Rheumatic heart disease
Reading File
Finding Sources
Searching PubMed
"rheumatic heart disease"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Rheumatic heart disease (RHD) is chronic valvular heart damage caused by prior acute rheumatic fever after untreated or undertreated group A streptococcal infection (usually pharyngitis).
High-yield summary
- Cause: autoimmune cross-reactivity after strep infection, not direct bacterial invasion of valves.
- Main valve affected: mitral valve (nearly always), then aortic valve.
- Typical lesion progression:
- early: valvular regurgitation
- late: fibrosis, commissural fusion, chordal thickening/shortening -> stenosis (classic mitral stenosis)
- Classic pathology:
- acute RF carditis: Aschoff bodies, verrucae along valve closure lines
- chronic RHD: thickened fibrotic leaflets, fused commissures, "fish-mouth" mitral stenosis
- Burden: now uncommon in many high-income settings, but still a major cause of cardiovascular morbidity/mortality in many low-resource regions.
Clinical picture
- Acute rheumatic fever usually appears about 2 to 3 weeks after strep pharyngitis.
- Jones-based manifestations include carditis, arthritis, chorea, erythema marginatum, subcutaneous nodules.
- RHD often presents years later with progressive valvular disease:
- dyspnea, reduced exercise tolerance
- palpitations/atrial fibrillation
- heart failure symptoms
- embolic risk (especially with enlarged left atrium/thrombus in mitral stenosis)
Diagnosis
- Echocardiography is central for detecting and grading valvular involvement (including subclinical carditis in acute RF and latent RHD in endemic areas).
- ARF diagnosis is clinical (Jones criteria with evidence of recent streptococcal infection); there is no single definitive test.
Management principles
- Secondary prophylaxis is essential to prevent recurrent ARF and worsening valve injury.
- Common regimen: intramuscular benzathine penicillin G every 4 weeks, long duration (often at least 10 years; sometimes longer depending on severity/risk).
- Treat valvular complications per severity:
- medical therapy for heart failure/rhythm control
- anticoagulation when indicated (for example AF with mitral stenosis)
- intervention for advanced disease: balloon mitral valvotomy (selected cases), valve repair/replacement when needed.
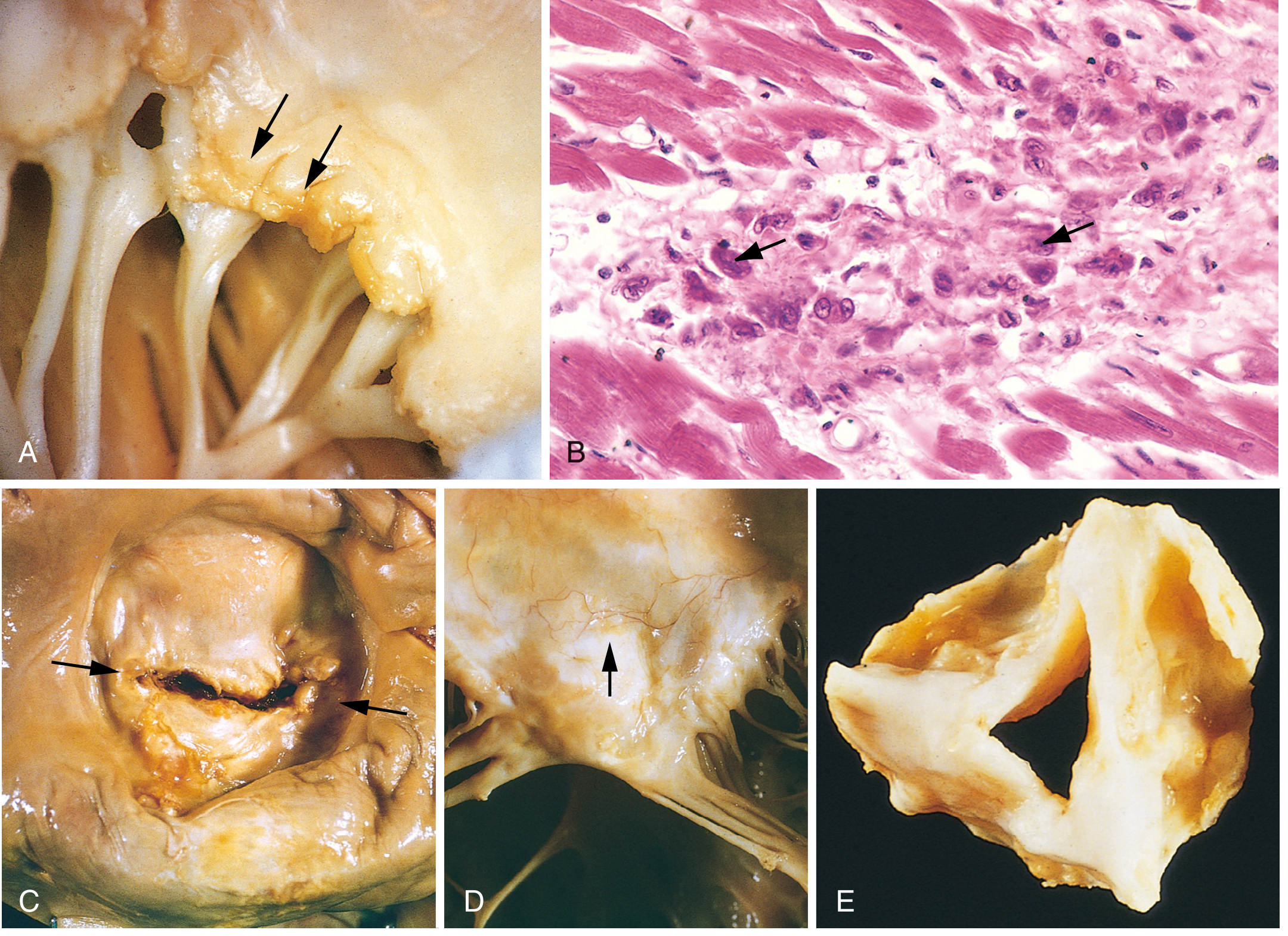
Pathology image (RHD)
This figure shows acute and chronic rheumatic valvular pathology (verrucae, Aschoff-body histology, commissural/chordal fibrosis, stenotic deformity):
Recent evidence check (last 2 years)
Recent systematic reviews/meta-analyses emphasize that prevention and adherence to secondary penicillin prophylaxis remain decisive for outcomes:
- PMID: 39542478
- PMID: 39312290
- PMID: 39960383
No major contradiction to core textbook principles, but these reviews reinforce that implementation quality (especially long-term prophylaxis adherence and timely valve intervention) strongly affects progression and outcomes.
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 525-527
- Goldman-Cecil Medicine, p. 3043-3044
This is a shared conversation. Sign in to Orris to start your own chat.