Explain breast carcinoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive content from Robbins & Cotran, Robbins Basic Pathology, Schwartz's Surgery, and Bailey & Love. Here is the full, structured explanation of breast carcinoma.
Breast Carcinoma
1. Overview and Epidemiology
Breast carcinoma is the most common malignancy globally and the leading cause of cancer death in females worldwide. In 2020, it surpassed lung cancer as the most common cancer overall with an estimated 2.3 million new cases, accounting for ~12% of all new cancer diagnoses. The lifetime risk for a US female is 1 in 8 (living to age 90). Over 297,790 new invasive cases and 43,000 deaths were projected in the US in 2023 alone.
- Rare below age 25; incidence rises sharply after age 30
- TNBC and HER2 subtypes peak in middle age (~40 years); luminal cancers continue to rise into old age
- Highest incidence in North America, Northern/Western Europe, and Australia/New Zealand
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 970-971
2. Risk Factors
| Category | Specific Factors |
|---|---|
| Hormonal | Early menarche, late menopause, nulliparity, late first pregnancy, postmenopausal HRT, exogenous estrogen |
| Genetic (high-risk) | BRCA1, BRCA2, PALB2, TP53 mutations; ~12% of all breast cancers from germline mutations |
| Family history | 25-33% of breast cancers are familial |
| Prior breast disease | LCIS, DCIS, atypical ductal hyperplasia |
| Age | 75% diagnosed after age 50 |
| Lifestyle | Obesity (postmenopausal), alcohol, radiation exposure |
| Reproductive | Delayed childbearing, fewer pregnancies, reduced breastfeeding |
BRCA1 and BRCA2 account for 80-90% of single-gene familial breast cancers and 3-6% of ALL breast cancers. Most female BRCA carriers develop breast cancer by age 70. BRCA mutations also increase risk for ovarian, pancreatic, and prostatic carcinoma. In Ashkenazi Jewish populations, ~1 in 40 individuals carries one of three specific BRCA mutations.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 972-973; Robbins & Kumar Basic Pathology, p. 719
3. Classification
3.1 In Situ Carcinomas (Non-invasive)
Ductal Carcinoma In Situ (DCIS)
- Neoplastic ductal cells confined within the basement membrane
- Most often detected mammographically as calcifications
- A direct precursor to invasive ductal carcinoma - if untreated, eventually invades in the same breast
- Subtypes: comedo (with central necrosis - most aggressive), cribriform, micropapillary, solid
Lobular Carcinoma In Situ (LCIS)
