Anti arrhythmic drugs pharmacology 5 mark
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive 5-mark answer on Antiarrhythmic Drugs Pharmacology:
Antiarrhythmic Drugs — Pharmacology
Definition & Mechanism of Arrhythmias
Arrhythmias arise from two fundamental mechanisms:
- Abnormal automaticity — ectopic pacemaker cells depolarize spontaneously outside the SA node
- Re-entry — a unidirectional block creates a short-circuit pathway that re-excites cardiac muscle
Antiarrhythmic drugs suppress arrhythmias by modulating ion channel flow or altering autonomic function.
Vaughan–Williams Classification
The Singh–Vaughan–Williams classification groups drugs by their predominant effect on the cardiac action potential across four classes.
Class I — Sodium Channel Blockers
Block fast Na⁺ channels → slow Phase 0 depolarization → reduce conduction velocity
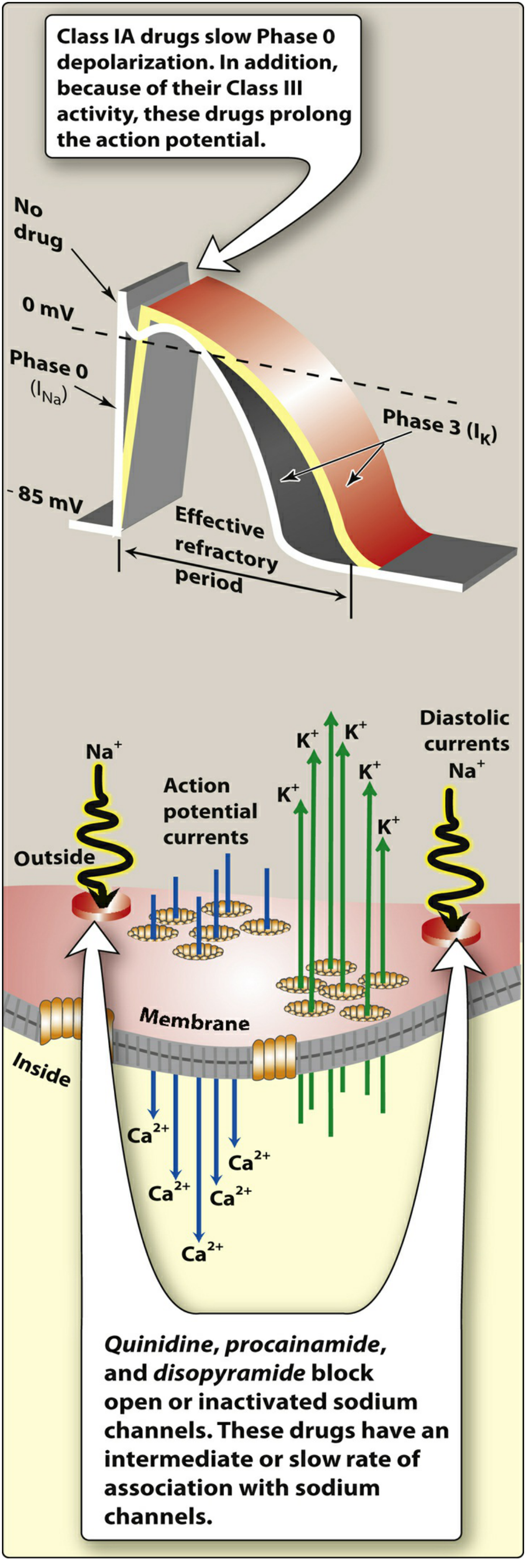
Class IA — Quinidine, Procainamide, Disopyramide
- Block open and inactivated Na⁺ channels (intermediate dissociation)
- Also block K⁺ channels → prolonged Phase 3 repolarization → ↑ effective refractory period (ERP) → QT prolongation
- Quinidine: additional α-blocking + anticholinergic actions; causes cinchonism (tinnitus, blurred vision, headache)
- Procainamide: IV only; causes lupus-like syndrome, hypotension; metabolized to NAPA (active Class III metabolite)
- Disopyramide: strongest anticholinergic (dry mouth, urinary retention); negative inotrope
Uses: Atrial + ventricular tachyarrhythmias, AF rhythm control
Class IB — Lidocaine, Mexiletine
- Preferentially bind inactivated Na⁺ channels (fast dissociation)
- Shorten Phase 3 repolarization → shorter action potential duration
- Most effective in ischemic tissue (depolarized cells accumulate drug)
- Lidocaine: IV only; CNS toxicity (tremor, seizures, confusion)
- Mexiletine: oral analog of lidocaine
Uses: Ventricular arrhythmias (VT, VF), especially post-MI
Class IC — Flecainide, Propafenone
- Markedly slow Phase 0 (slow dissociation); pronounced effect at normal heart rates
- Minimal effect on repolarization
- CAST trial warning: Increased mortality in post-MI patients with structural heart disease
Uses: AF/flutter without structural heart disease ("pill-in-the-pocket" for AF)
Class II — β-Adrenergic Blockers
Drugs: Atenolol, Metoprolol, Esmolol (IV, ultra-short)
