Anantomy of Bronchopulmonary Segments
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a detailed account of the anatomy of bronchopulmonary segments, drawn from Gray's Anatomy for Students, Fischer's Mastery of Surgery, and the Color Atlas of Human Anatomy.
Anatomy of Bronchopulmonary Segments
Definition
A bronchopulmonary segment is the area of lung supplied by a single segmental (tertiary) bronchus and its accompanying branch of the pulmonary artery. It is the smallest functionally independent region of the lung - the smallest unit that can be surgically isolated and removed without affecting adjacent regions.
- Gray's Anatomy for Students, p. 208-210
Structural Features
Each segment has a distinct 3D shape:
- Shape: Irregular cone / pyramidal wedge
- Apex: Points toward the hilum (origin of the segmental bronchus)
- Base: Projected peripherally onto the lung surface
Internal composition (the "bronchoarterial unit"):
| Structure | Location within segment |
|---|---|
| Segmental bronchus | Centrally located (intrasegmental) |
| Pulmonary artery branch | Central, travels alongside bronchus |
| Pulmonary vein tributaries | Intersegmental - run along segment margins/boundaries |
| Bronchial arteries | Follow the bronchial tree |
The pulmonary vein tributaries deliberately traveling between segments is what defines segment boundaries and makes surgical isolation possible.
- Color Atlas of Human Anatomy Vol 2, p. 214
Bronchial Tree Hierarchy
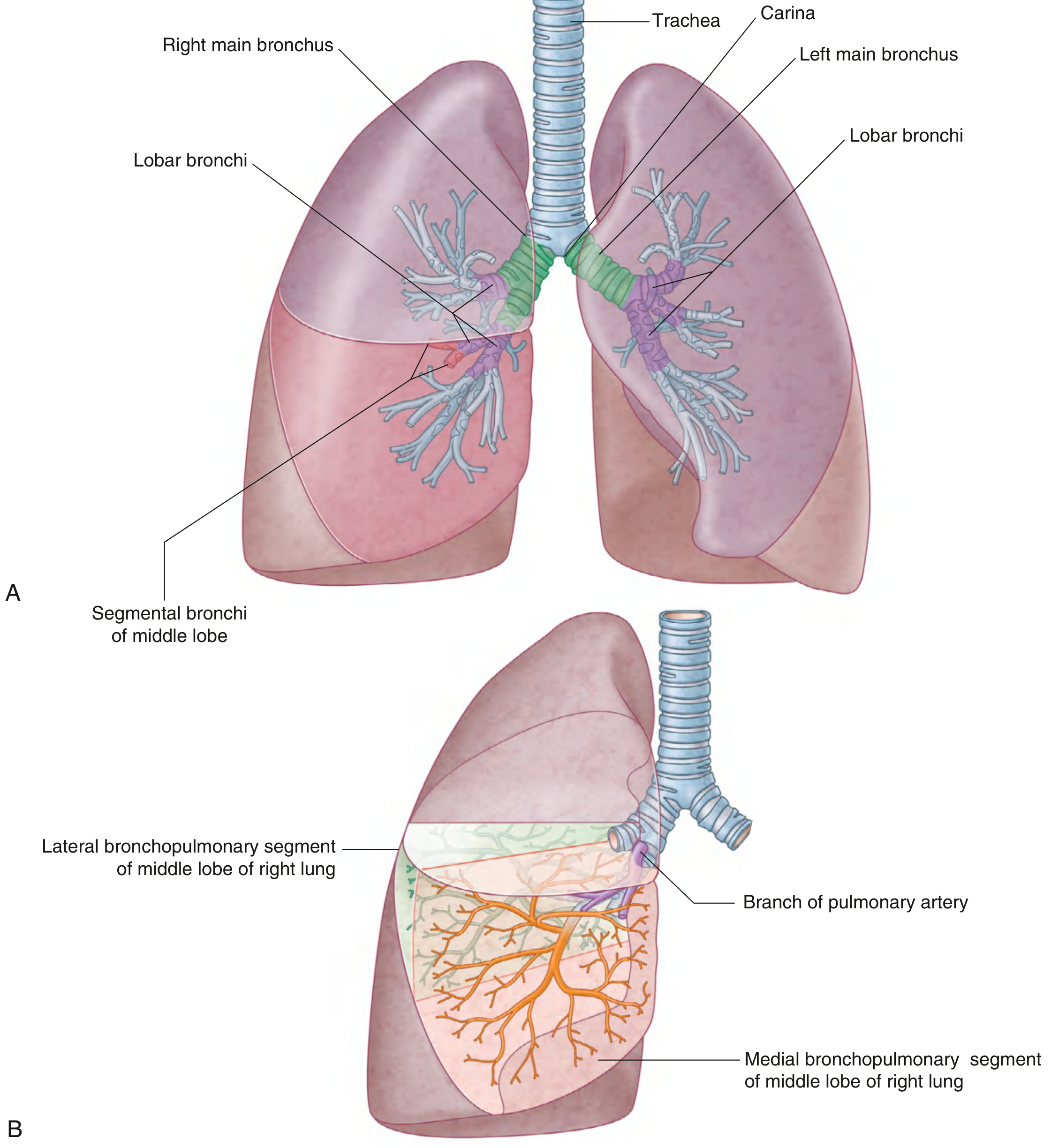
Fig. 3.48 (A) Bronchial tree. (B) Bronchopulmonary segments - Gray's Anatomy for Students
Hierarchy: Trachea → Main bronchi → Lobar bronchi → Segmental bronchi → Bronchioles → Terminal bronchioles → Respiratory bronchioles → Alveolar ducts → Alveoli
Within each segment, the segmental bronchi subdivide through multiple generations, ultimately reaching bronchioles. Bronchi have cartilaginous wall support; bronchioles do not.