- Neoplastic cells filling lobular acini; lacks E-cadherin expression (key diagnostic marker on IHC)
- Not an obligate precursor but a marker of increased bilateral risk
- If invasive carcinoma subsequently develops, two-thirds occur in the same breast, one-third in the contralateral breast
- Removed from TNM staging in AJCC 8th edition
Histology of DCIS with central necrosis (comedo type):
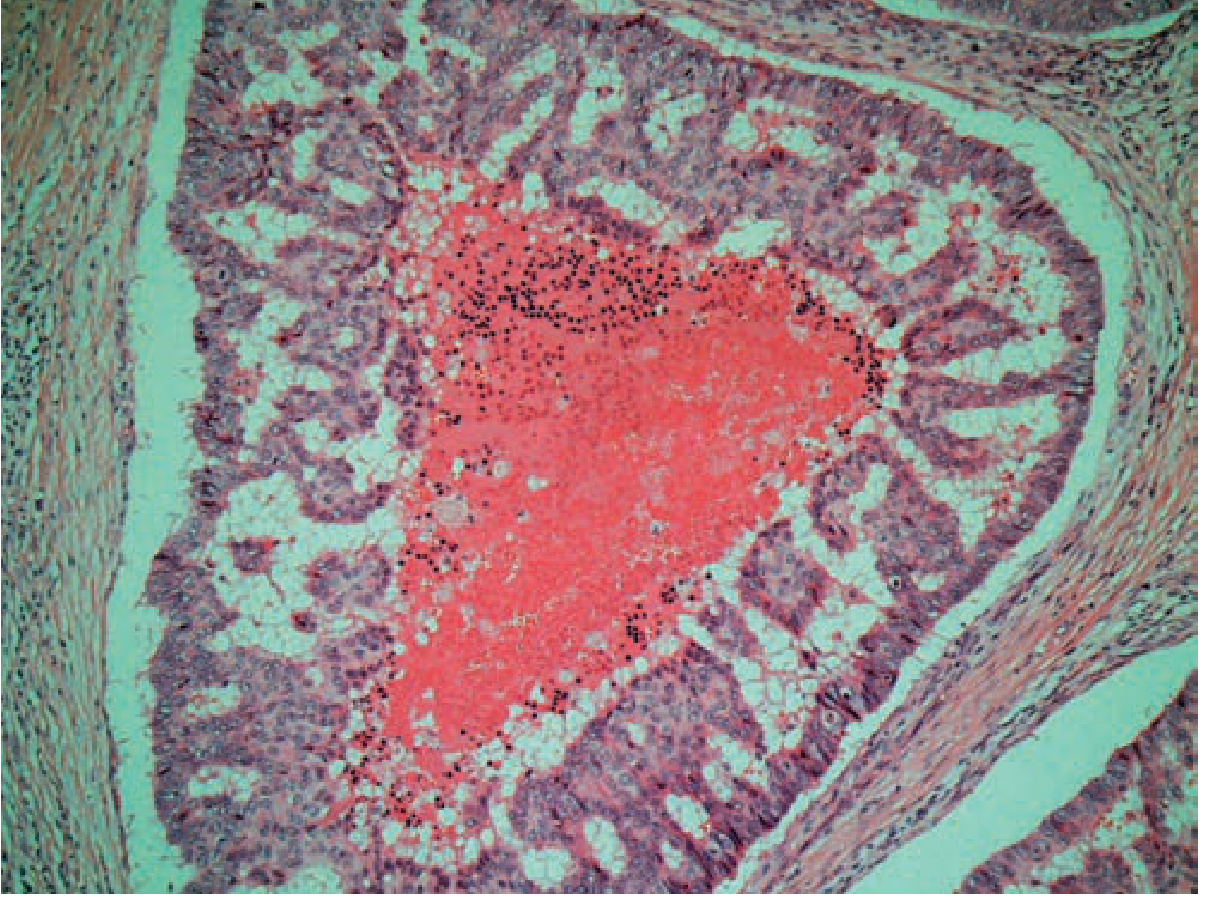
3.2 Invasive (Infiltrating) Carcinomas
Most breast malignancies are adenocarcinomas, subdivided into ~20 subtypes.
| Type | Frequency | Key Features |
|---|---|---|
| No Special Type (NST) / IDC | ~75-80% | Most common; hard, irregular, scirrhous mass; desmoplastic stroma; grating sound on cut; worst prognosis among special types |
| Invasive Lobular Carcinoma | 10-15% | Single file "Indian file" pattern; lacks E-cadherin; bilateral risk; tends to metastasize to GI tract, peritoneum, meninges |
| Medullary Carcinoma | ~4% | Soft, hemorrhagic; dense lymphocytic infiltrate; large pleomorphic nuclei; sheet-like growth; BRCA1-associated; better prognosis despite high grade |
| Mucinous (Colloid) Carcinoma | ~2% | Extracellular mucin pools; glistening cut surface; >90% ER-positive; lymph node mets in 33%; 5-yr survival 73% |
| Papillary Carcinoma | ~2% | Fibrovascular stalks; seventh decade; 87% ER-positive; low LN metastasis rate |
| Tubular Carcinoma | ~2% | Haphazard small tubules; 94% ER-positive; excellent prognosis; often found on screening mammography |
| Paget's Disease of Nipple | Rare | Chronic eczematous eruption of nipple; pathognomonic large pale vacuolated "Paget cells" in rete pegs; CEA-positive (vs melanoma S-100) |
To qualify as a "special type," at least 90% of the tumor must show the defining histologic features. Special types generally have better prognosis than NST.
- Schwartz's Principles of Surgery, p. 593-594; Robbins Cotran p. 978
3.3 Histologic Grading (Nottingham Score)
All invasive carcinomas are graded on three criteria:
- Tubule formation (glandular differentiation)
- Nuclear pleomorphism
- Mitotic rate
| Grade | Description |
|---|---|
| Grade 1 (Well differentiated) | Tubular/cribriform pattern, small uniform nuclei, low mitotic rate |
| Grade 2 (Moderately differentiated) | Solid clusters, greater pleomorphism, more mitoses |
| Grade 3 (Poorly differentiated) | Ragged nests/sheets, enlarged irregular nuclei, high mitoses, necrosis |
4. Molecular Classification
Breast carcinoma is classified into three major clinical subtypes based on biomarker expression, with six intrinsic molecular subtypes by gene expression profiling.
