Portal hypertension shunting changes
Reading File
Finding Sources
Searching PubMed
"portal hypertension" AND "portosystemic collaterals"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of portal hypertension shunting changes, drawn from multiple authoritative sources.
Portal Hypertension: Collateral Shunting Changes
Mechanism of Shunt Formation
When portal pressure rises (normally 5-10 mmHg; hypertension defined as >10 mmHg, bleeding risk at >12 mmHg), blood flow in pre-existing low-volume portal-systemic anastomoses reverses direction. Rather than flowing toward the portal circulation, blood is redirected away from it into systemic veins. These collaterals do not normalize portal pressure despite becoming extensive - portal hypertension persists and progresses even with fully developed collateral networks.
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1761
The underlying driver is splanchnic arterial vasodilation mediated by nitric oxide (via eNOS), TNF-alpha, VEGF, endocannabinoids, and heme oxygenase - leading to increased portal venous inflow on top of fixed intrahepatic resistance.
Spontaneous Portosystemic Collaterals
These form at anatomical sites where portal and systemic venous beds are in close proximity:
| Site | Portal Side | Systemic Side | Clinical Result |
|---|---|---|---|
| Distal esophagus / proximal stomach | Left gastric (coronary) vein, short gastric veins | Azygos / hemiazygos system | Esophageal and gastric varices |
| Umbilicus | Paraumbilical vein (from left portal vein, vestigial remnant of umbilical vein) | Epigastric veins (superficial & inferior) | Caput medusae |
| Rectum | Superior rectal vein (inferior mesenteric vein) | Middle & inferior rectal veins (pudendal vein) | Rectal varices (not hemorrhoids) |
| Retroperitoneum | Ovarian / testicular veins, mesenteric branches | Iliac veins | Retroperitoneal varices (commoner in women) |
Medical Physiology, p. 1766; Sleisenger and Fordtran's GI and Liver Disease, p. 1761
Esophageal variceal anatomy has four distinct zones at the gastroesophageal junction:
- Gastric zone (2-3 cm below GEJ): submucosal longitudinal veins draining into short gastric and left gastric veins
- Palisade zone (2-3 cm above gastric zone): vessels in parallel ("palisade" pattern), most prone to rupture
- Perforating zone and truncal zone above this communicate with the azygos system
Sleisenger and Fordtran's, p. 1762
Gastric varices (GV) bleed at lower portal pressure gradients (~16-20 mmHg) than esophageal varices (21-23 mmHg), but GV hemorrhage is more severe with higher transfusion requirements.
Portoportal Collaterals (distinct from portosystemic)
These arise when the portal, splenic, or superior mesenteric vein occludes:
- Splenic vein occlusion (e.g., from pancreatitis): retrograde flow through short gastric veins to left gastric vein - produces isolated gastric varices ("sinistral/left-sided portal hypertension")
- Portal vein thrombosis: numerous collateral veins develop in the gastrohepatic ligament, creating portal cavernoma (cavernous transformation of the portal vein)
- Superior mesenteric vein occlusion: collateral drainage through mesenteric and paraduodenal veins
These submucosal collaterals are prone to GI tract bleeding. Fischer's Mastery of Surgery, 8th ed., p. 5462
HVPG Classification of Portal Hypertension
| Type | Wedged HVP | Free HVP | HVPG | Example |
|---|---|---|---|---|
| Prehepatic | Normal | Normal | Normal | Portal vein thrombosis |
| Presinusoidal | Normal | Normal | Normal | Schistosomiasis |
| Sinusoidal | Increased | Normal | Increased | Cirrhosis |
| Postsinusoidal | Increased | Normal | Increased | Veno-occlusive disease |
| Posthepatic (heart failure) | Increased | Increased | Normal | Right heart failure |
HVPG is only accurate for sinusoidal and postsinusoidal causes; it underestimates or misses presinusoidal and prehepatic causes. Sleisenger and Fordtran's, Table 92.1
Therapeutic Shunts (Interventional/Surgical)
These create deliberate portosystemic connections to decompress the portal system:
1. TIPS (Transjugular Intrahepatic Portosystemic Shunt)
- Stent placed between hepatic vein branch and portal vein branch via jugular approach
- Effectively reduces portal pressure and resolves varices
- Complication: hepatic encephalopathy (bypasses liver detoxification of NH3 and other toxins)
- Has largely replaced surgical shunts for refractory variceal bleeding
2. Distal Splenorenal Shunt (Warren Shunt) - Selective
- Anastomosis: splenic vein (distal) to left renal vein (end-to-side)
- Portal-azygos disconnection is performed first
- Only decompresses gastroesophageal junction varices and spleen - maintains portal hypertension in SMV/portal vein, so hepatic portal perfusion is preserved
- ~90% variceal bleeding control, significantly lower encephalopathy than total shunts
- Ascites may still develop (~20%) because hepatic sinusoidal pressure is not reduced
3. Partial Portosystemic Shunt - Partial
- 8 mm synthetic interposition graft between portal vein and IVC
- Reduces portal pressure below 12 mmHg while maintaining antegrade hepatic flow
- Rebleeding and encephalopathy rates similar to distal splenorenal shunt
- Ascites in ~20% (hepatic sinusoidal pressure not reduced)
4. Portacaval Shunt (Side-to-Side) - Total
- Portal vein to IVC, >12 mm diameter = total portal flow diversion
- Controls both variceal bleeding AND ascites (decompresses hepatic sinusoids)
- Hepatic encephalopathy in 30-40% of patients
- Variceal rebleeding <10%
- Avoided in liver transplant candidates (increases operative morbidity at transplant)
5. Rex Shunt (Mesenterico-Left Portal Bypass)
- SMV connected via jugular vein graft to intrahepatic left portal vein (Rex recessus)
- Used in extrahepatic portal vein thrombosis when intrahepatic left portal vein is patent
- Restores (rather than bypasses) portal flow to liver - low encephalopathy risk
- Treatment of choice in children with extrahepatic portal vein thrombosis
Sleisenger and Fordtran's GI and Liver Disease, pp. 1779-1782
Consequences of Shunting
- Hepatic encephalopathy: Portal blood bypasses the liver, so ammonia (NH3) and other gut-derived toxins enter the systemic circulation directly and cross the blood-brain barrier, causing acute delirium and chronic neurological deterioration.
