what are the best surgical options for a patient 35y/f with type 2 fibroids who wants to retain fertility and who has failed medical management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"uterine fibroid" AND "myomectomy" AND "fertility"
Finding Sources
Finding Sources
Searching PubMed
"leiomyoma" AND "myomectomy" AND "reproductive outcome"
Finding Sources
Finding Sources
Searching PubMed
"submucosal fibroid" AND "hysteroscopic myomectomy" AND "fertility"
Finding Sources
Finding Sources
Searching PubMed
"uterine leiomyoma" AND "laparoscopic myomectomy" AND "pregnancy"
Reading File
Finding Sources
Searching PubMed
"FIGO" AND "leiomyoma" AND "classification" AND "hysteroscopy"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading Article
Reading File
Reading File
Reading File
Reading File
Reading File
I have all the data needed. Let me now compose the comprehensive answer.
Surgical Options for FIGO Type 2 Fibroid in a 35-Year-Old Wanting to Preserve Fertility (After Failed Medical Management)
Understanding FIGO Type 2
A FIGO type 2 fibroid is submucosal with 50% or more of its diameter extending into the myometrium, while still maintaining some intracavitary component. This distinction matters enormously for surgical planning because it sits at the boundary between hysteroscopic and open/laparoscopic approaches.
Per the FIGO classification table from Sabiston's Textbook of Surgery:
| Type | Location | Recommended Surgical Approach |
|---|---|---|
| 0 | Intracavitary | Vaginal or hysteroscopic |
| 1 | Submucosal (<50% intramural) | Hysteroscopic |
| 2 | Submucosal (≥50% intramural) | Hysteroscopic OR open/laparoscopic |
| 3-5 | Intramural | Open or laparoscopic |
Sabiston Textbook of Surgery, p. 2968
Primary Option: Hysteroscopic Myomectomy (Preferred When Feasible)
Hysteroscopic myomectomy (transcervical resection of fibroid, TCRM) is the least invasive fertility-preserving option and should be the first-line surgical approach if the type 2 fibroid is amenable to hysteroscopic access.
Why it is preferred:
- Avoids a uterine incision, so there is no scar in the myometrium - this eliminates the risk of uterine rupture in subsequent pregnancy
- Shorter recovery, same-day or overnight procedure
- Direct visualization of the endometrial cavity allows concurrent treatment of any cavity distortion
- Well-established improvement in pregnancy outcomes when submucosal fibroids distort the cavity
Technical considerations for type 2:
- Type 2 is the most challenging class for hysteroscopic resection because the majority of the fibroid is intramural
- For larger type 2 fibroids, a two-stage hysteroscopic procedure is often necessary: resect the intracavitary component first, then allow the remaining intramural component to migrate into the cavity over several weeks before resecting the rest
- Risks include: fluid overload from distension media (hyponatraemia), uterine perforation, thermal injury, intrauterine adhesion (Asherman's syndrome) formation post-resection
- A 2026 paper (PMID 42050576) specifically studied intrauterine adhesion formation after hysteroscopic myomectomy and found perioperative inflammatory response to be a key determinant - adjunctive measures (estrogen, hyaluronic acid gel) are used to reduce this risk
Bailey and Love's Short Practice of Surgery, p. 2892
Second Option: Laparoscopic Myomectomy
When the type 2 fibroid is large (typically >4-5 cm), multiple, or when the hysteroscopic approach has failed or is deemed insufficient, laparoscopic myomectomy is the next fertility-preserving option.
Advantages over open surgery (2024 Systematic Review, PMID 37566224 - 9 studies, 1,723 patients):
- Shorter hospital stay (p=0.04)
- Less intraoperative blood loss (p<0.00001)
- Shorter ileus duration (p<0.00001)
- Fewer episodes of postoperative fever (p=0.04)
- Reproductive outcomes (pregnancy rate, preterm delivery, delivery mode) were equivalent to mini-laparotomy
Critical technique requirement for fertility:
A multilayered myometrial closure is essential. A review of 19 published cases of uterine rupture after laparoscopic myomectomy found that nearly all involved failure to close the defect properly - 7 cases had no repair at all, and only 3 had multilayered closure. Excessive use of monopolar/bipolar diathermy for hemostasis is also implicated in poor wound healing and subsequent rupture risk.
(Berek & Novak's Gynecology, p. 5067)
Recurrence after laparoscopic myomectomy: A 2026 meta-analysis (PMID 41846572) documented recurrence rates and associated factors - multiple fibroids, younger age, and larger fibroids at baseline carry higher recurrence risk - relevant for counselling this 35-year-old patient.