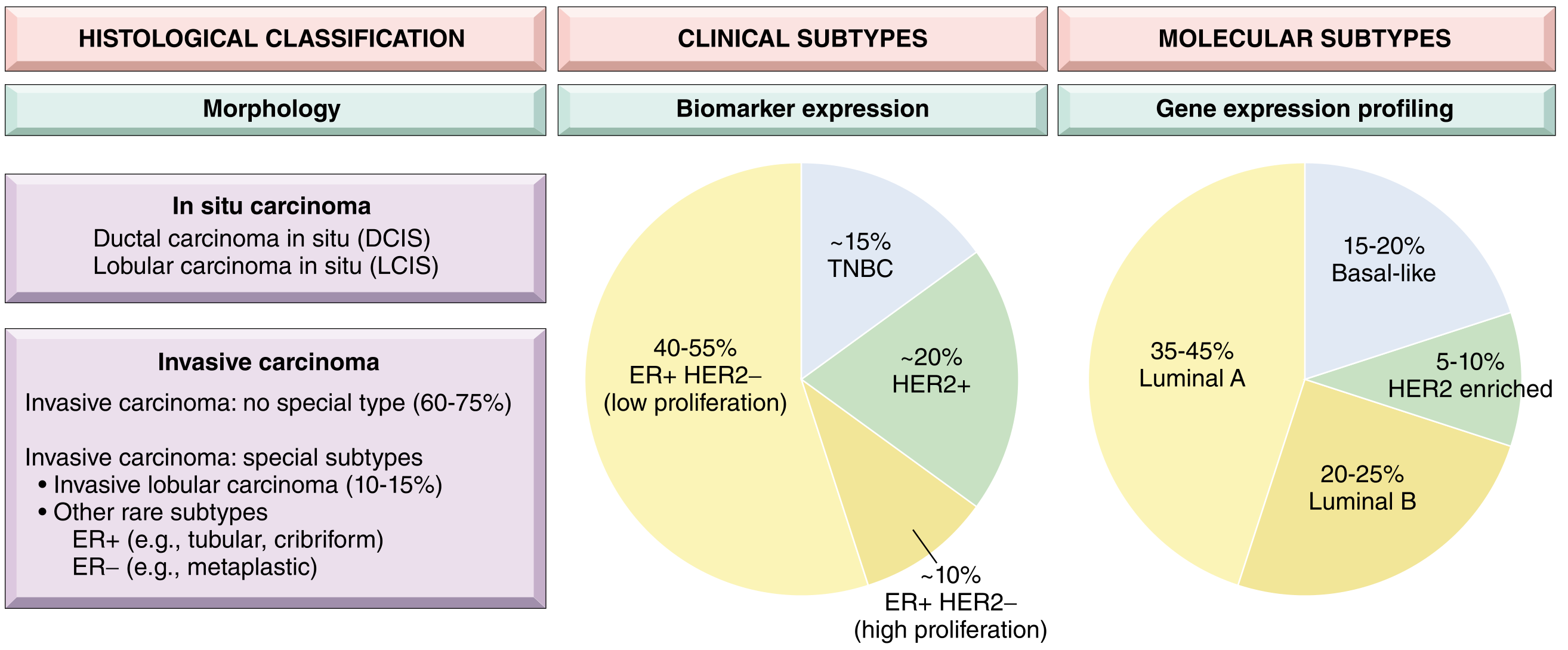
| Clinical Subtype | Biomarker Profile | Molecular Subtype | Frequency | Key Features |
|---|---|---|---|---|
| Luminal | ER+/HER2- | Luminal A (low prolif) / Luminal B (high prolif) | 50-65% / 10% | Most common; best prognosis (esp. Luminal A); responds to hormonal therapy |
| HER2 | HER2 overexpressed (ER+/- ) | HER2-enriched | ~20% | HER2 amplification; responds to trastuzumab; moderate prognosis |
| Triple-Negative (TNBC) | ER-/PR-/HER2- | Basal-like | ~15% | Often high grade; BRCA1 association; chemosensitive but aggressive; worst prognosis |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 973-975
5. Pathogenesis and Molecular Evolution
Two major pathways of breast cancer evolution exist:
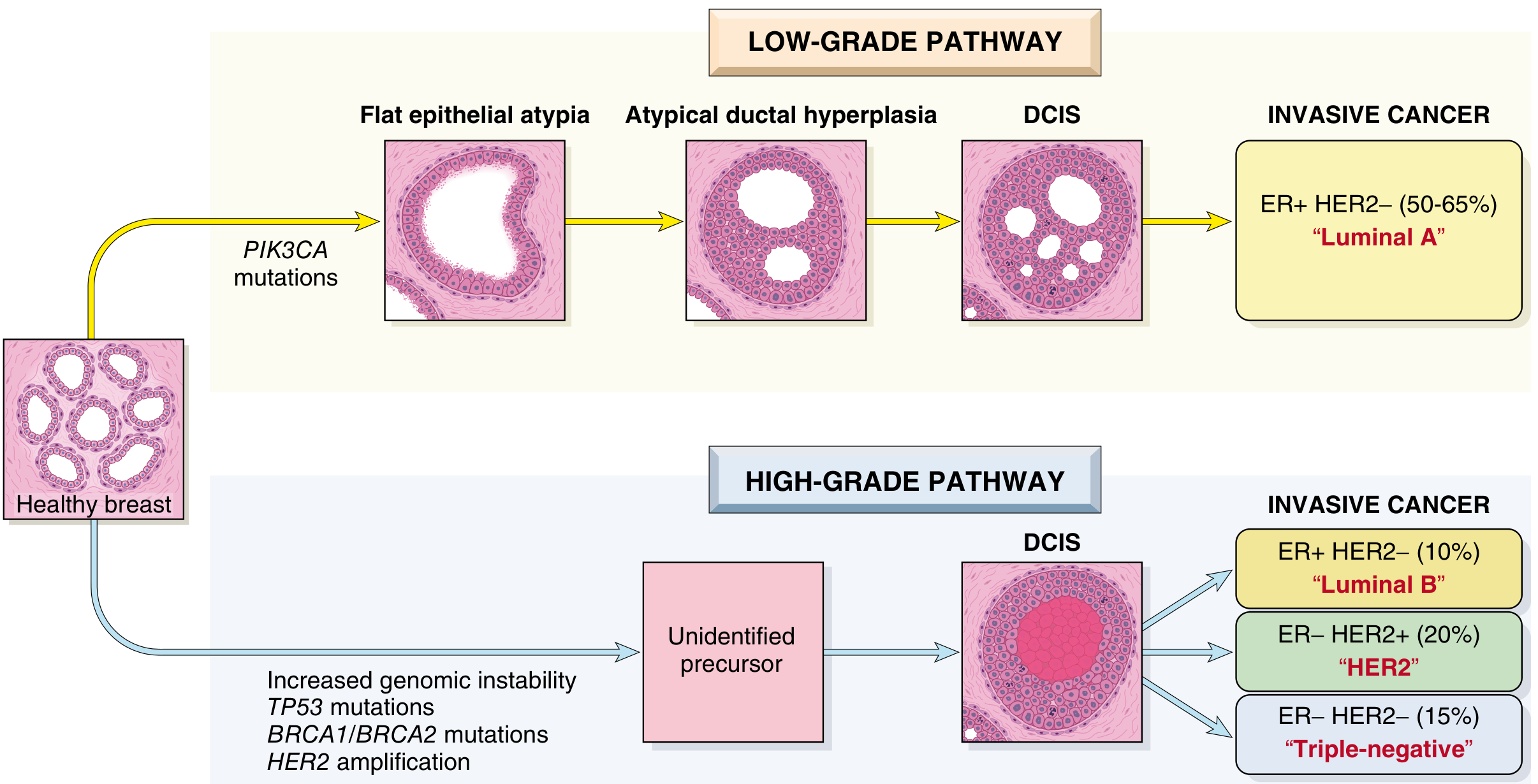
Low-grade pathway:
- PIK3CA mutations → Flat epithelial atypia → Atypical ductal hyperplasia → Low-grade DCIS → ER+/HER2- (Luminal A) invasive cancer
High-grade pathway:
- TP53 mutations, BRCA1/BRCA2 inactivation, HER2 amplification → Genomic instability → High-grade DCIS → Luminal B, HER2+, or TNBC
Key molecular alterations:
- BRCA1/BRCA2 - DNA double-strand break repair via homologous recombination; tumors with these defects are sensitive to PARP inhibitors
- HER2 amplification - overexpression of the epidermal growth factor receptor; targetable with trastuzumab, pertuzumab, lapatinib