Segments of the Right Lung (10 total)
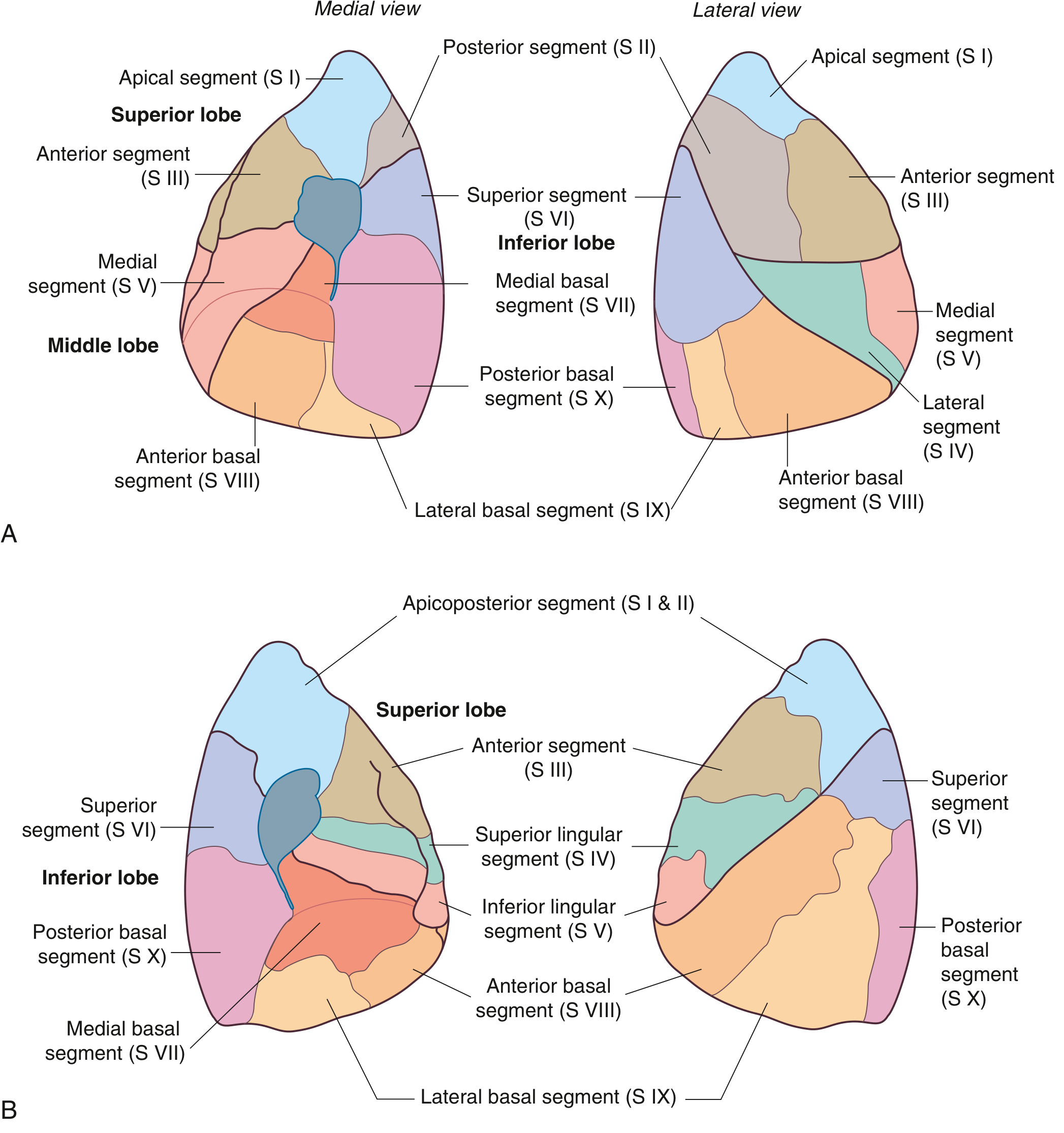
Fig. 3.49 Bronchopulmonary segments of right lung (A) and left lung (B) - Gray's Anatomy for Students
Right Superior (Upper) Lobe - 3 segments
| # | Segment | Bronchus (endoscopic clock position) |
|---|---|---|
| S I | Apical | B1 - orifice at 4 o'clock |
| S II | Posterior | B2 - orifice at 12 o'clock |
| S III | Anterior | B3 - orifice at 8 o'clock |
Right Middle Lobe - 2 segments
| # | Segment | Bronchus |
|---|---|---|
| S IV | Lateral | B4 - orifice at 3-6 o'clock |
| S V | Medial | B5 - orifice at 9-12 o'clock |
Right Inferior (Lower) Lobe - 5 segments
| # | Segment | Bronchus |
|---|---|---|
| S VI | Superior | B6 - at 5 o'clock, just past middle lobe bronchus |
| S VII | Medial basal | B7 - at 9 o'clock (usually most proximal basal) |
| S VIII | Anterior basal | B8 - at 1 o'clock |
| S IX | Lateral basal | B9 - at 3 o'clock |
| S X | Posterior basal | B10 - at 6 o'clock |
Note: In more than half of patients, a subapical (subsuperior) segment is present in the lower lobe, with a posteriorly directed bronchus arising anywhere from the superior segment to the final lobar division.
- Fischer's Mastery of Surgery, p. 2058
Segments of the Left Lung (8-10 depending on convention)
The left lung has 8 segments in American/international convention and 10 in British convention. The difference stems from fusion of segments:
- Apical (S I) + Posterior (S II) → Apicoposterior segment (S I + II)
- Medial basal (S VII) + Anterior basal (S VIII) → Anteromedial basal (S VII + VIII)
Left Superior (Upper) Lobe - 4 segments
Upper division (orifice at 8 o'clock):
| # | Segment | Notes |
|---|---|---|
| S I+II | Apicoposterior | Fusion of apical + posterior (B1+3 in some systems) |
| S III | Anterior | B2 |
Lingular division (orifice at 2 o'clock) - equivalent to the right middle lobe:
| # | Segment | Bronchus |
|---|---|---|
| S IV | Superior lingular | B4 - orifice at 10 o'clock |
| S V | Inferior lingular | B5 - orifice at 2 o'clock |
Left Inferior (Lower) Lobe - 4 segments
| # | Segment | Bronchus |
|---|---|---|
| S VI | Superior | B6 - at 6 o'clock, just past origin of lower lobe |
| S VII+VIII | Anteromedial basal | B8+7 - orifice at 12 o'clock |
| S IX | Lateral basal | B9 - at 9 o'clock |
| S X | Posterior basal | B10 - at 5 o'clock |
Detailed Segmental Diagram (Anterior & Medial Views)
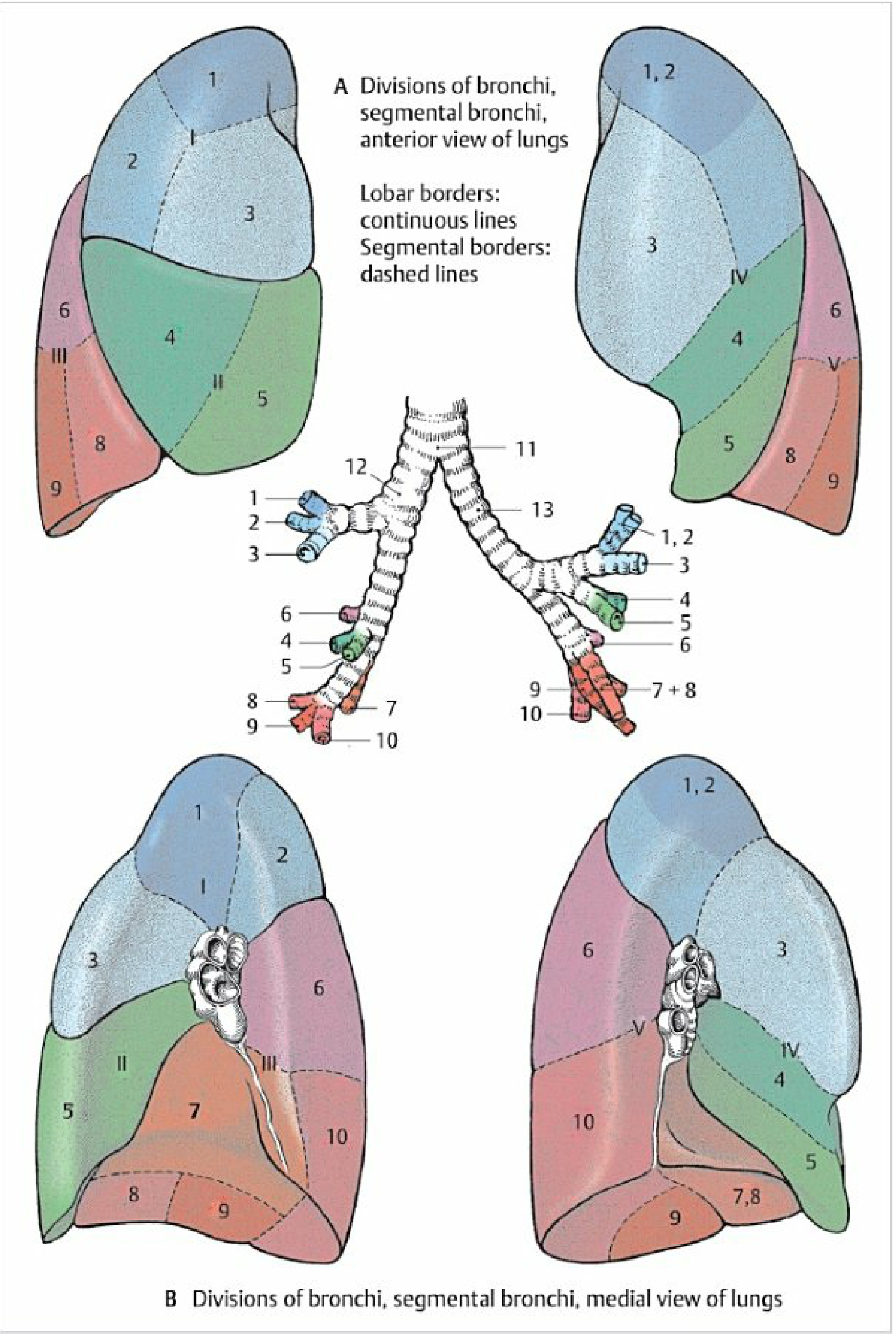
Fig. 3.16 Bronchial divisions and bronchopulmonary segments - Color Atlas of Human Anatomy Vol 2, p. 215-216
In this diagram:
- Blue = Superior lobe
- Green = Middle lobe (right) / Lingula (left)
- Red/orange = Inferior lobe
- Continuous lines = lobar borders
- Dashed lines = segmental borders
Quick Reference Summary Table
| Lung | Lobe | Segments |
|---|---|---|
| Right | Superior | Apical (I), Posterior (II), Anterior (III) |
| Right | Middle | Lateral (IV), Medial (V) |
| Right | Inferior | Superior (VI), Medial basal (VII), Anterior basal (VIII), Lateral basal (IX), Posterior basal (X) |
| Left | Superior | Apicoposterior (I+II), Anterior (III), Superior lingular (IV), Inferior lingular (V) |
| Left | Inferior | Superior (VI), Anteromedial basal (VII+VIII), Lateral basal (IX), Posterior basal (X) |
Clinical Relevance
- Surgery (segmentectomy): Because segments are separated by intersegmental veins with minimal cross-communication, individual segments can be resected (e.g., for small lung cancers or bronchiectasis) - Fischer's Mastery of Surgery, p. 2058
- Bronchoscopy: The clock-face positions of bronchial orifices help bronchoscopists navigate to specific segments for biopsy, BAL, or foreign body removal
- Postural drainage: Each segment drains best with a specific body position, used in physiotherapy for bronchiectasis and COPD
- Aspiration pneumonia: Due to gravity, aspirated material most often settles in the superior segment of the right lower lobe (S VI) and the posterior segment of the right upper lobe (S II) when supine
- Radiology: Lobar/segmental collapse patterns on CXR or CT follow these anatomical boundaries
Anatomy of Pleura
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Here is a comprehensive account of pleural anatomy, drawn from Gray's Anatomy for Students, Color Atlas of Human Anatomy, and Fischer's Mastery of Surgery.
