ppm H₂ = positive test = confirms lactose maldigestion
- Pitfall: False-negative if patient recently took antibiotics (kills gut bacteria)
- Pitfall: False-positive if small intestinal bacterial overgrowth (SIBO) is present
C. Lactose Tolerance Test
- Patient drinks lactose → blood glucose is measured at intervals
- If lactose is absorbed properly, blood glucose rises
- A flat glucose curve = lactose not being digested
D. Genetic Testing
- Detects mutations in the MCM6 gene (the regulatory gene for lactase / LCT gene)
- The 13910C>T variant = associated with lactase persistence (Northern Europeans)
- Useful for confirming primary hypolactasia
11. Treatment
1. Dietary Changes (First Line)
- Reduce or eliminate dairy products
- Foods high in lactose: Milk, ice cream, soft cheeses, cream
- Foods lower in lactose: Hard cheeses (cheddar, parmesan), butter, yogurt (bacteria pre-digest some lactose)
- Lactose-free milk is available and well tolerated
2. Lactase Enzyme Supplements
- Taken as a tablet/capsule just before eating dairy
- Provides the missing enzyme to digest the lactose
- Example: Lactaid tablets
3. Probiotics
- Some gut bacteria can help ferment lactose more slowly and reduce symptoms
- Ongoing area of research
4. Calcium Supplementation
- People avoiding dairy may need calcium + vitamin D supplements to prevent bone loss
5. Post-Gastroenteritis (Secondary Type)
- Avoid all dairy for 2 weeks after recovery from gastroenteritis
- Lactase activity recovers as the gut lining heals
"In post-gastroenteritis lactose malabsorption, lactase activity will eventually recover when the intestinal brush border regenerates."
- Symptom to Diagnosis, 4th ed.
12. Quick Summary Table
| Feature | Detail |
|---|---|
| What is it? | Inability to digest lactose due to insufficient lactase |
| Where does it happen? | Small intestine (brush border of jejunum) |
| Mechanism | Undigested lactose → osmotic diarrhea + bacterial fermentation → gas |
| Most common type | Primary (genetic, age-related decline in lactase) |
| Most affected groups | Asian, African, Middle Eastern, Native American |
| Key symptoms | Diarrhea, bloating, gas, cramps after dairy |
| Best diagnostic test | Hydrogen breath test |
| Treatment | Low-lactose diet, lactase supplements |
13. Memory Hook 🧠
"No Lactase = Lactose Stays → Bacteria Feast → Gas + Water = Pain"
Sources: Costanzo Physiology 7th ed.; Yamada's Textbook of Gastroenterology 7th ed.; Symptom to Diagnosis 4th ed.; Lippincott Illustrated Reviews: Biochemistry 8th ed.; Basic Medical Biochemistry 6th ed.
