Describe the anatomy of parapharyngeal space in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
parapharyngeal space anatomy tumors
Searching the Web
parapharyngeal space anatomy RGUHS ENT 20 marks deep neck spaces
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
ANATOMY OF THE PARAPHARYNGEAL SPACE
RGUHS MS/DNB ENT - 20 Marks Answer
INTRODUCTION
The parapharyngeal space (PPS) - also called the lateral pharyngeal space, pharyngomaxillary space, pterygomaxillary space, pterygopharyngeal space, and peripharyngeal space - is a potential deep neck space filled with fat and areolar tissue lying laterally on either side of the pharynx. It serves as the anatomic epicenter of the suprahyoid neck around which all other fascial spaces are organized. Despite being the site of only 0.5% of all head and neck masses, its intimate relations with vital neurovascular structures make it surgically significant.
(Scott-Brown's Otorhinolaryngology, Olsen KD 1994; Cummings Otolaryngology; K.J. Lee's Essential Otolaryngology)
DIAGRAM 1 - The Parapharyngeal Space as an Inverted Pyramid (Coronal/Lateral View)
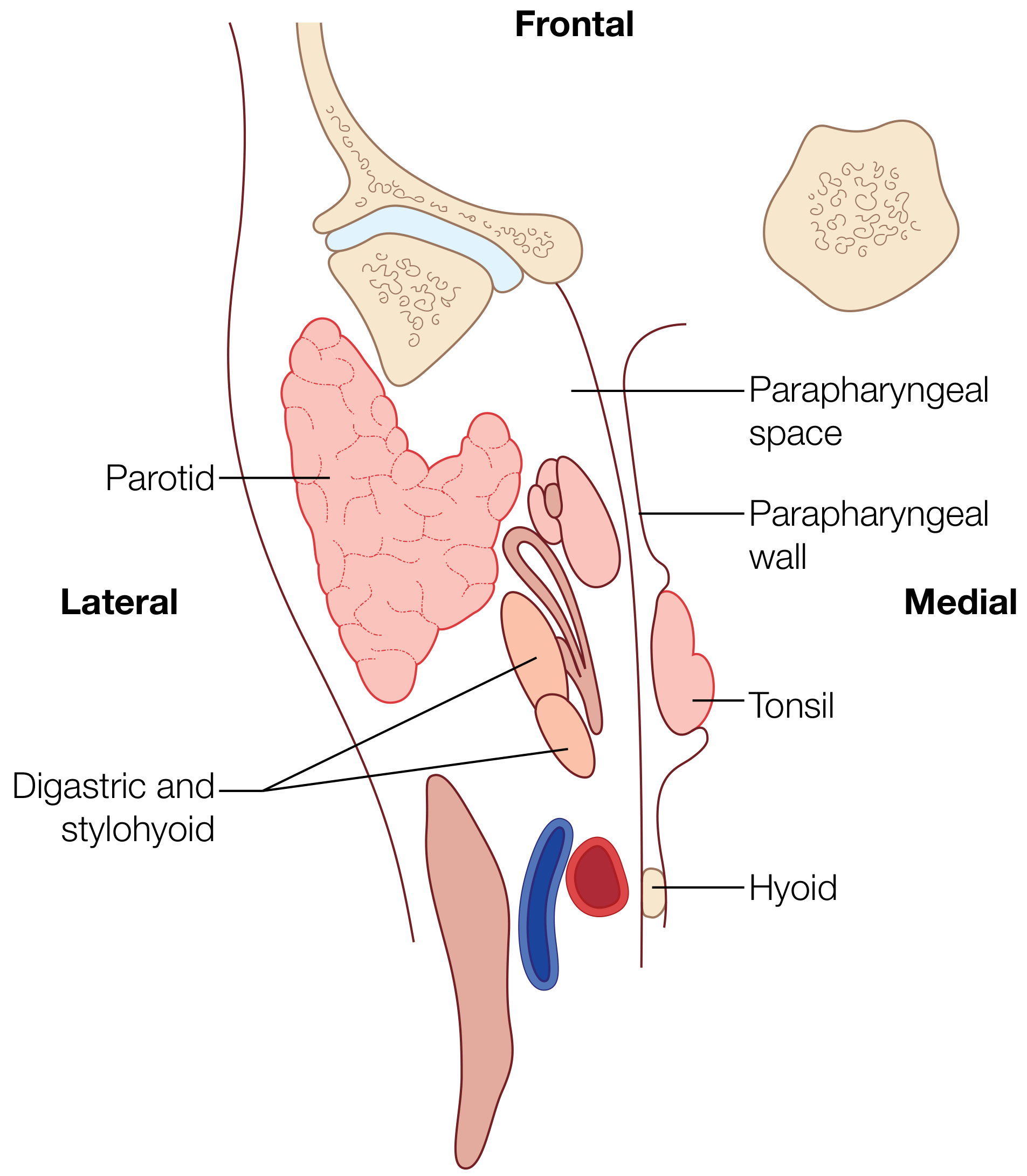
SHAPE
The parapharyngeal space is classically described as an inverted pyramid (or inverted cone):
- Base - superiorly at the skull base (sphenoid and temporal bones, including the jugular foramen, hypoglossal canal, and foramen lacerum)
- Apex - inferiorly at the greater cornu of the hyoid bone
- Three sides - medial, lateral, and posterior
- Anterior leading edge - the pterygomandibular raphe
In the axial plane it appears triangular; in the coronal plane it has an hourglass shape (thicker at skull base and hyoid levels, thinner in midneck).
BOUNDARIES
| Wall | Structure |
|---|---|
| Superior (base) | Skull base - petrous temporal bone, sphenoid bone (middle cranial fossa) |
| Inferior (apex) | Greater cornu of the hyoid bone |