Anatomy of the Pleura
Definition and Basic Structure
The pleura is a serous membrane that lines the thoracic cavity and covers the lungs. Each pleural cavity is lined by a single layer of flat cells - mesothelium - and an associated layer of supporting connective tissue; together these form the pleura.
There are two major types:
| Type | Location | Characteristics |
|---|---|---|
| Parietal pleura | Lines the walls of the pleural cavity | Thicker; somatic innervation; pain-sensitive |
| Visceral pleura | Covers the lung surface | Thinner; visceral innervation; not directly pain-sensitive |
The pleural cavity is the potential space enclosed between the two layers. It normally contains only a thin film of serous fluid (a few mL), which reduces friction and allows the lung surface to glide freely over the thoracic wall during breathing.
- Gray's Anatomy for Students, p. 201
Diagram: Pleural Cavities and Parts of Parietal Pleura
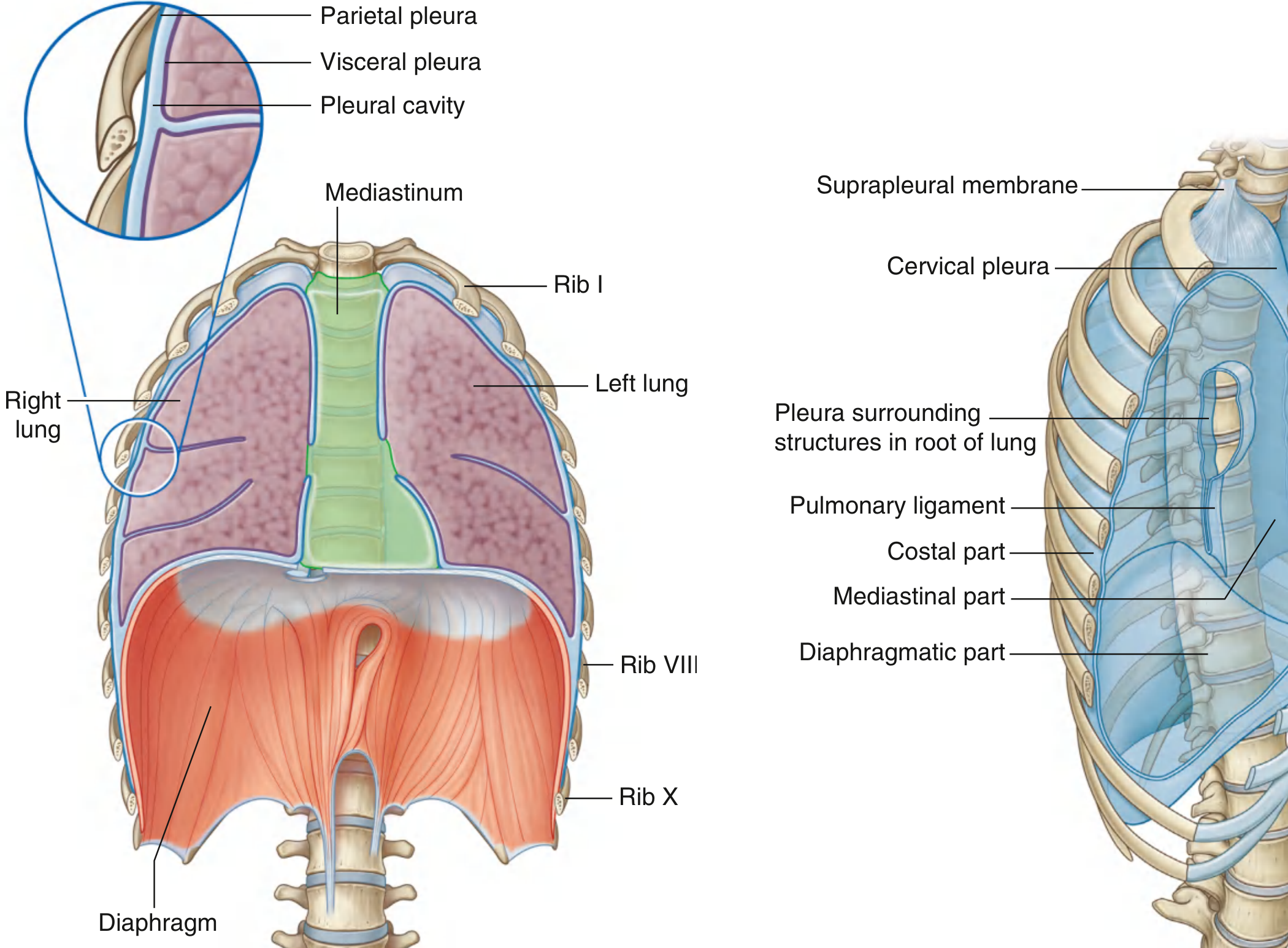
Fig. 3.38 & 3.39 - Pleural cavities and parietal pleura. Gray's Anatomy for Students
Parietal Pleura - Parts
The parietal pleura is named according to the wall it covers. There are four named parts:
1. Costal Part
- Lines the inner surface of the ribs and intercostal spaces
- Separated from the thoracic wall by endothoracic fascia (a layer of connective tissue between the pleura and the internal thoracic wall)
- Innervated by intercostal nerves → pain felt in the thoracic wall
2. Diaphragmatic Part
- Covers the upper (thoracic) surface of the diaphragm
- Innervated by the phrenic nerve (C3, C4, C5) → pain referred to the lateral neck and shoulder (C3-C5 dermatomes)
3. Mediastinal Part
- Covers the lateral surface of the mediastinum
- Also innervated by the phrenic nerve → same referred pain pattern (neck/shoulder)
- In the region of TV-TVII, the mediastinal pleura reflects off as a tubular sleeve around the structures of the root of the lung (bronchi, vessels, nerves, lymphatics)
- This sleeve-like covering becomes continuous with the visceral pleura at the hilum
4. Cervical Pleura (Pleural Cupola / Dome of Pleura)
-
The dome-shaped apex of the pleural cavity projecting into the root of the neck, above the first rib
-
Filled by the apex of the lung
-
Covered superiorly by the suprapleural membrane (Sibson's fascia) - a thickened layer of endothoracic fascia attached to the medial margin of rib I and the transverse process of C7
-
The scalene muscles attach to this membrane and keep it taut
-
The cervical pleura is at risk during procedures at the root of the neck (e.g., subclavian line, brachial plexus block, first rib resection)
-
Color Atlas of Human Anatomy Vol 2, p. 214; Gray's Anatomy for Students, p. 201
Visceral Pleura
- Covers the lung almost entirely, including the surfaces within the interlobar fissures
- Cannot be stripped from the lung surface - it is firmly adherent
- Does not cover the hilum or the area between the lung and pulmonary ligament
- Continuous with the parietal pleura at the hilum
- Innervated by visceral afferent fibers accompanying bronchial vessels - pain is generally not elicited from visceral pleura directly
Pulmonary Ligament
Below the root of the lung, the mediastinal pleura forms a double-layered fold called the pulmonary ligament, which hangs downward from the hilum like a curtain. It anchors the lower lobe of the lung to the mediastinum and allows the lung to expand/move without excess displacement.