- Block β₁ receptors → inhibit Phase 4 spontaneous depolarization in SA and AV nodes
- ↓ heart rate, ↓ AV conduction velocity, ↑ PR interval
- Uses: Rate control in AF/flutter, SVT, post-MI arrhythmias
- Adverse effects: Bradycardia, heart block, bronchospasm, worsening HF
Class III — Potassium Channel Blockers
Block K⁺ channels → prolong Phase 3 repolarization → ↑ action potential duration → ↑ ERP → QT prolongation
| Drug | Key Features |
|---|---|
| Amiodarone | Class I+II+III+IV actions; longest half-life (~40–55 days); pulmonary fibrosis, thyroid toxicity, hepatotoxicity, corneal deposits, photosensitivity; drug of choice for VT/VF |
| Sotalol | Also has Class II (β-blocking) activity; risk of torsades de pointes |
| Dofetilide | Pure K⁺ blocker; AF/flutter; QT monitoring mandatory |
| Ibutilide | IV; acute cardioversion of AF/flutter |
Uses: Ventricular arrhythmias, AF rate/rhythm control
Class IV — Calcium Channel Blockers
Drugs: Verapamil, Diltiazem (non-dihydropyridines)
- Block L-type Ca²⁺ channels → slowed Phase 0 and Phase 4 in SA/AV nodes (Ca²⁺-dependent tissue)
- ↓ AV conduction → prolongs PR interval
- Uses: SVT termination, rate control in AF/flutter
- Adverse effects: Bradycardia, AV block, hypotension, negative inotropy
Miscellaneous (Unclassified) Antiarrhythmics
| Drug | Mechanism | Key Use |
|---|---|---|
| Adenosine | Activates K⁺ channels → hyperpolarizes AV node; t½ ~10–15 sec | Drug of choice for acute SVT |
| Digoxin | Inhibits Na⁺/K⁺-ATPase → ↑ vagal tone → slows AV conduction | Rate control in AF (overcome by sympathetics) |
| Magnesium sulfate | Slows SA node + AV conduction; membrane stabilizer | Drug of choice for torsades de pointes + digoxin toxicity |
Key Proarrhythmic Risks (Important!)
- All antiarrhythmics can be proarrhythmic — they can cause the very arrhythmias they treat
- QT prolongation → torsades de pointes (TdP): Class IA, IC, III drugs; also macrolide antibiotics + antipsychotics
- CAST trial: Class IC drugs ↑ mortality post-MI → avoid in structural heart disease
- Risk ↑ with hypokalemia, hypomagnesemia, or drug combinations inhibiting metabolism
Sources: Lippincott Illustrated Reviews: Pharmacology; Goodman & Gilman's Pharmacological Basis of Therapeutics; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.