| Medial | Pharyngobasilar fascia + superior pharyngeal constrictor muscle (buccopharyngeal membrane) |
| Lateral | Medial pterygoid muscle, ramus of mandible, deep lobe of parotid gland; below mandible - fascia of posterior belly of digastric |
| Anterior | Pterygomandibular raphe |
| Posterior | Prevertebral fascia; carotid sheath posterolaterally; retropharyngeal space posteromedially |
(K.J. Lee's Essential Otolaryngology, p. 699; Scott-Brown's Vol 2, Chapter 11)
DIAGRAM 2 - Axial Cross-Section of the Parapharyngeal Space
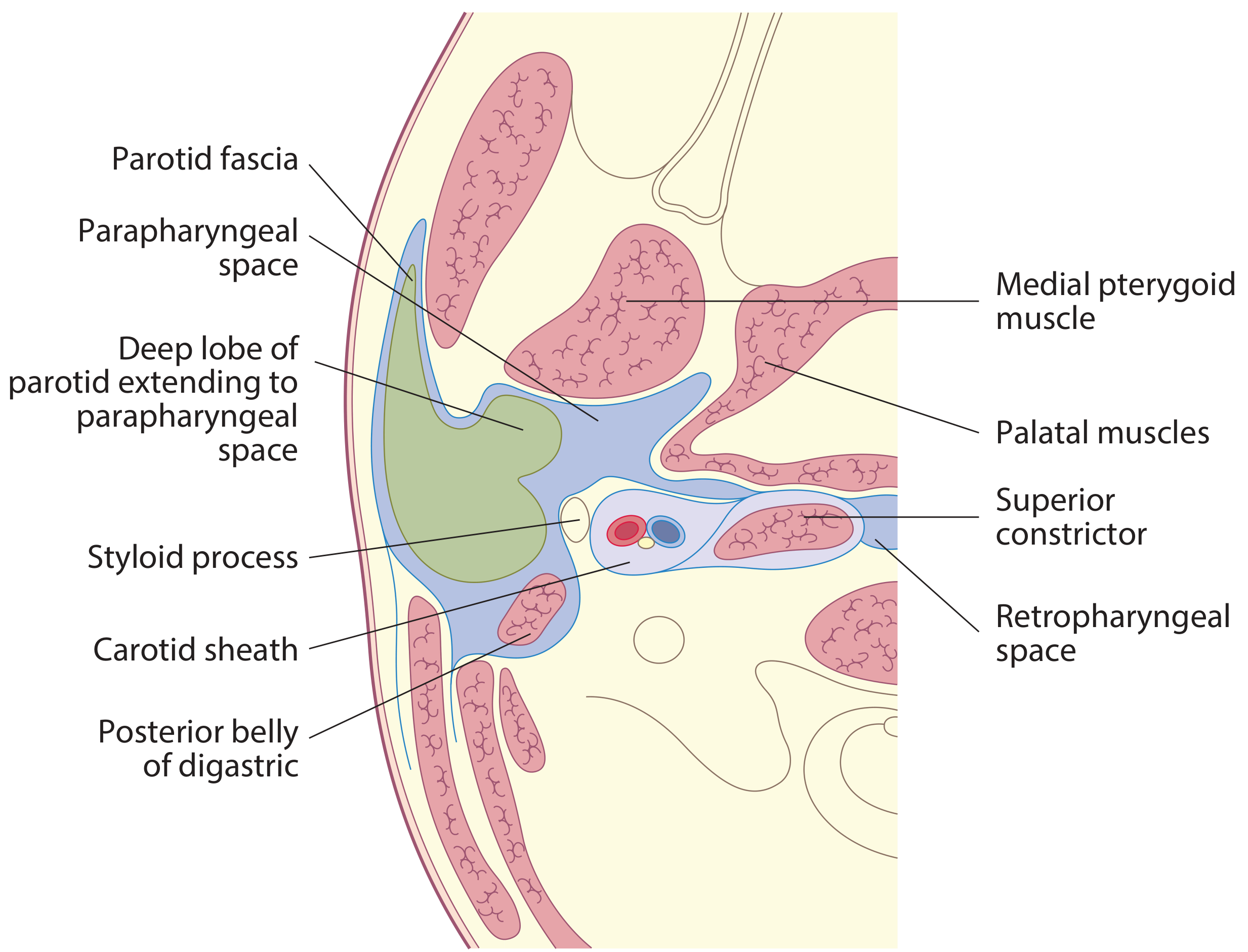
FASCIAL DIVISIONS - THE STYLOID APPARATUS
The PPS is divided into two compartments by a critical fascial condensation:
The Aponeurosis of Zuckerkandl and Testut
This fascia joins the styloid process to the tensor veli palatini muscle and extends to the skull base. It is the true anatomical divider between:
- Prestyloid (anterior) compartment
- Poststyloid / Retrostyloid (posterior/neurovascular) compartment
(Scott-Brown's Vol 2, Scott-Brown's Vol 1 [9781138094634])
FLOW CHART 1 - Division of PPS by Styloid Apparatus
PARAPHARYNGEAL SPACE
|
Styloid Process + Aponeurosis of Zuckerkandl & Testut
(Tensor-veli palatini fascia)
|
______|______
| |
PRESTYLOID POSTSTYLOID
(Anterior) (Posterior / Neurovascular)
Muscular Vascular
compartment compartment
CONTENTS
DIAGRAM 3 - Detailed Horizontal Section Showing All Compartment Contents
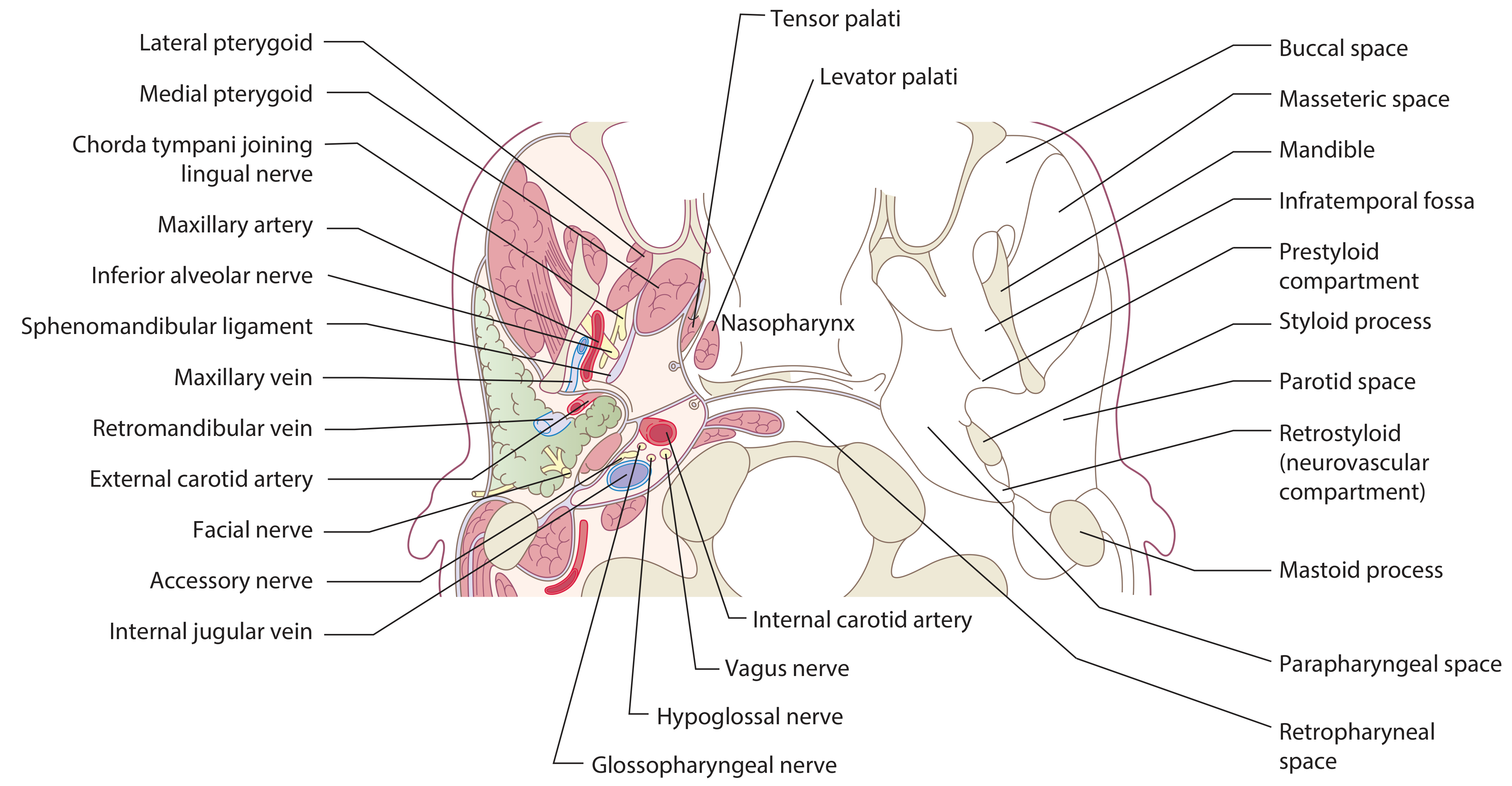
A. PRESTYLOID (ANTERIOR/MUSCULAR) COMPARTMENT
This compartment lies anterior and lateral to the styloid process. The medial wall is distensible (pharynx) and the lateral wall is relatively immobile (mandible, pterygoids, parotid).
| Structure | Notes |
|---|---|
| Fat (main component) | Fibrofatty areolar tissue - acts as radiological marker space |
| Lymph nodes | Regional lymphatics |
| Internal (deep) maxillary artery | Branch of external carotid; variable course |