Pleural Recesses
The lungs do not completely fill the pleural cavities, so there are potential spaces called pleural recesses where the lung expands during deep inspiration.
1. Costodiaphragmatic Recess (most important clinically)
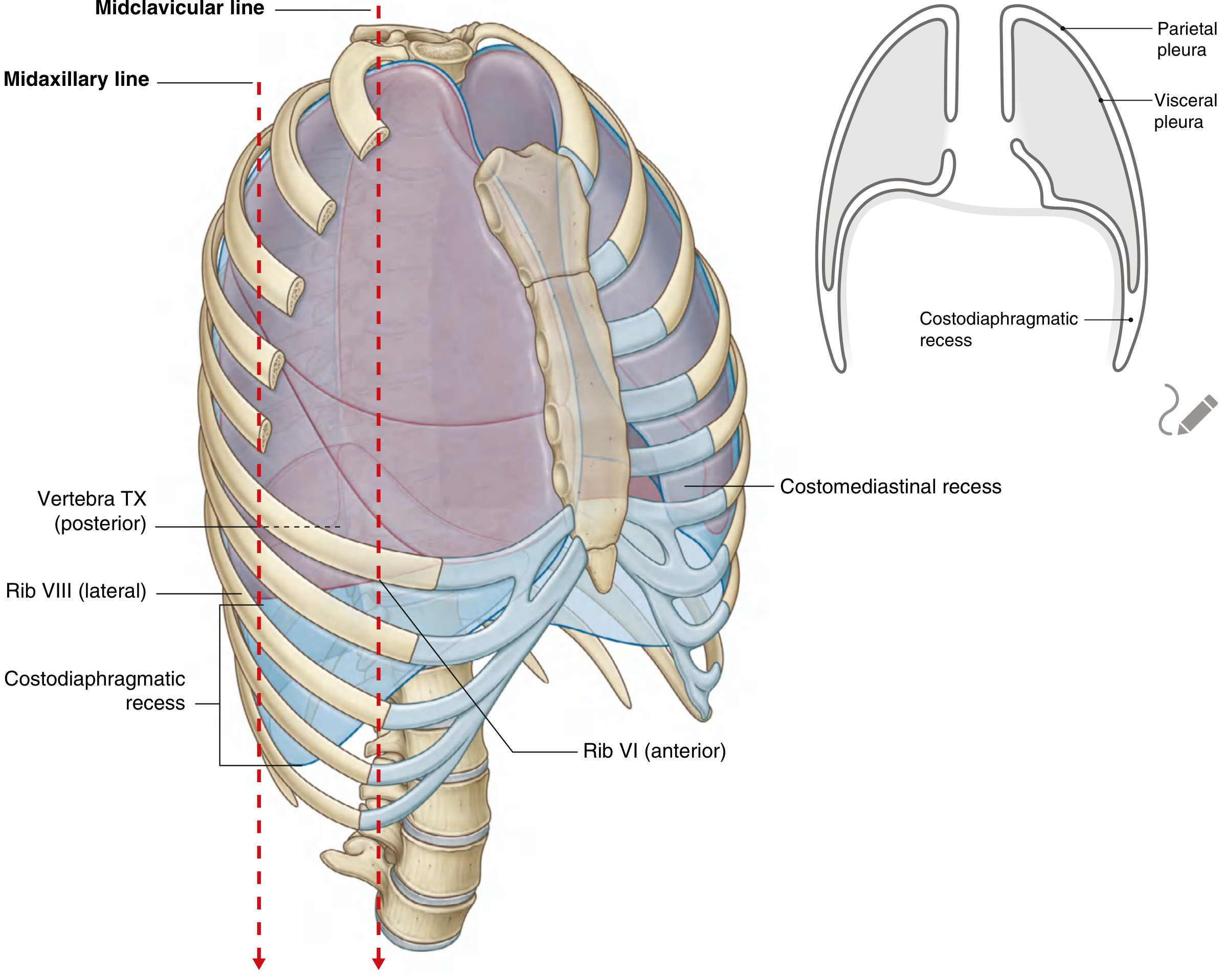
Fig. 3.41 - Pleural recesses and lung/pleural margins. Gray's Anatomy for Students
- Located between costal pleura and diaphragmatic pleura
- Deepest recess; deepest during forced expiration (when lung margins rise up)
- The region between the inferior lung margin and inferior pleural margin
2. Costomediastinal Recess
- Located anteriorly where costal pleura meets mediastinal pleura
- Largest on the left side, overlying the cardiac notch of the left lung
- On the right it is narrow
Pleural Reflections - Surface Landmarks
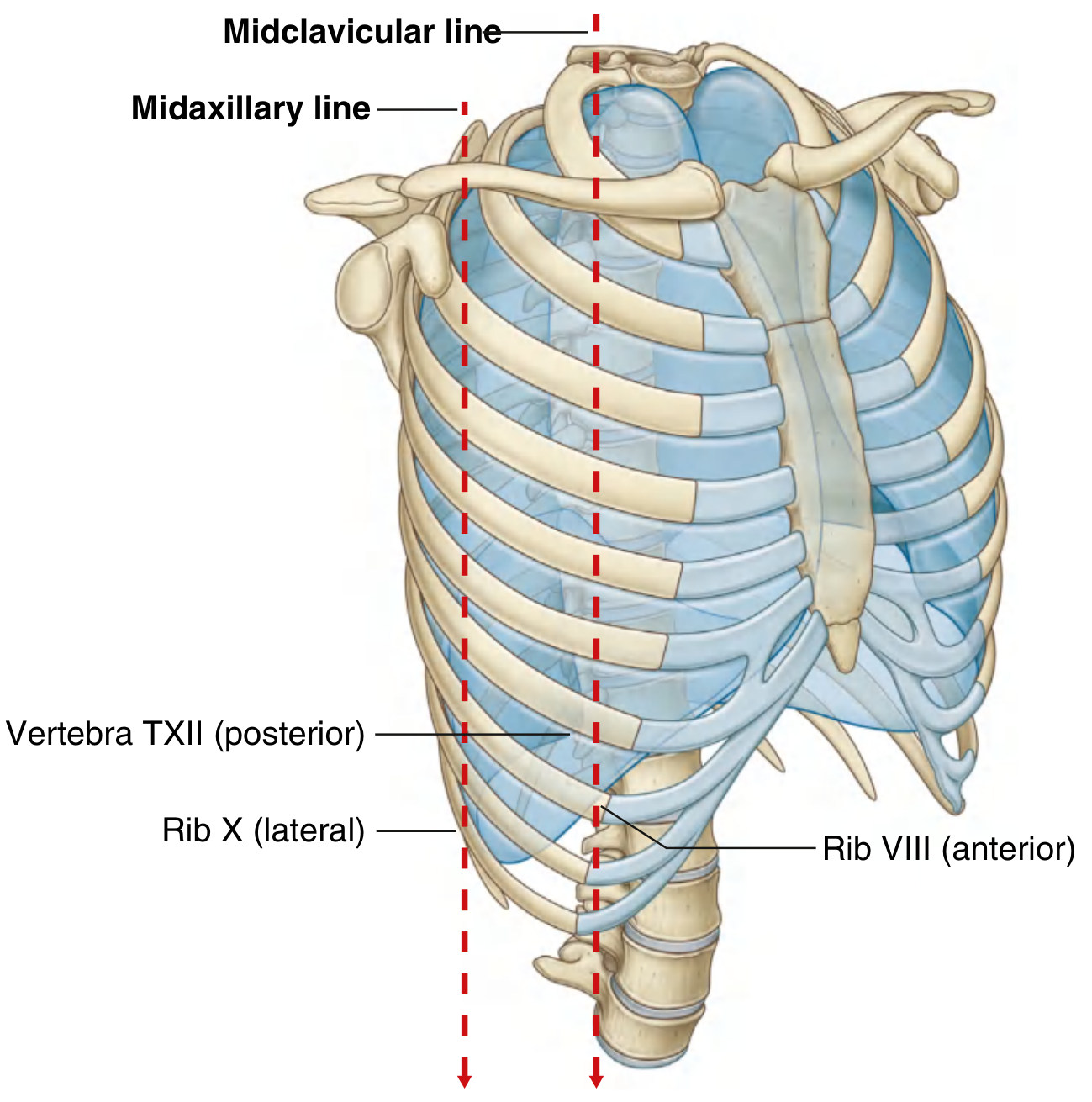
Fig. 3.40 - Inferior pleural reflections. Gray's Anatomy for Students
Superior extent
- The pleural cavity projects 3-4 cm above the first costal cartilage into the neck
- Does not extend above the neck of rib I
Anterior extent
- Both pleural cavities approach each other posterior to the upper sternum
- On the left, the cavity does not reach the midline as closely as on the right (because the pericardium and heart bulge to the left)
Inferior extent (key landmarks)
| Vertical Line | Inferior Lung Margin | Inferior Pleural Margin |
|---|---|---|
| Midclavicular line | Rib VI | Rib VIII |