- PIK3CA mutations - PI3K pathway activation; targetable with PI3K inhibitors (e.g., alpelisib)
- TP53 mutations - common in high-grade tumors; associated with genomic instability
6. Clinical Features
Symptoms and signs:
- Painless, hard, irregular lump (most common presentation)
- Skin changes: dimpling, peau d'orange (dermal lymphatic involvement)
- Nipple retraction or discharge (bloody in DCIS/papillary)
- Axillary lymphadenopathy
- Inflammatory breast carcinoma: diffuse erythema, warmth, skin thickening, rapid onset - caused by dermal lymphatic obstruction; no discrete mass; T4d staging; worst prognosis
Common metastatic sites:
Lymph nodes (axillary) → lungs → liver → bone → brain
- Lobular carcinoma has a predilection for GI tract, peritoneum, and meninges
7. Diagnosis and Imaging
Triple assessment:
- Clinical examination
- Imaging (mammography ± ultrasound ± MRI)
- Pathology (FNAC or core needle biopsy)
Mammography:
- Principal screening tool; detects calcifications, densities, architectural distortion
- Average size on mammography: ~1 cm (vs. ~2-3 cm when palpable)
- Sensitivity/specificity increases with age: lesion probability of cancer = 10% at age 40, >25% after age 50
- ~10% of invasive carcinomas are mammographically occult
Digital breast tomosynthesis, ultrasound, and MRI serve as adjuncts for dense breasts and equivocal findings.
