Aids microbiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative microbiology textbooks. Let me compile the full, detailed answer.
AIDS Microbiology - A Comprehensive Review
1. Classification and Taxonomy
HIV (Human Immunodeficiency Virus) is the causative agent of AIDS (Acquired Immunodeficiency Syndrome). It belongs to:
- Family: Retroviridae
- Subfamily: Orthoretrovirinae
- Genus: Lentivirus (lenti = "slow" - causes long latency with viremia before disease)
- Types: HIV-1 (worldwide pandemic, major cause of AIDS) and HIV-2 (mainly West Africa, less virulent, slower progression)
Retroviruses are enveloped, icosahedral, single-stranded positive-sense RNA viruses that encode reverse transcriptase (RT) - an RNA-dependent DNA polymerase. This enzyme converts the RNA genome into dsDNA. Discovery of RT by David Baltimore and Howard Temin in 1970 earned them the Nobel Prize. HIV-1 was discovered by Françoise Barré-Sinoussi and Luc Montagnier (Nobel Prize 2008).
- Sherris & Ryan's Medical Microbiology, 8th Ed.
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
2. Viral Structure
HIV-1 is a spherical, enveloped virus ~100-120 nm in diameter with:
| Component | Details |
|---|---|
| Envelope | Lipid bilayer derived from host cell membrane |
| gp120 | Surface glycoprotein - binds CD4 receptor and CCR5/CXCR4 co-receptors |
| gp41 | Transmembrane glycoprotein - mediates fusion of viral envelope with host cell membrane |
| Matrix (p17) | Lines the inner surface of the envelope |
| Capsid (p24) | Cone-shaped core; important diagnostic antigen |
| Nucleocapsid (p7/p9) | Binds RNA genome |
| Genome | 2 identical copies of (+)ssRNA (~9.7 kb); diploid |
| Enzymes (in core) | Reverse transcriptase (RT), Integrase (IN), Protease (PR) |
Genome Organization (gag, pol, env + 6 accessory genes):
- gag - encodes structural proteins (MA, CA, NC)
- pol - encodes enzymes (RT, IN, PR)
- env - encodes envelope glycoproteins (gp160 → cleaved to gp120 + gp41)
- Regulatory: tat, rev
- Accessory: vif, vpr, vpu, nef
3. HIV Replication Cycle
Step-by-Step:
-
Attachment - gp120 binds to CD4 receptor on T-helper cells, macrophages, and dendritic cells. Conformational change allows binding to co-receptor CCR5 (R5 tropism, macrophage-tropic, early infection) or CXCR4 (X4 tropism, T-tropic, late infection).
-
Fusion - gp41 undergoes refolding, mediating fusion of viral and host membranes. The viral core enters the cytoplasm. Fusion inhibitor: enfuvirtide targets this step.
-
Reverse Transcription - RT converts the ssRNA genome → single-stranded cDNA → double-stranded DNA. RT has three enzymatic activities: RNA-dependent DNA polymerase, RNase H (removes RNA template), and DNA-dependent DNA polymerase. NRTIs and NNRTIs target this step.
-
Nuclear Import & Integration - dsDNA forms a preintegration complex (with viral IN and Vpr), enters the nucleus, and integrates into the host chromosome at preferentially actively transcribed regions, forming the provirus. The cell is permanently infected; provirus is replicated as long as the cell divides. Integrase inhibitors (dolutegravir, raltegravir) target this step.
-
Transcription - Host RNA polymerase II transcribes the provirus. LTR sequences contain promoter and enhancer elements. Full-length genomic RNA and spliced mRNAs are produced. Viral protein Tat greatly enhances transcription; Rev regulates nuclear export of unspliced/singly-spliced RNA.
-
Translation - Gag, Gag-Pol polyproteins (from genomic RNA); Env gp160 precursor. Viral protease (PR) cleaves Gag-Pol into MA, CA, NC, RT, IN, and PR. Host protease cleaves gp160 → gp120 + gp41. Protease inhibitors (ritonavir, darunavir, etc.) target this step.