Third Option: Open (Abdominal) Myomectomy
Reserve for:
- Very large fibroids (>10 cm) or numerous fibroids making laparoscopy technically difficult
- Inaccessible fibroid location
- Failed laparoscopic approach
- Deep intramural involvement making multilayered closure difficult laparoscopically
Open myomectomy provides the best exposure for complex cases and the easiest multilayered closure, but carries more morbidity (longer hospital stay, greater adhesion formation, longer recovery).
Compared to hysterectomy, myomectomy has similar or lower complication rates. One retrospective review of 197 myomectomies vs. 197 hysterectomies with similar uterine size showed longer operating time with myomectomy (200 vs. 175 min) but significantly less blood loss (227 vs. 484 mL).
(Berek & Novak's Gynecology, p. 5184)
Key Preoperative Consideration: GnRH Agonist Pretreatment
If the patient has significant anaemia from heavy bleeding (which is common with submucosal/type 2 fibroids and failed medical management):
- GnRH agonist (e.g., leuprolide) for 2-3 months preoperatively can reduce fibroid volume by ~30% and uterine volume by ~35%, reduce blood loss at surgery, and correct anaemia
- This is especially helpful before hysteroscopic resection of large type 2 fibroids, as reducing the intramural component may make single-stage hysteroscopy feasible
- Ulipristal acetate (selective progesterone receptor modulator) was previously used for preoperative downsizing but has been suspended in many countries due to rare but serious hepatotoxicity
(Berek & Novak's Gynecology, p. 5111-5113)
What to Avoid in a Fertility-Preserving Context
- Uterine artery embolization (UAE) - Not recommended if future pregnancy is desired. UAE can cause non-target embolization of ovarian vasculature, premature ovarian failure, and significantly higher rates of miscarriage and placental complications compared to myomectomy
- Endometrial ablation - Absolutely contraindicated if fertility is desired
- Radiofrequency ablation (Acessa/transcervical radiofrequency) - Fertility data are limited; currently not recommended as standard of care for women actively trying to conceive
- Hysterectomy - Definitively excluded given the patient's fertility wishes
Recommended Surgical Decision Pathway for This Patient
FIGO Type 2 fibroid, 35F, fertility-preserving, failed medical management
↓
Assess fibroid size, number, MRI to map intramural depth
↓
Size ≤4 cm, single, accessible → Attempt hysteroscopic myomectomy
(consider 2-stage technique if large intramural component)
↓
Size >4-5 cm, multiple, or failed hysteroscopic attempt
↓
Laparoscopic myomectomy (surgeon experience essential; multilayer closure mandatory)
↓
Very large, numerous, or technically difficult laparoscopically
↓
Open (abdominal) myomectomy
Postoperative Fertility Counselling
- Trial of labor after myomectomy carries a 0.47% risk of uterine rupture (comparable to trial of labor after cesarean)
- Caesarean delivery is recommended if the endometrial cavity was entered during myomectomy or the repair was complex
- Allow 3-6 months of uterine healing before attempting conception
- Fibroid recurrence rates after myomectomy are meaningful (~20-30% at 5 years radiologically, ~10% requiring repeat surgery) - counsel regarding the reproductive time window
(Berek & Novak's Gynecology, pp. 5063-5065)
Sources:
- Berek & Novak's Gynecology (Berek & Novak, 2020)
- Sabiston Textbook of Surgery, 21st ed.
- Bailey and Love's Short Practice of Surgery, 28th ed.
- Tsiampa et al. (2024) - Systematic review: laparoscopic vs. mini-laparotomy myomectomy [PMID 37566224]
- Zhao et al. (2026) - Meta-analysis: recurrence after laparoscopic myomectomy [PMID 41846572]
- Wang et al. (2025) - Review: TCRM technique [PMID 39794046]
can you share image and steps of first recommendation surgery
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Generating Image
Here is everything consolidated - the textbook classification image, a procedural diagram, and the full operative steps.