| Ascending pharyngeal artery | Branch of external carotid |
| Pharyngeal venous plexus | Venous drainage |
| Inferior alveolar nerve | Branch of V3 (mandibular division CN V) |
| Lingual nerve | Branch of V3 |
| Auriculotemporal nerve | Branch of V3 |
| Small branch to tensor veli palatini | Branch of trigeminal |
| Ectopic salivary gland tissue | Origin of de novo pleomorphic adenomas |
| Deep lobe of parotid gland | Enters through stylomandibular tunnel |
| Medial and lateral pterygoid muscles | Form part of lateral wall |
(K.J. Lee's p. 699; Cummings Otolaryngology; Scott-Brown's Ch. 11)
B. POSTSTYLOID (POSTERIOR/NEUROVASCULAR) COMPARTMENT
Also called the retrostyloid or carotid space (some authors). Contains the major neurovascular bundle of the neck:
| Structure | Notes |
|---|---|
| Internal carotid artery (ICA) | In carotid sheath |
| Internal jugular vein (IJV) | In carotid sheath |
| Vagus nerve (CN X) | Between ICA and IJV in carotid sheath |
| Glossopharyngeal nerve (CN IX) | Exits jugular foramen, passes through space |
| Accessory nerve (CN XI) | Immediately curves posterolaterally, medial to styloid |
| Hypoglossal nerve (CN XII) | Emerges from anterior condylar foramen, spirals lateral |
| Cervical sympathetic chain | Behind carotid sheath, anterior to prevertebral fascia; ends superiorly at superior cervical ganglion |
| Glomus bodies (paraganglia) | Origin of glomus jugulare/vagale tumors |
| Lymph nodes | Jugulodigastric group |
(Scott-Brown's Vol 2 p. 1252-1254; K.J. Lee's p. 699-700)
FLOW CHART 2 - Contents of the Two Compartments
PRESTYLOID COMPARTMENT POSTSTYLOID COMPARTMENT
(Anterior / Muscular) (Posterior / Neurovascular)
| |
Fat (main component) Internal Carotid Artery
Lymph nodes Internal Jugular Vein
Deep lobe parotid CN IX (Glossopharyngeal)
Ectopic salivary tissue CN X (Vagus)
Internal maxillary artery CN XI (Accessory)