| Midaxillary line | Rib VIII | Rib X |
| Vertebral column (posterior) | Vertebra TX | Vertebra TXII |
So the inferior pleural boundary runs: Rib VIII → Rib X → T12
The costodiaphragmatic recess lies between the lung margin and the pleural margin in this zone.
Topography: Lung and Pleural Borders in Context
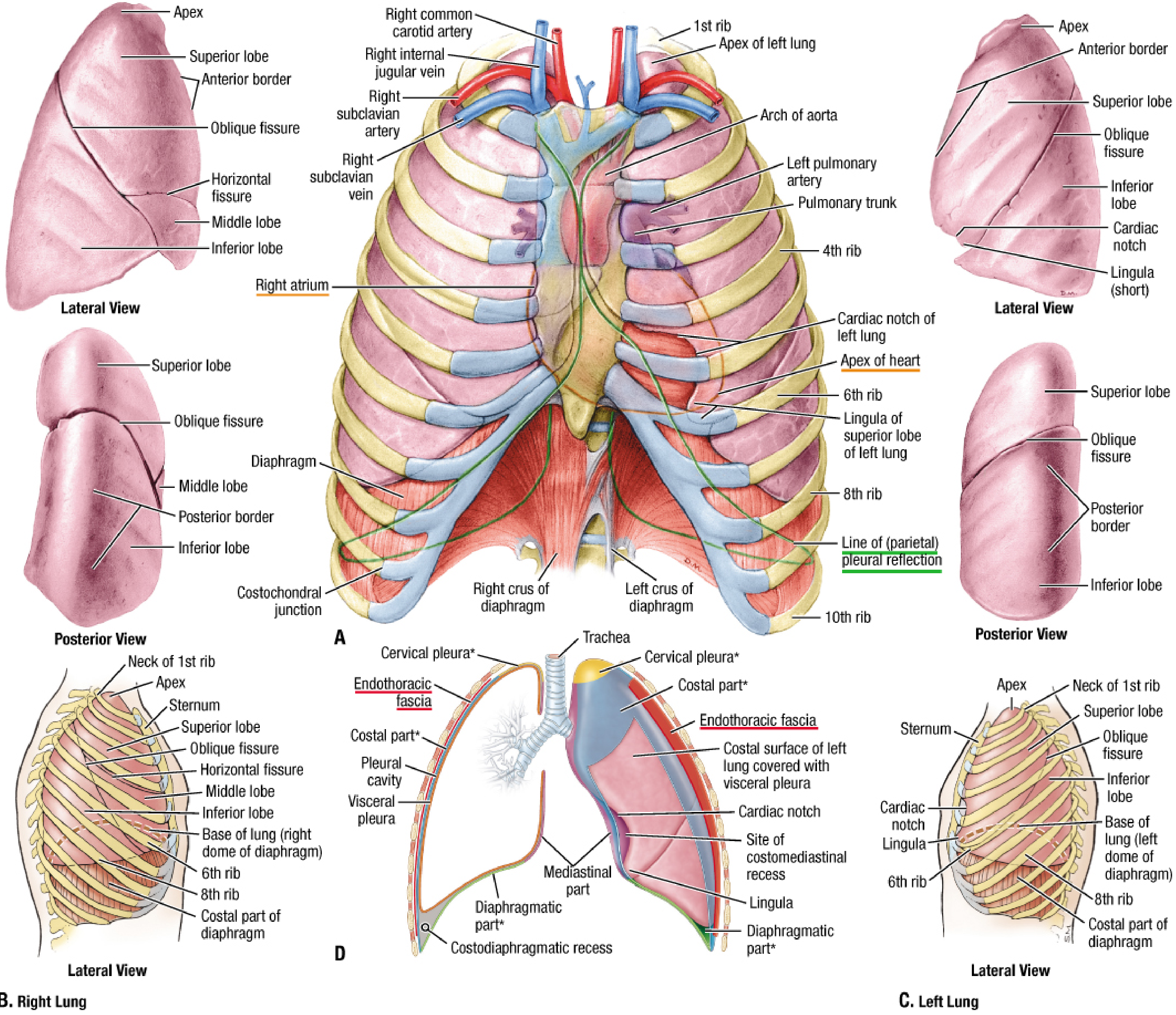
Fig. 84.1D - Pleura topography. Fischer's Mastery of Surgery, p. 2211
Neurovascular Supply and Lymphatics
Parietal Pleura
| Region | Arterial Supply | Innervation |
|---|---|---|
| Costal part | Posterior intercostal arteries, internal thoracic artery, musculophrenic artery | Intercostal nerves (somatic) |
| Diaphragmatic part | Musculophrenic and pericardiophrenic arteries | Phrenic nerve (C3-C5) |
| Mediastinal part | Pericardiophrenic artery | Phrenic nerve (C3-C5) |
| Cervical (cupola) | Superior intercostal / subclavian branches | Intercostal nerves |
Venous drainage: via veins of the thoracic wall
Visceral Pleura
- Arterial supply: bronchial arteries (part of the lung's intrinsic supply)
- Innervation: visceral afferents - not pain sensitive
Histology
The pleura is composed of:
- Mesothelium - a single layer of flat (squamous) cells forming the surface
- Connective tissue - providing structural support beneath the mesothelium
The visceral pleura forms an integral part of the lung parenchyma; the parietal pleura is a separate, slidable layer.
