Hot to check ecg report
Reading File
Finding Sources
Searching the Web
how to read ECG report step by step interpretation
Finding Sources
Searching Images
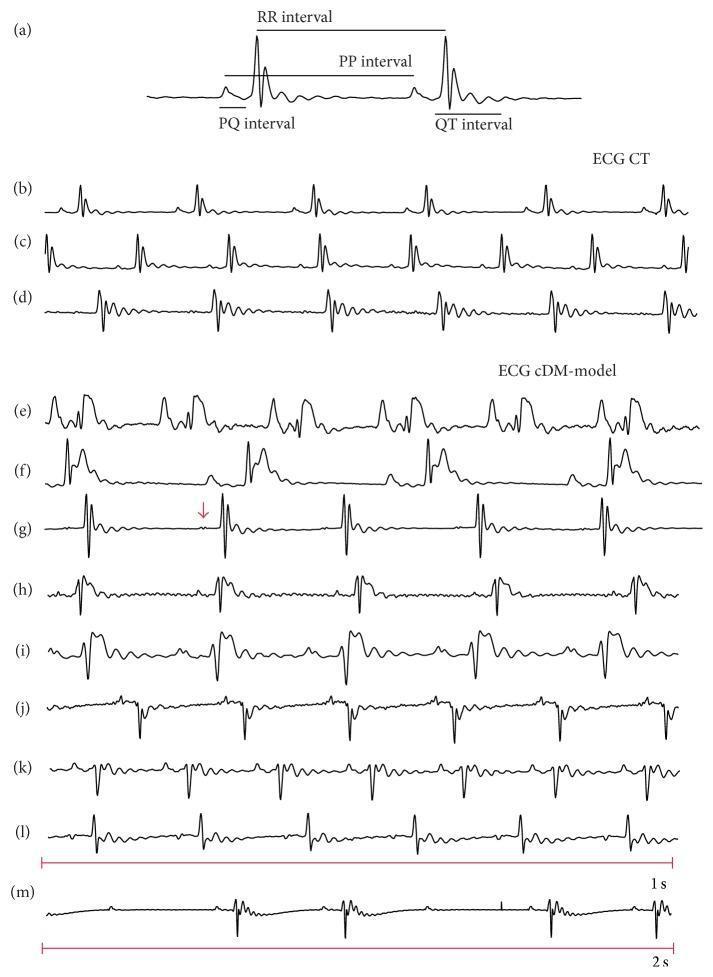
ECG interpretation diagram waves intervals
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here is a comprehensive, step-by-step guide to reading an ECG report:
How to Read an ECG Report
The ECG Grid
Each small square = 0.04 sec (horizontal) and 0.1 mV (vertical)
Each large square = 0.20 sec (5 small squares)
Step 1 — Check Heart Rate
Fastest method (regular rhythms):
300 ÷ number of large squares between two R peaks
| Large squares between R-R | Heart rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
For irregular rhythms: Count QRS complexes in a 10-second rhythm strip × 6.
- Normal: 60–100 bpm
- Bradycardia: < 60 bpm
- Tachycardia: > 100 bpm
Step 2 — Assess Rhythm
Ask: Is there a P wave before every QRS? Is the R-R interval regular?
| Finding | Likely Rhythm |
|---|---|
| Regular, P before every QRS | Normal Sinus Rhythm |
| Irregular, no P waves | Atrial Fibrillation |
| Regularly irregular | 2nd degree AV block / Wenckebach |
| Absent/buried P waves | Junctional or Ventricular rhythm |
Step 3 — Determine Electrical Axis
Look at Lead I and aVF:
| Lead I | aVF | Axis |
|---|---|---|
| ↑ Positive | ↑ Positive | Normal (−30° to +90°) |
| ↑ Positive | ↓ Negative | Left Axis Deviation (LAD) |
| ↓ Negative | ↑ Positive | Right Axis Deviation (RAD) |
| ↓ Negative | ↓ Negative | Extreme / Northwest axis |
Step 4 — Measure Intervals
| Interval | Normal Range | Abnormal Meaning |
|---|---|---|
| PR interval | 0.12–0.20 sec (3–5 small squares) | Prolonged → AV block; Short → pre-excitation (WPW) |
| QRS duration | < 0.12 sec (< 3 small squares) | Wide → Bundle branch block or ventricular beat |
| QT/QTc | < 0.44 sec (men), < 0.46 sec (women) | Prolonged → risk of Torsades de Pointes |
Step 5 — Examine Individual Waves
P Wave (Atrial Depolarization)
- Normal: < 0.12 sec wide, < 2.5 mm tall, upright in Lead II
- Tall peaked P in II → Right atrial enlargement
- Broad notched P in II → Left atrial enlargement
QRS Complex (Ventricular Depolarization)
- Normal: narrow (< 0.12 sec), Q waves < 1 mm wide and < 25% of R-wave height
- Wide QRS → Bundle branch block (LBBB/RBBB) or ventricular origin
- Pathological Q waves → Prior myocardial infarction
T Wave (Ventricular Repolarization)
- Normal: same direction as QRS
- Inverted T → Ischemia, strain, or infarction
- Peaked tall T → Hyperkalemia or early STEMI (hyperacute T)
Step 6 — Analyze ST Segment
This is the most critical step for detecting heart attack:
| Finding | Significance |
|---|---|
| ST elevation ≥ 1 mm in ≥ 2 contiguous leads | STEMI (acute MI) — emergency! |
| ST depression | Ischemia, NSTEMI, or digoxin effect |
| Flat/isoelectric ST | Normal |
Localizing the Infarct by Leads:
| Leads with changes | Territory |
|---|---|
| II, III, aVF | Inferior (RCA) |
| I, aVL, V5, V6 | Lateral (LCx) |
| V1–V4 | Anterior (LAD) |
| V1–V2 | Septal |
Step 7 — Look for Special Patterns
| Pattern | ECG Finding |
|---|---|
| Right Bundle Branch Block (RBBB) | "M" shape (rSR') in V1; wide S in V6 — mnemonic: MaRRoW |
| Left Bundle Branch Block (LBBB) | Broad notched R in V5/V6; QS in V1 — mnemonic: WiLLiaM |
| WPW (pre-excitation) | Short PR + delta wave |
| Atrial flutter | Sawtooth P waves, ~300 bpm atrial rate |
| 1st degree AV block | PR > 0.20 sec |
| 2nd degree Mobitz I (Wenckebach) | Progressively longer PR until a QRS drops |
| 2nd degree Mobitz II | Constant PR, then sudden dropped QRS |
| 3rd degree (complete) AV block | P waves and QRS are completely dissociated |
| Hyperkalemia | Peaked T → wide QRS → sine wave pattern |
| Hypokalemia | Flat T, prominent U wave |
Quick Systematic Checklist
- ✅ Rate (bradycardia / normal / tachycardia)
- ✅ Rhythm (regular? P before every QRS?)
- ✅ Axis (Lead I + aVF)
- ✅ Intervals (PR, QRS, QT)
- ✅ P wave morphology
- ✅ QRS morphology (Q waves, bundle branch block)
- ✅ ST segment (elevation or depression?)
- ✅ T wave changes
- ✅ Compare with previous ECG if available
Sources: Braunwald's Heart Disease, 12e; Miller's Anesthesia, 10e; UNC School of Medicine EKG Interpretation
This is a shared conversation. Sign in to Orris to start your own chat.