Ascending pharyngeal artery CN XII (Hypoglossal)
Pharyngeal venous plexus Cervical Sympathetic Chain
CN V3 branches Glomus bodies
- Inferior alveolar Lymph nodes
- Lingual
- Auriculotemporal
Pterygoid muscles
THE STYLOMANDIBULAR TUNNEL
A condensation of cervical fascia forms a band from the apex of the styloid process to the angle and posterior border of the mandible - the stylomandibular ligament. Together with the posterior border of the mandible anteriorly, this creates the stylomandibular tunnel.
- The deep lobe of the parotid passes through this tunnel
- Deep lobe tumors extending into the PPS through this tunnel produce a "dumbbell-shaped" tumour
- The stylomandibular tunnel is surgically important as it limits exposure in transcervical approaches
(Scott-Brown's Ch. 11, Olsen 1994)
COMMUNICATIONS OF THE PPS
The PPS is the "hub" of deep neck spaces and communicates with:
PARAPHARYNGEAL SPACE (Central Hub)
|
_____|_______________________________
| | | | |
Peritonsillar Retro- Parotid Masticator Submandibular
space pharyngeal space space space
space
| |
(medially) (posteriorly and bilateral
PPS communicate with each other)
|
DANGER SPACE
|
Posterior mediastinum
(Scott-Brown's Ch. 35 p. 594)
Key communications:
- Peritonsillar space - most common source of infection (tonsillar abscess spreading to PPS)
- Retropharyngeal space - posteriorly (bilateral PPS communicate through this)
- Parotid space - laterally via the stylomandibular tunnel (deficient fascia)
- Masticator space - anterolaterally (dental/odontogenic source)
- Submandibular space - inferiorly (origin of Ludwig's angina spreading upward)
- Carotid sheath runs through the poststyloid PPS
FLOW CHART 3 - Radiological Significance of PPS Fat Displacement
The PPS fat acts as a pivotal marker space in neck imaging (CT/MRI). Direction of PPS fat displacement indicates the origin of an adjacent lesion:
DIRECTION OF PPS FAT DISPLACEMENT → SPACE OF ORIGIN