-
Assembly & Budding - New virions assemble at the plasma membrane. Budding occurs; immature virion is released and undergoes maturation via protease cleavage.
Key point: Activation of CD4+ T-lymphocytes greatly increases viral transcription, explaining why antigen stimulation during HIV infection accelerates disease progression.
- Sherris & Ryan's Medical Microbiology, 8th Ed.
4. Pathogenesis
4a. Target Cells
HIV infects cells expressing CD4: CD4+ T-lymphocytes (primary), macrophages, dendritic cells, microglial cells (CNS).
4b. Course of Infection
| Stage | Timeframe | Key Events |
|---|---|---|
| Primary/Acute HIV | 2-4 weeks post-exposure | Intense viral replication, high viremia (within 7-28 days), dissemination to lymphoid tissues; flu/mono-like illness (fever 97%, lymphadenopathy 77%, pharyngitis 73%, rash 70%, myalgias) = Acute Retroviral Syndrome |
| Seroconversion | 3-12 weeks | IgM anti-HIV appears first (2 weeks), then IgG. Viral load drops as immune response activates |
| Clinical Latency (Chronic) | 8-10 years (untreated) | Continued low-level viral replication, slowly declining CD4 count, patient largely asymptomatic. Virus establishes reservoirs in GALT, lymph nodes, resting T-cells, macrophages |
| AIDS | CD4 <200/µL | Severe immunodeficiency; opportunistic infections, malignancies, neurological complications |
4c. CD4 T-Cell Depletion Mechanisms
- Direct cytolysis by viral budding
- Apoptosis triggered by gp120-CD4 crosslinking
- CTL (CD8+) killing of infected cells
- Syncytia formation with gp120-positive cells
- Chronic immune activation and exhaustion
4d. Viral Reservoirs
HIV establishes latent reservoirs in:
- Resting memory CD4+ T-cells (main reservoir)
- Gut-associated lymphoid tissue (GALT)
- CNS macrophages and microglial cells
- Lymph nodes
These reservoirs are impervious to ART and are the major barrier to cure.
5. AIDS Definition (CDC)
AIDS is defined by either:
- CD4+ T-cell count < 200 cells/µL, OR
- Presence of an AIDS-defining condition regardless of CD4 count
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
6. AIDS-Defining Opportunistic Infections
| Category | Organisms/Diseases |
|---|---|
| Protozoal | Toxoplasma gondii (brain abscess), Cryptosporidium (diarrhea), Isospora belli |
| Fungal | Pneumocystis jirovecii pneumonia (PCP - commonest OI), Candida (esophagitis, oral thrush), Cryptococcus neoformans (meningitis), Histoplasma, Coccidioides |
| Bacterial | Mycobacterium avium complex (MAC), M. tuberculosis, Salmonella (recurrent bacteremia) |
| Viral | CMV (retinitis, colitis, esophagitis, pneumonia), HSV (severe mucocutaneous disease), VZV (disseminated), JC virus (PML - progressive multifocal leukoencephalopathy), EBV |
| AIDS-defining Malignancies | Kaposi sarcoma (HHV-8), Primary CNS lymphoma, Burkitt/lymphoblastic lymphoma, Invasive cervical carcinoma |
| Other | HIV encephalopathy (AIDS dementia complex), HIV wasting syndrome (>10% weight loss + >1 month diarrhea/weakness and fever) |
- Medical Microbiology 9e; Jawetz Medical Microbiology
7. Transmission
High viral titers are found in blood and semen. Routes:
- Sexual contact - anal and vaginal (most common globally); oral-genital less efficient. Co-existing STIs (syphilis, gonorrhea, HSV-2) increase risk up to 100-fold.