Hysteroscopic Myomectomy (TCRM) - Images & Operative Steps
Fibroid Classification Diagram (Textbook)
This image from Berek & Novak's Gynecology shows the FIGO submucosal fibroid types your patient falls under - T:II is the type 2 fibroid (>50% invasion of myometrial wall):
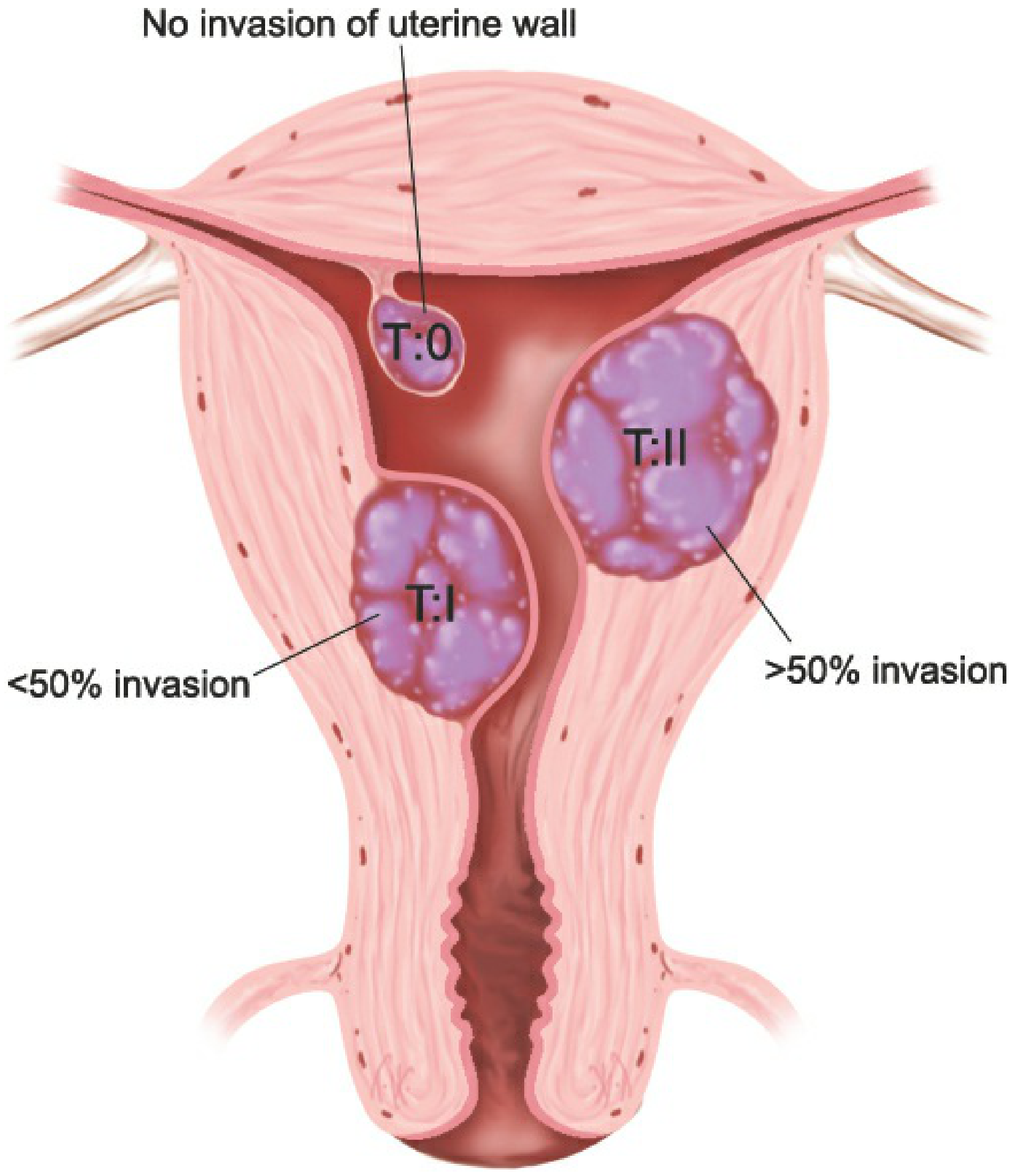
Figure 11-6, Berek & Novak's Gynecology - FIGO submucosal fibroid classification showing degree of myometrial invasion
Procedural Step Diagram
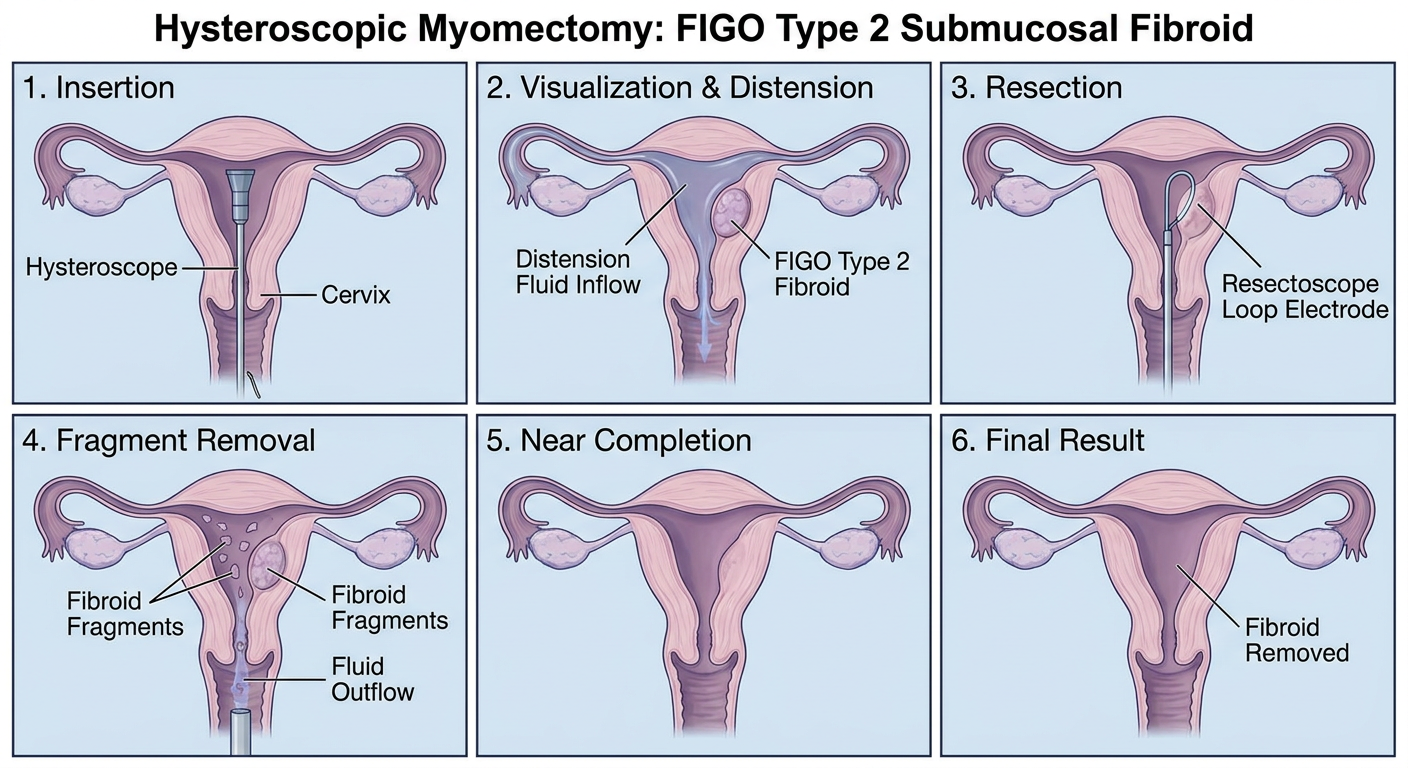
Step-by-Step Operative Technique
Preoperative Preparation
1. Preoperative imaging
- MRI (preferred) or saline infusion sonography (SIS) to map the fibroid - specifically to measure the thickness of myometrium between the fibroid and serosa. For type 2 fibroids, this is the single most important safety parameter; if the residual myometrial mantle is <5 mm, the risk of perforation with the loop electrode is significantly elevated.
- Plan for single-stage vs. two-stage procedure based on size and intramural depth.
2. GnRH agonist pretreatment (optional but strongly advisable for type 2)
- 2-3 months of GnRH agonist (e.g. leuprolide 3.75 mg IM monthly) to reduce fibroid volume by ~30% and thin the endometrium, improving hysteroscopic visualization and potentially converting a type 2 to a more favorable type 1 profile.
3. Cervical priming
- Misoprostol (Cytotec) 400 mcg vaginally 8-12 hours preoperatively to soften and partially dilate the cervix, facilitating easier and safer passage of the resectoscope.
Intraoperative Steps
Step 1 - Cervical dilation
- Under general or regional anaesthesia, dilate the cervix to Hegar 9-10 (sufficient to admit the resectoscope, typically 9 mm outer diameter).
- Dilation should be gentle and graduated to avoid false passages or perforation at the internal os.
Step 2 - Resectoscope insertion and cavity survey
- Insert the operative hysteroscope/resectoscope under continuous distension fluid flow.