|
_______|_______________________________________
| | | | |
Postero- Antero- Postero- Antero- Antero-
medial medial lateral lateral medial
| | | | |
Masticator Parotid Pharyngeal Retro- Carotid
space space mucosal pharyngeal space
space / danger /
prevertebral
(Cummings Otolaryngology, Ch. 8 - Imaging)
With CT: PPS fat = low-density marker
With MRI T1WI: PPS fat = bright signal (best sequence for PPS mapping)
APPLIED ANATOMY - PATHOLOGY AND CLINICAL IMPORTANCE
A. Infections
- PPS abscess is the "central space" for deep neck infections
- Most common source: peritonsillar abscess spreading laterally through superior constrictor
- Also from: odontogenic (submandibular → PPS), parotitis, masticator space infection
- Clinical features: Trismus (pterygoid inflammation), medial displacement of tonsil and lateral pharyngeal wall, neck swelling may be absent, airway compromise
- Spread of untreated PPS abscess: → retropharyngeal space → danger space → posterior mediastinum (descending necrotizing mediastinitis)
B. Tumors of the PPS
Account for 0.5% of all head and neck masses. Riffat et al. (2014) systematic review of 1143 cases:
| Category | % |
|---|---|
| Salivary gland tumors (prestyloid) | 45% |
| Neurogenic tumors (poststyloid) | ~33% |
| Miscellaneous (branchial cyst, hemangioma, ICA aneurysm) | 12% |
| Metastatic | 3% |
| Lymphoid | 2% |
Salivary gland tumors (prestyloid):
- Benign 75% - Pleomorphic adenoma (64% of benign), Warthin's, myoepithelioma
- Malignant - Adenoid cystic carcinoma, mucoepidermoid carcinoma
Neurogenic tumors (poststyloid):
- Paraganglioma (52% of neurogenic): carotid body tumor, glomus vagale, glomus jugulare
- Schwannoma (27%): vagal, sympathetic chain
- Neurofibroma (9%)
Key radiological sign: Prestyloid lesions displace carotid sheath posteromedially (fat pad moves posteromedially). Poststyloid lesions displace fat anteriorly.