- Parenteral - IV drug use (needle sharing), blood transfusions, clotting factor concentrates (pre-1985), needle-stick injuries in healthcare workers
- Mother-to-child (vertical) - in utero, intrapartum (most common), breastfeeding
Not transmitted via air, dust, fomites, casual contact - highly susceptible to factors affecting surface tension as an enveloped virus.
8. Laboratory Diagnosis
| Test | Details |
|---|---|
| 4th-generation ELISA (screening) | Detects HIV-1/2 antibodies + p24 antigen; window period ~2-4 weeks |
| Western blot / HIV-1/2 differentiation assay | Confirmatory; requires bands for gp120/gp160, gp41, p24 |
| HIV RNA PCR (viral load) | Earliest marker (~7-28 days); used for monitoring, diagnosis in acute phase, neonates |
| CD4+ T-cell count | Monitors immune status; guides prophylaxis and ART initiation |
| p24 antigen | Detectable in early acute phase before antibodies; declines as anti-p24 rises |
Window period: The time between infection and detectable antibody (3-12 weeks). Early infection is detected by HIV RNA PCR or p24 antigen. The 4th-gen test reduces the window period significantly.
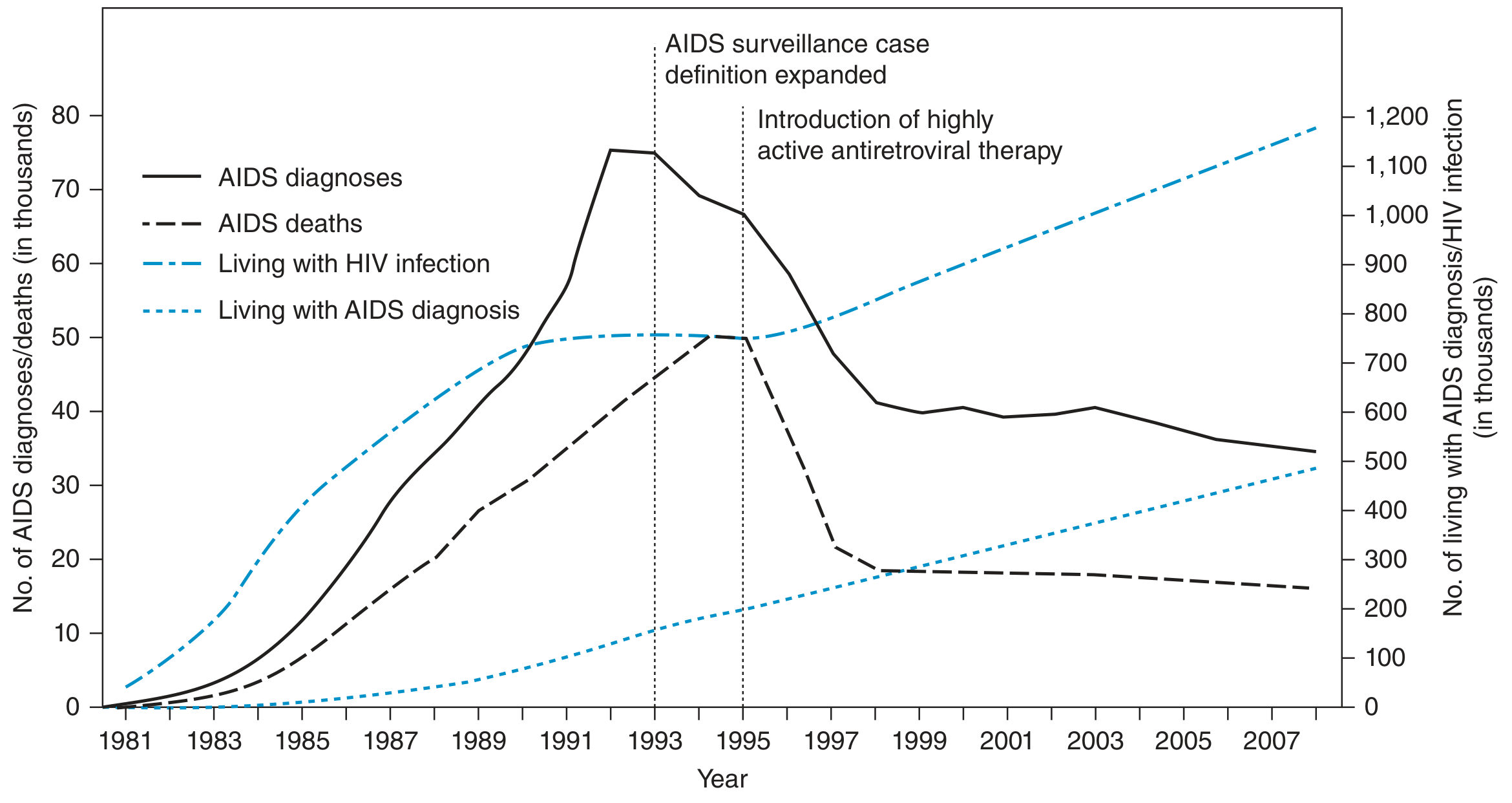
9. Epidemiology
- ~38 million people worldwide living with HIV; 67% in Sub-Saharan Africa
- 1.2 million in the United States
- First recognized in 1981 in the US: unusual Kaposi sarcoma and PCP in men who have sex with men (MSM)
- Epidemic expanded to heterosexuals, hemophiliacs, IV drug users
- HAART (1996) dramatically reduced AIDS deaths and morbidity (see graph below)
10. Antiretroviral Therapy (ART)
| Drug Class | Mechanism | Examples |
|---|---|---|
| NRTIs | Nucleoside/nucleotide RT inhibitors; chain terminators | Zidovudine (AZT), Tenofovir, Emtricitabine, Lamivudine, Abacavir |
| NNRTIs | Non-nucleoside RT inhibitors; allosteric binding | Efavirenz, Nevirapine, Rilpivirine, Etravirine |