- Distension media choice:
- Bipolar resectoscope → normal saline or Lactated Ringer's (isotonic; safe fluid deficit limit: 2,500 mL)
- Monopolar resectoscope → sorbitol 5%, sorbitol/mannitol, or glycine 1.5% (hypotonic; fluid deficit limit: 1,000 mL - must terminate earlier to prevent hyponatraemia)
- Modern practice strongly favours bipolar with isotonic saline to reduce electrolyte risk.
- Perform a full panoramic survey of the uterine cavity, identify the fibroid, note its relationship to the tubal ostia, assess the endometrium.
Step 3 - Resection of the intracavitary component
- Position the cutting loop beyond the fibroid (distal to it).
- Activate electrosurgical current only while drawing the loop toward the surgeon (never advancing the loop while powered - to prevent uncontrolled cutting).
- Shave the fibroid systematically in chips/slices from its most prominent intracavitary portion downward.
- Resect down to the level of the surrounding myometrium - do not go deeper.
- For fertility preservation: minimize thermal spread to surrounding normal myometrium; use short controlled bursts rather than continuous activation.
Step 4 - Fragment extraction
- Chips of fibroid tissue are removed from the cavity either:
- With a grasping forceps (polyp forceps) - retrieve visible fragments
- By capturing fragments with the loop and withdrawing the entire telescope together
- With a hysteroscopic tissue removal (HTR/intrauterine morcellator) system - mechanically cuts and aspirates simultaneously in saline; systematic reviews show equivalent complete resection rates to classical resectoscopy with no significant increase in complications
Step 5 - Dealing with the intramural component (Type 2 specific)
- After resecting the intracavitary portion, the remaining intramural fibroid mass often spontaneously contracts and is pushed into the cavity by uterine muscle contractions over the following weeks.
- Two-stage approach: If significant intramural component remains after the first resection, terminate the procedure (especially if fluid deficit limits are approaching), allow 6-8 weeks for the residual fibroid to migrate into the cavity, then perform a second hysteroscopic resection. This is the standard, safe approach for type 2 fibroids rather than risking deep resection in a single sitting.
Step 6 - Fluid monitoring throughout
- A dedicated fluid management system must be used throughout. The scrub nurse or circulating nurse calls out the running fluid deficit at regular intervals.
- Warning threshold: 750 mL deficit - increase vigilance, consider expediting.
- Stop threshold: 1,000 mL (hypotonic) / 2,500 mL (isotonic) - terminate procedure, check electrolytes, give diuretics if needed.
- If the limit is reached before resection is complete, terminate and plan a second stage.
Postoperative Steps
Step 7 - Intrauterine adhesion prevention
- Since this patient wants fertility, adhesion prevention after resection is important (type 2 fibroids carry higher adhesion risk than type 0/1 due to deeper resection).
- Options: oral estrogen (conjugated estrogens 2.5 mg/day for 30 days + progestin withdrawal) to promote endometrial regeneration; hyaluronic acid gel instillation at end of procedure.
- Second-look hysteroscopy at 4-6 weeks post-op to check for adhesions and treat early if present.
Step 8 - Pathology
- All resected tissue is sent for histopathological examination to confirm leiomyoma and exclude the rare possibility of leiomyosarcoma (important in a reproductive-age woman).
Step 9 - Fertility follow-up
- Allow 3 months of uterine healing before attempting conception (for type 2, some surgeons advise 6 months given deeper myometrial involvement).
- No myometrial scar from hysteroscopic resection, so vaginal delivery is not contraindicated and caesarean is not mandatory.
- Repeat SIS or sonohysterography at 3 months to confirm complete cavity restoration before conception attempts.
Summary Table
| Step | Action | Key Safety Point |
|---|---|---|
| 1 | Preop MRI + cervical priming | Check myometrial mantle thickness |
| 2 | Insert resectoscope, survey cavity | Use bipolar + isotonic saline |
| 3 | Resect intracavitary component with loop | Loop moves toward surgeon only; avoid deep thermal injury |
| 4 | Extract fibroid chips | Grasping forceps or HTR morcellator |
| 5 | Assess residual intramural component | Plan 2-stage if >50% remains |
| 6 | Monitor fluid deficit continuously | Stop at 1,000 mL (hypotonic) / 2,500 mL (isotonic) |
| 7 | Adhesion prevention + estrogen | Second-look hysteroscopy at 4-6 weeks |
| 8 | Send all chips to pathology | Rule out sarcoma |
| 9 | 3-6 months healing before TTC | No uterine scar = vaginal delivery permitted |
Sources: Berek & Novak's Gynecology pp. 531-533; Sabiston Textbook of Surgery pp. 2968-2052
This is a shared conversation. Sign in to Orris to start your own chat.