Find recent research on lactose intolerance diagnosis and management
Searching PubMed
lactose intolerance diagnosis
Searching PubMed
lactose intolerance management treatment
Searching the Web
lactose intolerance diagnosis management guidelines 2024 2025
Reading Article
PMID: 39255349
Reading Article
PMID: 36308983
Reading Article
PMID: 38426798
Searching PubMed
lactose intolerance hydrogen breath test lactase
Reading Web Page
https://www.revistagastroenterologiamexico.org/en-clinical-g…
Reading Article
PMID: 40432984
Reading Article
PMID: 41843249
Reading Article
PMID: 38159728
Reading Article
PMID: 36750424
Reading Article
PMID: 39641896
I now have rich, up-to-date evidence. Here is the synthesized research summary:
Recent Research on Lactose Intolerance: Diagnosis & Management
Overview of the Evidence Landscape
The field has shifted in two major directions over the last 3-5 years:
- Diagnosis - moving away from symptom-only assessment toward objective testing, with a growing debate between the hydrogen breath test (HBT) vs. genetic testing depending on the population
- Management - moving away from total dairy elimination toward personalized, incremental lactose tolerance, microbiota-based strategies, and addressing comorbidities like IBS and SIBO
DIAGNOSIS
1. Self-Reported Symptoms Are Unreliable - A Systematic Review Warning
Pop A et al. (2024) - Systematic Review - PMID: 39255349 J Gastrointestin Liver Dis, Sep 2024
- Analyzed 6 studies with 845 IBS patients
- Found significant variability and only moderate accuracy in self-reported lactose intolerance for diagnosing actual lactose intolerance
- HBTs revealed that self-reported symptoms frequently produce false positives
- Key conclusion: A lactose-free diet should NOT be routinely recommended for IBS patients without objective confirmation, and routine HBT is not recommended in IBS without clear indication
- This challenges the common clinical habit of diagnosing lactose intolerance purely by history in patients with functional bowel symptoms
2. Genetic Testing May Outperform HBT in Lactase-Persistent Populations
Stouten K et al. (2023) - Observational Study, n=1,101 - PMID: 36750424 Ann Clin Biochem, Jul 2023
- Compared HBT vs. DNA genotyping of LCT-13910 C/T in a Dutch population (high lactase-persistence prevalence)
- HBT performance: Sensitivity 89%, Specificity 94%, PPV 80%, NPV 97%
- Symptom questionnaire during HBT added little diagnostic value
- Recommendation: In populations with high lactase-persistence allele prevalence (Northern European), genetic genotyping should replace HBT as the first-line diagnostic tool
Clinical takeaway: Diagnostic strategy should be population-tailored. HBT remains better in high-prevalence populations (Asian, African, Middle Eastern), while genetic testing is more efficient in low-prevalence European populations.
2025 AMG Clinical Guideline (Asociación Mexicana de Gastroenterología)
A fresh 2025 clinical guideline based on a Delphi consensus (26 statements, 15 specialist participants) makes these key diagnostic recommendations:
- Clinical diagnosis based solely on symptoms after lactose ingestion is NOT a reliable diagnostic method (88.9% strong agreement)
- The lactose breath test is the recommended first-line noninvasive tool - highly sensitive
- Genetic studies and biochemical tests complement the breath test
- Defined five distinct LIRD phenotypes that must be differentiated: lactase nonpersistence, hypolactasia, clinical lactose intolerance, self-perceived lactose intolerance, and lactose sensitivity
MANAGEMENT
3. Gut Microbiota Adaptation - Daily Lactose Exposure May Increase Tolerance
JanssenDuijghuijsen L et al. (2024) - PMID: 38159728 Am J Clin Nutr, Mar 2024
This is one of the most clinically significant recent findings:
- 25 healthy Asian adults with lactase-nonpersistent genotype were given incrementally increasing lactose doses over 12 weeks (3g → 6g → 12g twice daily)
- Results:
- Bifidobacterium abundance increased significantly (5.5% → 10.4%, p=0.009)
- Fecal β-galactosidase activity doubled (272 → 570 U/g, p<0.001)
- Expired hydrogen during HBT fell 1.5-fold (57 → 38 ppm·min, p=0.01)
- Daily consumption was well tolerated with mild/no GI complaints
- Mechanism: Bifidobacteria metabolize lactose without gas production, reducing intestinal gas formation
- Conclusion: Gradual lactose exposure adapts the gut microbiota and may lift the necessity for complete dairy elimination - a paradigm shift from strict avoidance