SURGICAL APPROACHES TO THE PPS
SURGICAL APPROACHES TO PPS
|
_________|__________________________
| | |
CERVICOTOMY TRANSPAROTID- TRANSORAL
(Transcervical) TRANSCERVICAL (Classical + TORS)
| | |
For poststyloid Dumbbell tumors Small benign
neurogenic Deep lobe ectopic salivary
tumors parotid tumors tumors
(best vascular (most common independent of
control) approach) parotid
Mandibulotomy / Lip-split approach: For large tumors requiring wide vascular control.
TORS (Transoral Robotic Surgery): Recent advance - see below.
RECENT ADVANCES (RGUHS / PG Level)
1. Transoral Robotic Surgery (TORS) for PPS Tumors
- FDA-approved since 2009 for oropharyngeal lesions
- Da Vinci robotic system: 3D high-resolution magnified visualization, tremor filtration, motion scaling
- Allows delicate dissection around neurovascular structures
- Best suited for ectopic salivary gland prestyloid tumors independent of deep lobe parotid
- Not suitable for deep lobe parotid extensions (require transparotid approach)
- Addresses earlier concerns about tumor spillage and hemorrhage control in transoral approaches
- (Scott-Brown's Ch. 11, p. 202; [Vogl TJ et al., Rofo 2025, PMID 39631740])
2. Advanced Imaging
- MRI with fat suppression sequences + gadolinium is now the gold standard for PPS mapping
- Differentiates prestyloid vs. poststyloid lesions with high accuracy
- Determines relationship of tumor to deep lobe parotid (critical for surgical planning)
- 4D-CT for paragangliomas to assess vascularity and feeding vessels
- Image-guided FNA cytology: Improved preoperative histological diagnosis
- (Rai P et al., Clin Radiol 2024, [PMID 39307678]; Cummings Otolaryngology)
3. Endoscopic Transoral Anatomy (Step-wise)
- Better understanding of transoral cross-sectional anatomy of PPS has refined surgical approaches
- Lim CM et al. described transoral anatomy of the tonsillar fossa and lateral parapharyngeal wall
- (Scott-Brown's Ch. 11 references)
4. Systematic Review Evidence (Riffat et al. 2014)
- 1143 PPS tumors over 20 years: 82% benign, 18% malignant
- ~70 different histological subtypes identified
- Changed understanding of tumor frequency and operative planning
5. Neurological Complications
- Recent systematic review (Faisal M et al., Int Arch Otorhinolaryngol 2023, [PMID 36714902]) documented neurological complications in benign PPS tumors, emphasizing careful preoperative nerve mapping
DHINGRA, HAZARIKA, STELL & MARAN, ZAKIR HUSSAIN - KEY TEACHING POINTS
(Note: These Indian/classic ENT textbooks are not in the digital library, but their standard teaching content on PPS anatomy is summarized from established curriculum references below)
Dhingra (Diseases of Ear Nose Throat):
- Describes PPS as an inverted cone, emphasizes styloid process division
- Pre-styloid: fat, deep parotid lobe, maxillary artery, V3 branches
- Post-styloid (carotid space): ICA, IJV, CN IX-XII, sympathetic chain
Hazarika (Textbook of ENT and Head & Neck Surgery):
- Emphasizes communication with retropharyngeal space and danger space
- Clinical importance: PPS abscess as "crossroads" infection; airway management priority
Stell & Maran (Head and Neck Surgery):
- Detailed surgical anatomy with emphasis on the stylomandibular tunnel
- Transparotid-transcervical as the standard surgical approach