8. Staging (AJCC 8th Edition - TNM)
Primary Tumor (T)
| Stage | Description |
|---|---|
| T1 | ≤2 cm (T1a ≤0.5, T1b 0.5-1, T1c 1-2 cm) |
| T2 | >2 cm but ≤5 cm |
| T3 | >5 cm |
| T4 | Any size with chest wall/skin extension; T4d = inflammatory |
Regional Lymph Nodes (N)
| Stage | Description |
|---|---|
| N0 | No regional LN involvement |
| N1 | Movable ipsilateral Level I/II axillary nodes |
| N2 | Fixed/matted ipsilateral axillary nodes; or internal mammary without axillary |
| N3 | Infraclavicular, internal mammary + axillary, or supraclavicular nodes |
Distant Metastasis (M)
- M0: No distant mets; M1: Distant metastasis present
AJCC 8th edition combines anatomic stage + molecular group (ER, PR, HER2, and gene expression score) to create prognostic stage groups that better estimate survival.
- Schwartz's Principles of Surgery, p. 604
9. Treatment
Treatment is determined by stage, biologic subtype, and patient's general health.
Local Control
Surgery:
- Breast-conserving surgery (lumpectomy + radiation): Equivalent survival to mastectomy for stages I-II; requires adequate surgical margins
- Mastectomy (simple or modified radical): Required for multicentric disease, large tumors relative to breast size, prior radiation, patient preference
- Axillary assessment: Sentinel lymph node biopsy (SLNB) is standard for clinically node-negative patients; axillary lymph node dissection (ALND) if sentinel node positive
Radiation therapy:
- Mandatory after breast-conserving surgery
- Chest wall radiation after mastectomy for T3/T4 or ≥4 positive nodes
Systemic Therapy
| Subtype | Therapy |
|---|---|
| ER+/PR+ (Luminal) | Endocrine therapy (tamoxifen for premenopausal; aromatase inhibitors [anastrozole, letrozole] for postmenopausal); CDK4/6 inhibitors (palbociclib, ribociclib) for advanced disease |
| HER2+ | Trastuzumab (Herceptin) + pertuzumab; TDM-1 (T-DM1); lapatinib; often with chemotherapy |
| TNBC | Chemotherapy (anthracyclines + taxanes); PARP inhibitors (olaparib, talazoparib) for BRCA-mutant; immunotherapy (pembrolizumab) for PD-L1-positive |
| BRCA mutant | PARP inhibitors (all subtypes); olaparib/talazoparib |
Neoadjuvant therapy (pre-surgery) is used to downstage tumors and convert inoperable to operable disease, and is standard for locally advanced and HER2+/TNBC cases.
In Situ (Stage 0)
- LCIS: Observation, chemoprevention (tamoxifen/raloxifene), or bilateral prophylactic mastectomy
- DCIS: Wide local excision + radiation (or mastectomy); endocrine therapy if ER+
10. Prognosis
Prognosis depends on:
- Biologic subtype - Luminal A is best; TNBC is worst
- Anatomic stage - Lymph node involvement is the most powerful single prognostic factor
- Histologic grade - Grade 1 far better than Grade 3
- Tumor size
| Subtype | 5-year Overall Survival |
|---|---|
| Luminal A | ~90%+ |
| HER2 (treated) | ~85%+ |
| TNBC | ~70-75% (early stage); poor in metastatic |
| Metastatic (Stage IV) | ~28% (5-year) |
Special-type carcinomas with favorable prognosis: tubular, mucinous, papillary, medullary (paradoxically better than grade suggests due to immune response).
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, pp. 970-980
- Robbins & Kumar - Basic Pathology, p. 719
- Schwartz's Principles of Surgery, 11th Ed., pp. 590-610
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 53
This is a shared conversation. Sign in to Orris to start your own chat.