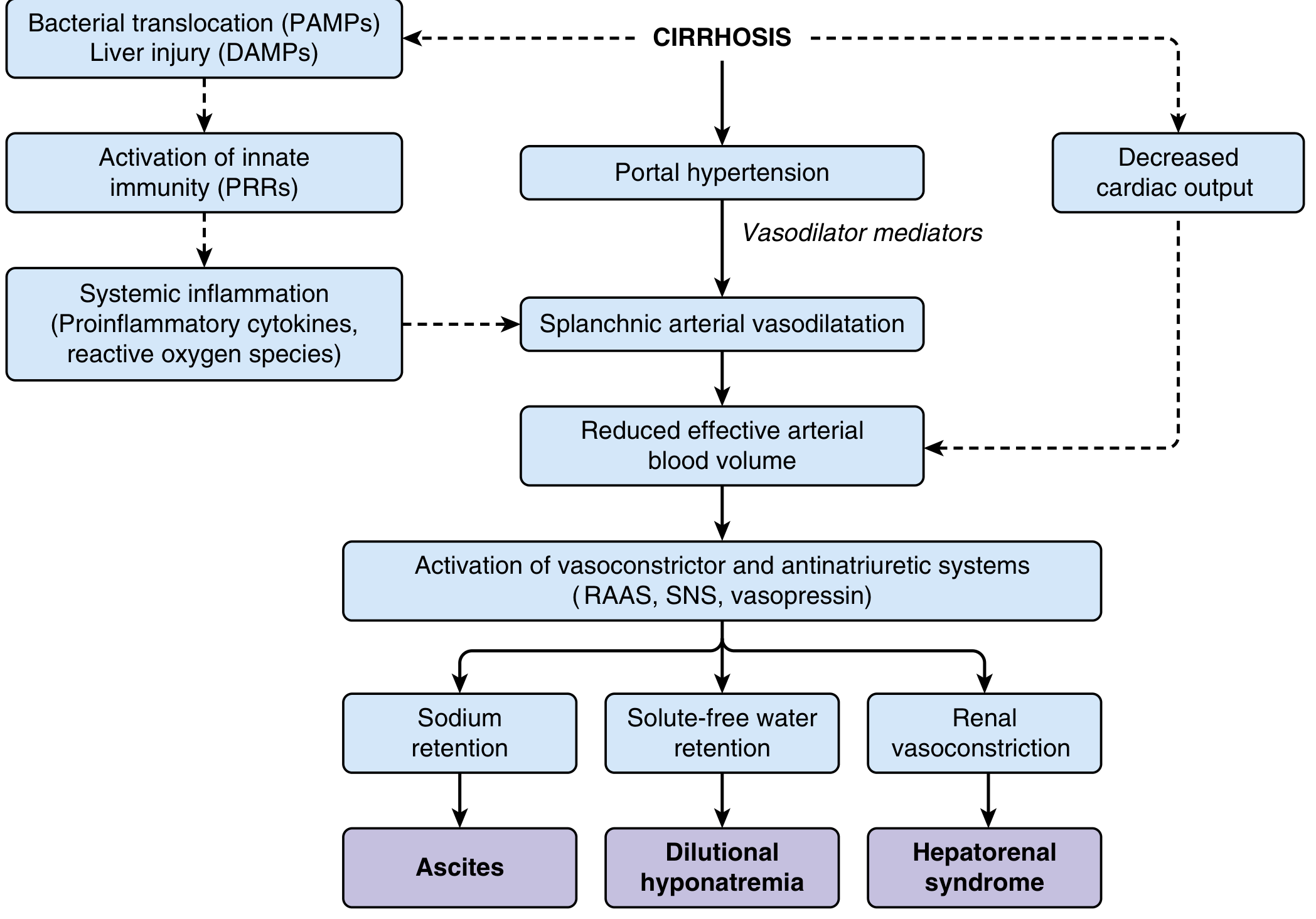
- Hyperdynamic circulation: Splanchnic vasodilation increases cardiac output, reduces SVR, and causes effective arterial hypovolemia - activating RAAS, SNS, and vasopressin, leading to sodium retention, dilutional hyponatremia, ascites, and hepatorenal syndrome.
- Incomplete decompression: Even massive collateral formation fails to normalize portal pressure, because the underlying cause (intrahepatic resistance) persists.
Key pressure thresholds to remember:
- HVPG >10 mmHg: varices begin to form
- HVPG >12 mmHg: variceal bleeding risk (virtually absent below 12)
- HVPG >20 mmHg: high-risk of early rebleeding and treatment failure
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Fischer's Mastery of Surgery 8th ed.; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.