- Dumbbell tumors of parotid deep lobe extending through tunnel
Zakir Hussain (Short Cases in ENT):
- Summary mnemonics for PPS contents
- Displacement signs on imaging as RGUHS exam favorites
SUMMARY TABLE - At a Glance
| Feature | Prestyloid | Poststyloid |
|---|---|---|
| Also called | Muscular compartment | Neurovascular / Carotid space |
| Main contents | Fat, deep parotid, V3 branches | ICA, IJV, CN IX-XII, sympathetic |
| Common tumors | Pleomorphic adenoma, Warthin's | Paraganglioma, Schwannoma |
| PPS fat displaced | Posteromedially | Anteriorly |
| Surgical approach | Transparotid-transcervical or TORS | Transcervical (best vascular control) |
| Radiological T1 MRI | Bright fat | Vascular flow voids |
FLOW CHART 4 - Applied Anatomy Summary
PARAPHARYNGEAL SPACE - APPLIED ANATOMY
Shape: Inverted Pyramid
Base: Skull base (petrous temporal + sphenoid)
Apex: Greater cornu of hyoid
Walls: Medial (superior constrictor), Lateral (pterygoids + mandible + parotid),
Posterior (prevertebral fascia), Anterior (pterygomandibular raphe)
|
↓
Divided by STYLOID PROCESS + Aponeurosis of Zuckerkandl & Testut
|
______|______
| |
PRESTYLOID POSTSTYLOID
(Ant) (Post)
Fat ICA + IJV
Deep parotid CN IX, X, XI, XII
V3 branches Sympathetic chain
Max artery Paraganglia
|
↓
Communications with 5 spaces:
Peritonsillar | Retropharyngeal | Parotid | Masticator | Submandibular
|
↓
Clinical Significance:
Infection (PPS abscess) → Mediastinitis
Tumors (0.5% HN masses) → 82% benign
Imaging: PPS fat as pivot marker
Surgery: Transcervical / Transparotid-transcervical / TORS
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9781138094642), Ch. 11 - Tumors of the Parapharyngeal Space; Ch. 35 - Deep Neck Spaces
- Scott-Brown's Vol 2 (9781138094634), Ch. 98 - Anatomy of the Temporal Bone and Parapharyngeal Space
- Cummings Otolaryngology Head and Neck Surgery (9780323612173), Ch. 8 - Imaging of the Suprahyoid Neck; Ch. 115 - Neoplasms of the Parapharyngeal Space
- K.J. Lee's Essential Otolaryngology (9781260122237), Ch. 37 - Parapharyngeal Space
- Olsen KD. Tumors of the parapharyngeal space. Laryngoscope 1994;104(5 Suppl 63):1-28.
- Riffat F et al. A systematic review of 1143 parapharyngeal space tumors reported over 20 years. Oral Oncol 2014.
- Rai P et al. Beyond the throat: Imaging of parapharyngeal space lesions. Clin Radiol 2024 PMID 39307678
- Vogl TJ et al. Parapharyngeal Space: Diagnostic Imaging and Intervention. Rofo 2025 PMID 39631740
- Faisal M et al. Neurological Complications in Benign PPS Tumors. Int Arch Otorhinolaryngol 2023 PMID 36714902
- Rigsby RK & Bhatt AA. Primary Pathology of the Parapharyngeal Space. Clin Neuroradiol 2023 PMID 37380900
RGUHS Exam Tip: For a 20-mark question, examiners expect: (1) Definition + synonyms, (2) Shape and boundaries in tabular form, (3) Contents of both compartments clearly separated, (4) Communications, (5) Applied anatomy - infections and tumors, (6) Radiological significance of PPS fat displacement, (7) Surgical approaches, (8) Recent advances (TORS, robotic surgery, advanced MRI). Draw at minimum 2 diagrams: the inverted pyramid (lateral view) and an axial cross-section. The "dumbbell tumor" concept and stylomandibular tunnel are high-yield points frequently asked in RGUHS/NBE theory papers.
This is a shared conversation. Sign in to Orris to start your own chat.