Clinical Correlates
| Condition | Mechanism | Relevance to Pleural Anatomy |
|---|---|---|
| Pleural effusion | Excess fluid in pleural cavity | Accumulates in costodiaphragmatic recess first; aspirated in midaxillary line above rib IX (below rib VIII margin) to avoid neurovascular bundle |
| Pneumothorax | Air enters pleural cavity | Lung collapses due to tissue elasticity once negative pressure lost |
| Pleurisy | Inflammation of parietal pleura | Costal pleura involvement = sharp chest wall pain; diaphragmatic/mediastinal = shoulder tip pain (phrenic nerve) |
| Thoracocentesis | Needle aspiration of pleural fluid | Needle inserted above the upper border of a rib to avoid the intercostal neurovascular bundle |
| Cervical pleura injury | During neck surgery, subclavian line | Can cause pneumothorax - suprapleural membrane is the protective barrier |
| Mesothelioma | Malignant tumor of mesothelium | Usually from asbestos exposure; arises from the pleural mesothelium |
- Gray's Anatomy for Students, p. 202-203; Color Atlas of Human Anatomy Vol 2, p. 224
Anatomy of Blood Supply of Heart
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Now I have all the content needed for a comprehensive answer. Here it is:
Anatomy of Blood Supply of the Heart
Overview
The heart has its own dedicated arterial supply through two coronary arteries - the right and left coronary arteries - which arise from the aortic sinuses of the ascending aorta, just above the aortic valve. These are the first branches of the aorta. Venous drainage returns primarily through the coronary sinus to the right atrium.
The coronary arteries lie in the subepicardial fat within the sulci of the heart; their branches often penetrate into the myocardium (myocardial bridges).
Arterial Supply - Overview Diagram
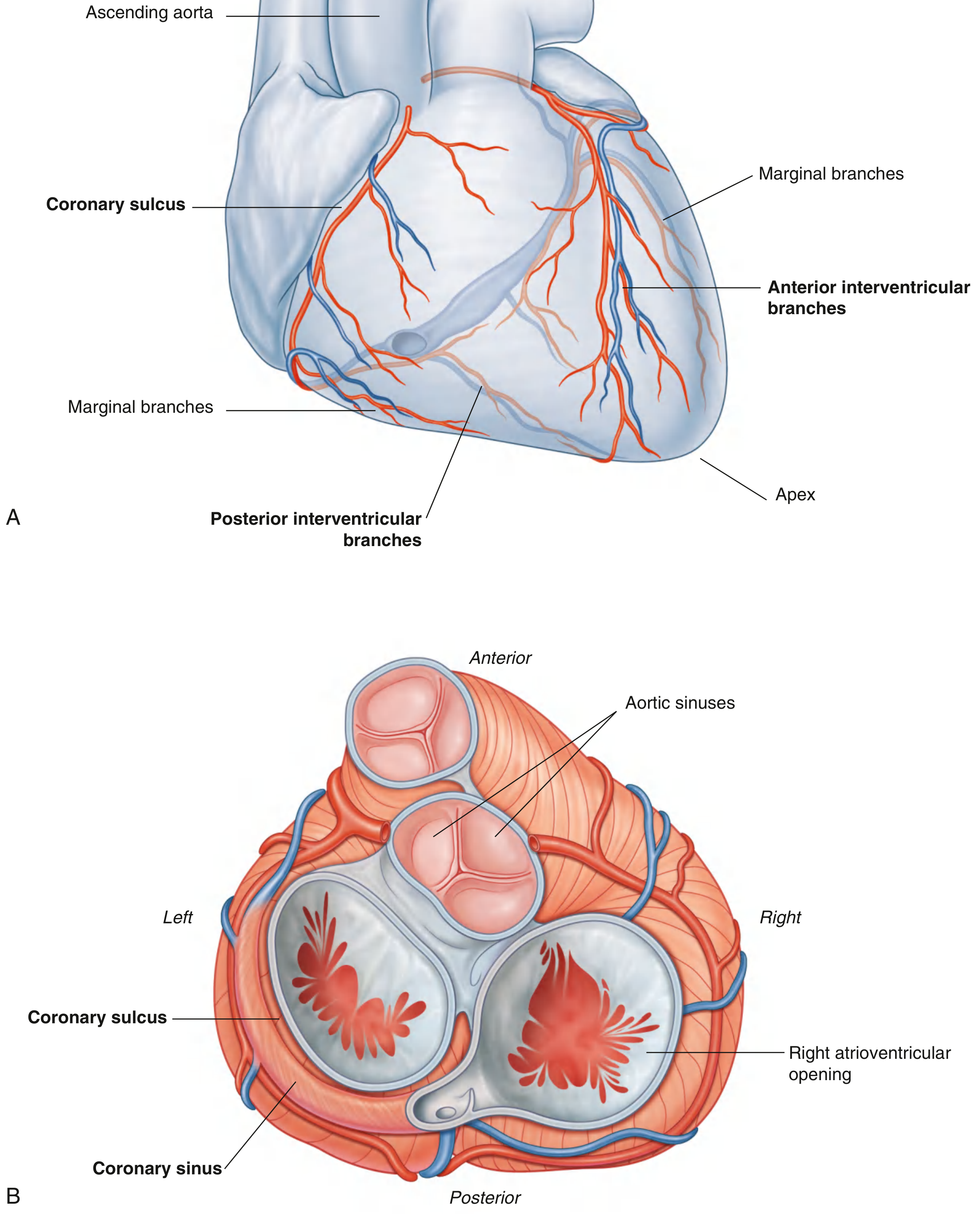