4. Low-Lactose Diet (Not Lactose-Free) Is the New Standard
Borralho AI & Marcos P (2025) - Comprehensive Review - PMID: 40432984 GE Port J Gastroenterol, Apr 2025
Key management messages from this 2025 review:
- Instead of a completely dairy-free diet, a low-lactose diet allowing up to 12-15 g lactose/day is well tolerated and beneficial for most LI individuals
- Lactose-free products, hard cheeses, and fermented dairy (yogurt) are practical alternatives
- Probiotics, prebiotics, and plant-based beverages may be helpful but their effectiveness has not yet been conclusively proven
- The HBT remains the most widely used and effective diagnostic method when combined with symptom assessment
5. Probiotics - Emerging Evidence (With Caveats)
Perets TT et al. (2026) - Review - PMID: 41843249 Antonie Van Leeuwenhoek, Mar 2026
- Reviews probiotics as a treatment strategy via modulating colonic metabolism and enhancing lactose digestion
- Current international guidelines require both typical symptoms AND pathologic breath test results to diagnose lactose intolerance
- Avoiding dairy increases risk of nutritional deficiencies (calcium, vitamin D) - probiotics and microbiota strategies offer an alternative to restrictive diets
- Research is ongoing; most robust benefit seen with specific strains
Oliveira LS et al. (2022) - Systematic Review - PMID: 36308983 Clin Nutr, Dec 2022
- Reviewed 5 RCTs covering probiotics and prebiotics
- Best probiotic results: Limosilactobacillus reuteri DSM 17938 and Lactobacillus acidophilus DDS-1 - both showed significant symptom improvement
- Prebiotic GOS (RP-G28) showed high-certainty evidence for reducing symptoms even 30 days post-cessation
- Overall probiotic evidence is still limited; needs larger, methodologically stronger RCTs
6. Treating SIBO Can Improve Lactase Activity in IBS
García-Cedillo MF et al. (2025) - PMID: 39641896 Dig Dis Sci, Jan 2025
This is a novel finding with practical clinical implications:
- IBS patients with small intestinal bacterial overgrowth (SIBO) often have secondary lactase deficiency because SIBO suppresses brush-border enzyme activity
- After 2 weeks of rifaximin-alpha (400 mg q8h):
- Lactose maldigestion (by HBT) dropped from 88% to 52% of subjects
- Significant symptomatic improvement (abdominal pain 60%, borborygmi 72%, stool consistency 72%)
- D-Xylose levels improved (marker of mucosal function)
- Clinical implication: Before labeling a patient as lactose intolerant, always consider and treat SIBO - especially in IBS patients
Research Summary Table
| Topic | Key Finding | Best Evidence | Year |
|---|---|---|---|
| Self-reported LI diagnosis | Unreliable; leads to false positives | Systematic Review (n=845) | 2024 |
| Genetic testing vs. HBT | Genotyping preferred in European populations | Observational (n=1,101) | 2023 |
| Microbiota adaptation | Gradual lactose exposure increases tolerance via Bifidobacterium | Clinical trial (n=25) | 2024 |
| Optimal diet | Low-lactose (12-15g/day), not lactose-free | Review (2013-2023 lit) | 2025 |
| Probiotics | L. reuteri DSM 17938, L. acidophilus DDS-1 most effective; GOS prebiotic high certainty | Systematic Review | 2022 |
| SIBO-lactase connection | Rifaximin improves lactase activity in IBS+SIBO | Pilot study | 2025 |
| Infant colic & lactase | Lactase supplementation evidence inconclusive | Systematic Review (5 RCTs) | 2024 |
What This Means Clinically (2025-2026 Takeaways)
- Don't diagnose on symptoms alone - objective testing (HBT or genetics depending on ethnicity) is required per current guidelines
- Total dairy elimination is outdated - up to 12-15g lactose/day is tolerated; gradual re-introduction also builds tolerance
- Gut microbiota is key - incremental lactose exposure, specific probiotics (L. reuteri, L. acidophilus), and prebiotic GOS are evidence-backed adjuncts
- Always screen for SIBO in IBS patients with suspected secondary lactose intolerance - treating SIBO with rifaximin can restore lactase function
- Choose your diagnostic tool by population - genetic LCT-13910 C/T testing outperforms HBT in Northern European populations; HBT remains better in Asian/African populations
- Calcium and vitamin D are at risk - nutritional counseling is an essential part of management for anyone reducing dairy
This is a shared conversation. Sign in to Orris to start your own chat.