| Protease Inhibitors (PIs) | Block viral protease; immature virions | Ritonavir, Darunavir, Atazanavir, Saquinavir |
| Integrase Strand Transfer Inhibitors (INSTIs) | Block viral DNA integration | Dolutegravir, Raltegravir |
| Fusion Inhibitors | Block gp41-mediated membrane fusion | Enfuvirtide |
| Entry Inhibitors (CCR5 antagonists) | Block CCR5 co-receptor | Maraviroc |
Current first-line regimen: 2 NRTIs + 1 INSTI (e.g., tenofovir + emtricitabine + dolutegravir in a single tablet).
Goals of ART:
- Reduce viral load to undetectable levels (<50 copies/mL)
- Raise CD4 count
- Prevent opportunistic infections
- Prevent transmission (U = U: Undetectable = Untransmittable)
Key limitations: No cure (viral reservoirs persist), drug resistance if non-adherent, lifelong treatment required.
Prevention of mother-to-child transmission: AZT regimen during pregnancy, labor, and neonatal period reduces transmission from 25-30% → <2%.
PrEP (Pre-Exposure Prophylaxis): Tenofovir-based regimens highly effective at preventing new infections in high-risk individuals.
11. Key Microbiological Features Summary
| Feature | HIV |
|---|---|
| Family | Retroviridae |
| Genus | Lentivirus |
| Genome | (+)ssRNA, diploid |
| Envelope | Yes (lipid bilayer) |
| Key enzymes | RT, Integrase, Protease |
| Key surface proteins | gp120, gp41 |
| Primary receptor | CD4 |
| Co-receptors | CCR5 (R5-tropic), CXCR4 (X4-tropic) |
| Integration | Into host chromosome as provirus |
| Diagnostic antigen | p24 |
| Cytopathic effect | CD4+ T-cell depletion, syncytia |
Sources:
- Sherris & Ryan's Medical Microbiology, 8th Ed.
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
- Medical Microbiology, 9th Ed.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Janeway's Immunobiology, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.