Fig. 3.79 Cardiac vasculature - anterior view (A) and superior view showing aortic sinuses and coronary sulcus (B). Gray's Anatomy for Students
Right Coronary Artery (RCA)
Origin: Right aortic sinus of the ascending aorta
Course: Passes anteriorly → descends vertically in the coronary sulcus (between right atrium and right ventricle) → reaches the inferior (acute) margin → turns posteriorly onto the diaphragmatic surface
Branches of the RCA
| Branch | Course & Supply |
|---|---|
| Sinoatrial (SA) nodal branch | Arises early; passes posteriorly around the superior vena cava to supply the SA node (in ~60% of people) |
| Right marginal branch | Runs along the inferior (acute) margin toward the apex |
| AV nodal branch | Small branch to the atrioventricular node before giving off the terminal branch |
| Posterior interventricular branch (= posterior descending artery, PDA) | Terminal branch; runs in the posterior interventricular sulcus |
Territory supplied by RCA
-
Right atrium and right ventricle
-
SA node and AV node (usually)
-
Interatrial septum
-
Posterior portion of left atrium
-
Posteroinferior 1/3 of the interventricular septum
-
Posterior part of the left ventricle
-
Gray's Anatomy for Students, p. 238
Left Coronary Artery (LCA)
Origin: Left aortic sinus of the ascending aorta
Course: The short stem (left main stem) passes between the pulmonary trunk and left auricle → enters the coronary sulcus → emerges from behind the pulmonary trunk → bifurcates into two terminal branches
Two Terminal Branches
1. Anterior Interventricular Branch (= Left Anterior Descending, LAD)
- Descends obliquely in the anterior interventricular sulcus toward the apex
- Wraps around the apex and usually anastomoses with the posterior interventricular branch of the RCA
- May give off 1-2 diagonal branches descending across the anterior left ventricle
- Supplies: both ventricles, anterior 2/3 of the interventricular septum, AV bundle and its branches
2. Circumflex Branch
- Courses left in the coronary sulcus onto the base/diaphragmatic surface
- Usually ends before reaching the posterior interventricular sulcus
- Gives off the left marginal artery (following the obtuse margin)
- In ~40% of people gives off the SA nodal branch
Territory supplied by LCA
- Most of the left atrium and left ventricle
- Most of the interventricular septum (anterior 2/3)
- AV bundle and its branches
Both Coronary Arteries - Labeled Diagram
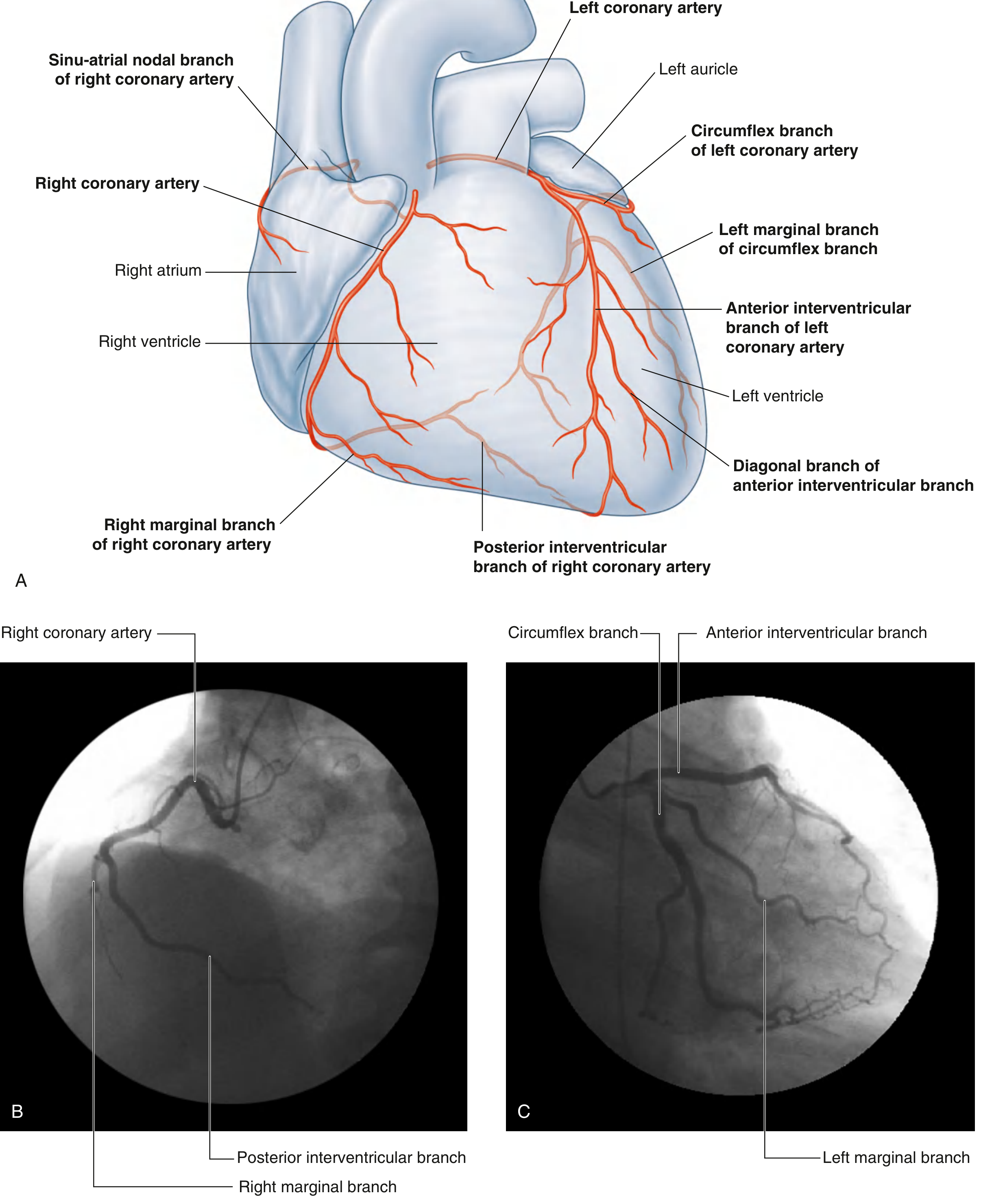
Fig. 3.80 - Coronary arteries with angiographic correlation. Gray's Anatomy for Students, p. 240-241
Coronary Dominance
"Dominance" refers to which artery gives rise to the posterior interventricular (descending) branch and therefore supplies the posterior left ventricular wall.
| Pattern | Frequency | Description |
|---|---|---|
| Right dominant | ~70% | PDA from RCA; RCA supplies large portion of posterior LV wall; circumflex is relatively small |
| Left dominant | ~15% | PDA from an enlarged circumflex branch; circumflex supplies most of posterior LV |
| Co-dominant / Balanced | ~15% | Both RCA and circumflex contribute to posterior supply |
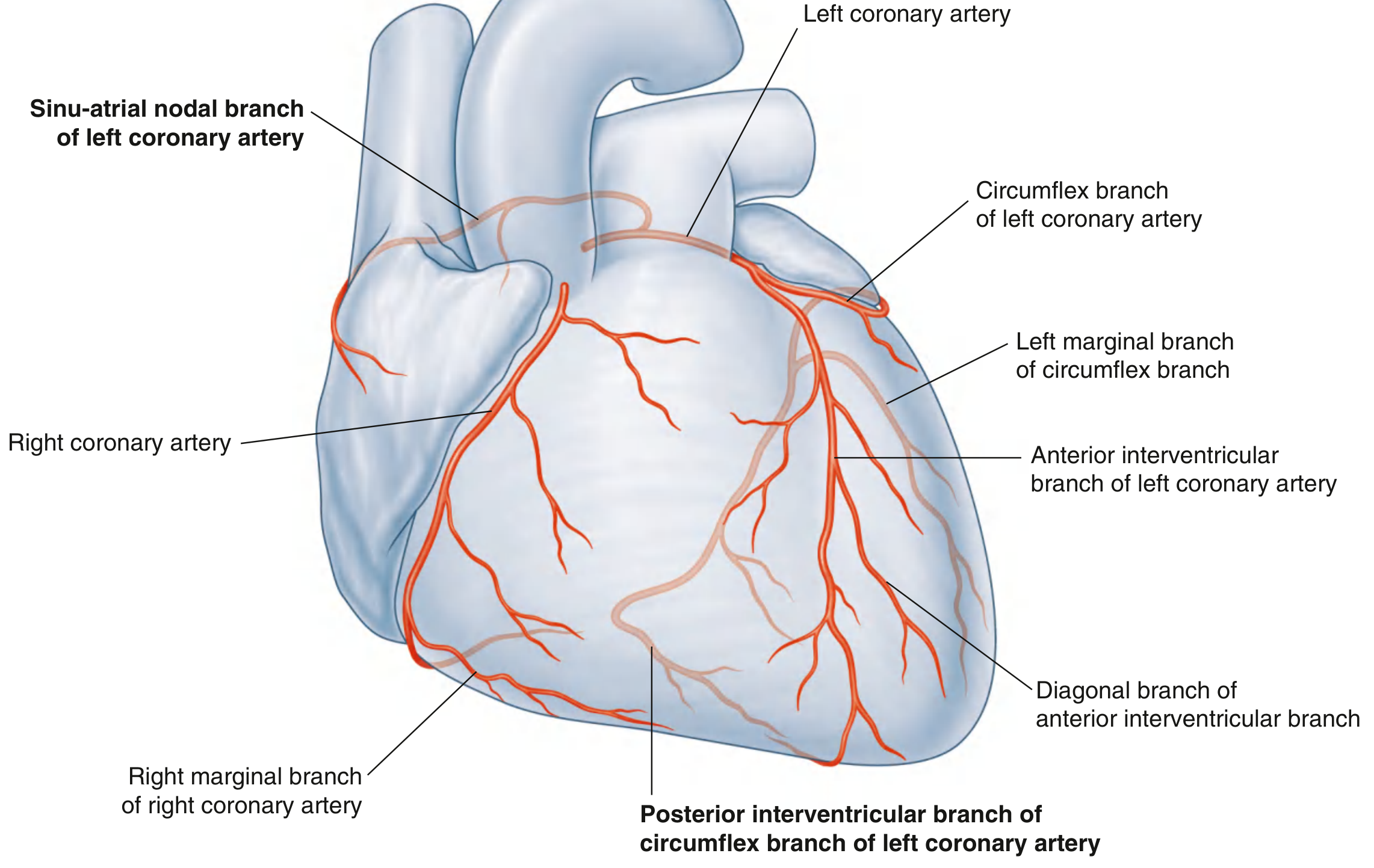
Fig. 3.81 - Left dominant coronary artery. Gray's Anatomy for Students, p. 241
- Color Atlas of Human Anatomy Vol 2, p. 58
Coronary Arteries on Sternocostal and Diaphragmatic Surfaces
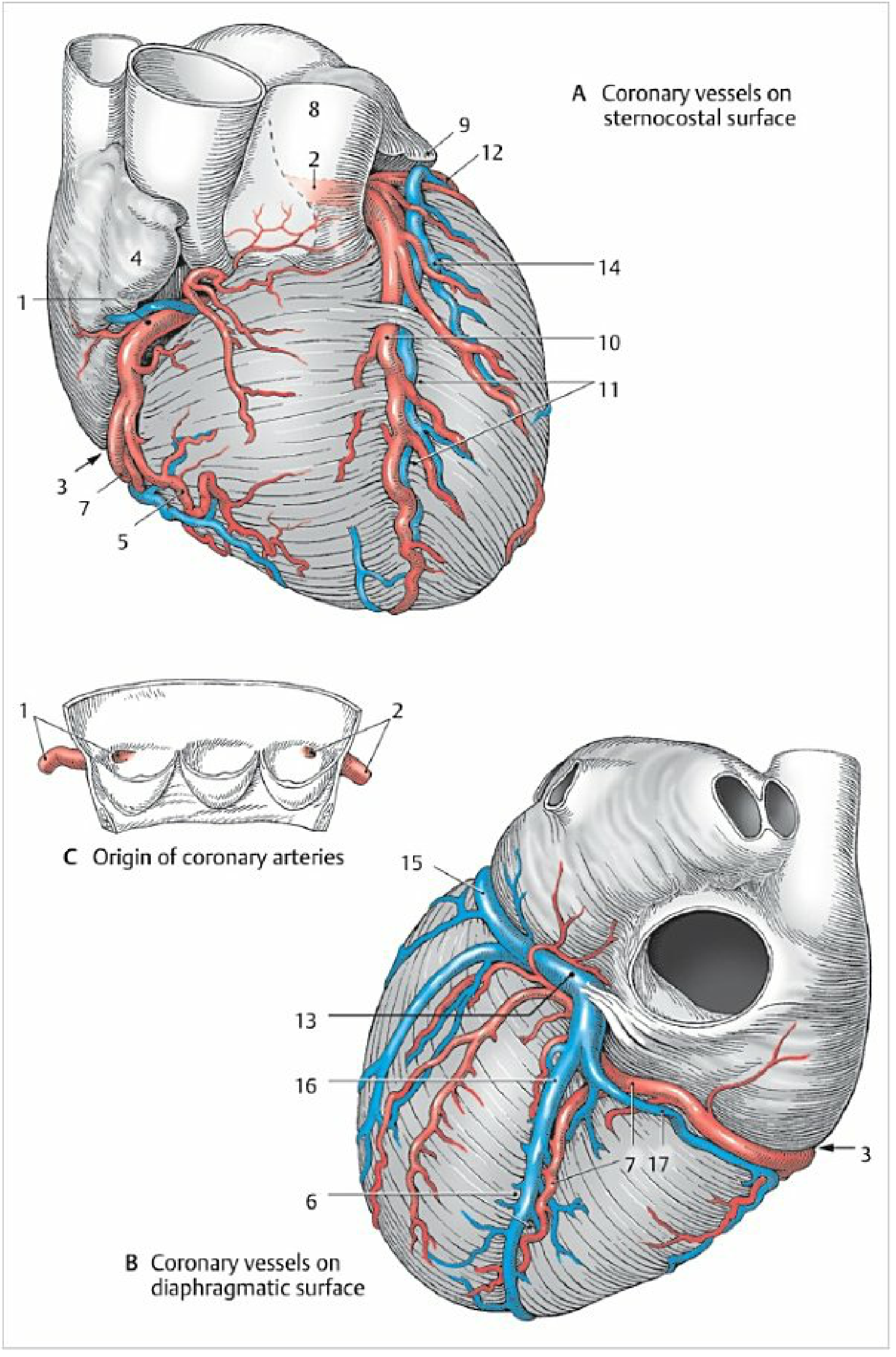
Color Atlas of Human Anatomy Vol 2, p. 58-59
Venous Drainage
About 85% of cardiac venous blood drains via the greater coronary venous system (coronary sinus and its tributaries); the remainder drains via small veins directly into cardiac chambers (thebesian veins).
Cardiac Veins - Anterior View
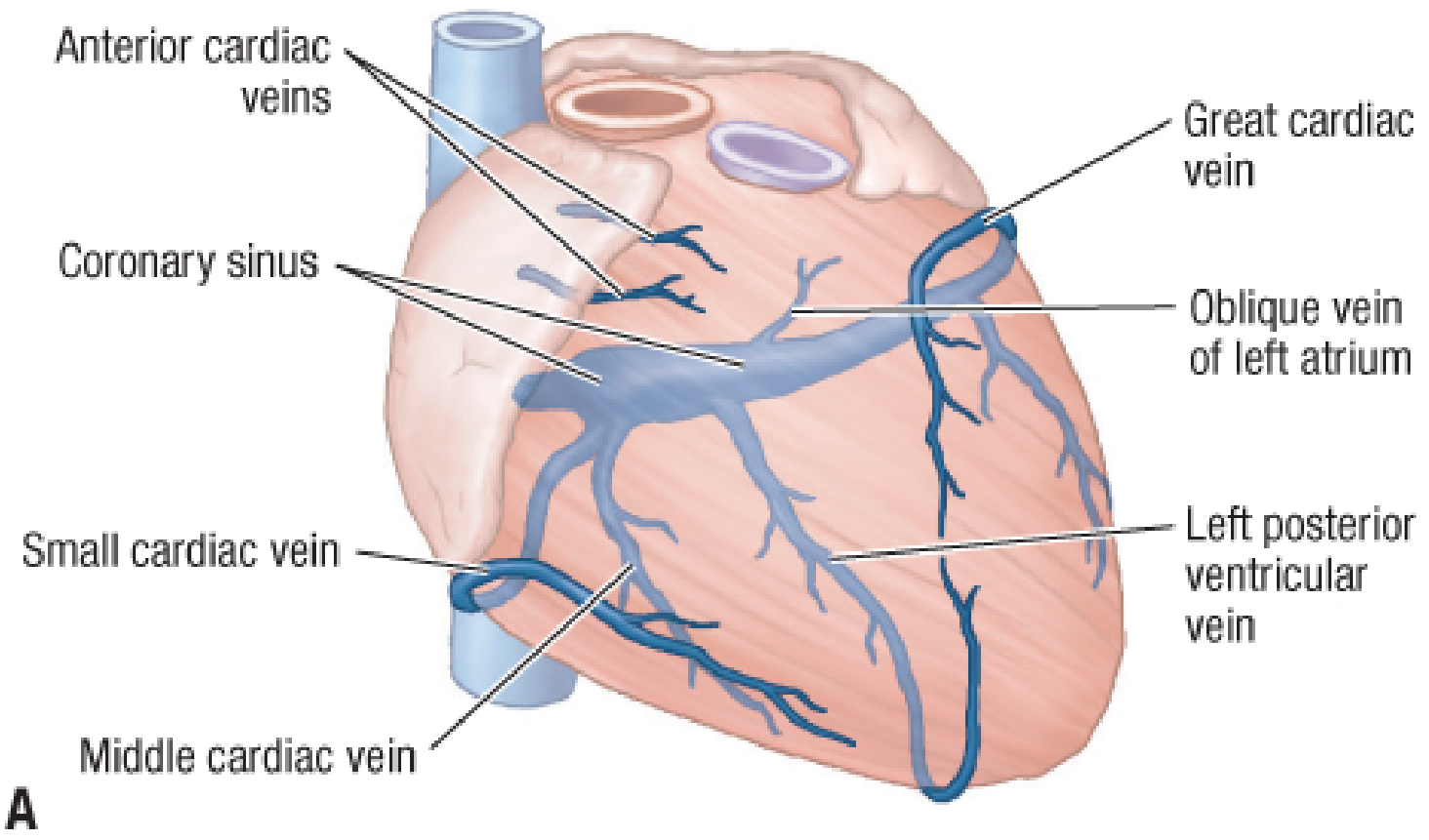
Fig. 273.7A - Cardiac veins, anterior view. Fischer's Mastery of Surgery
Cardiac Veins - Posteroinferior View
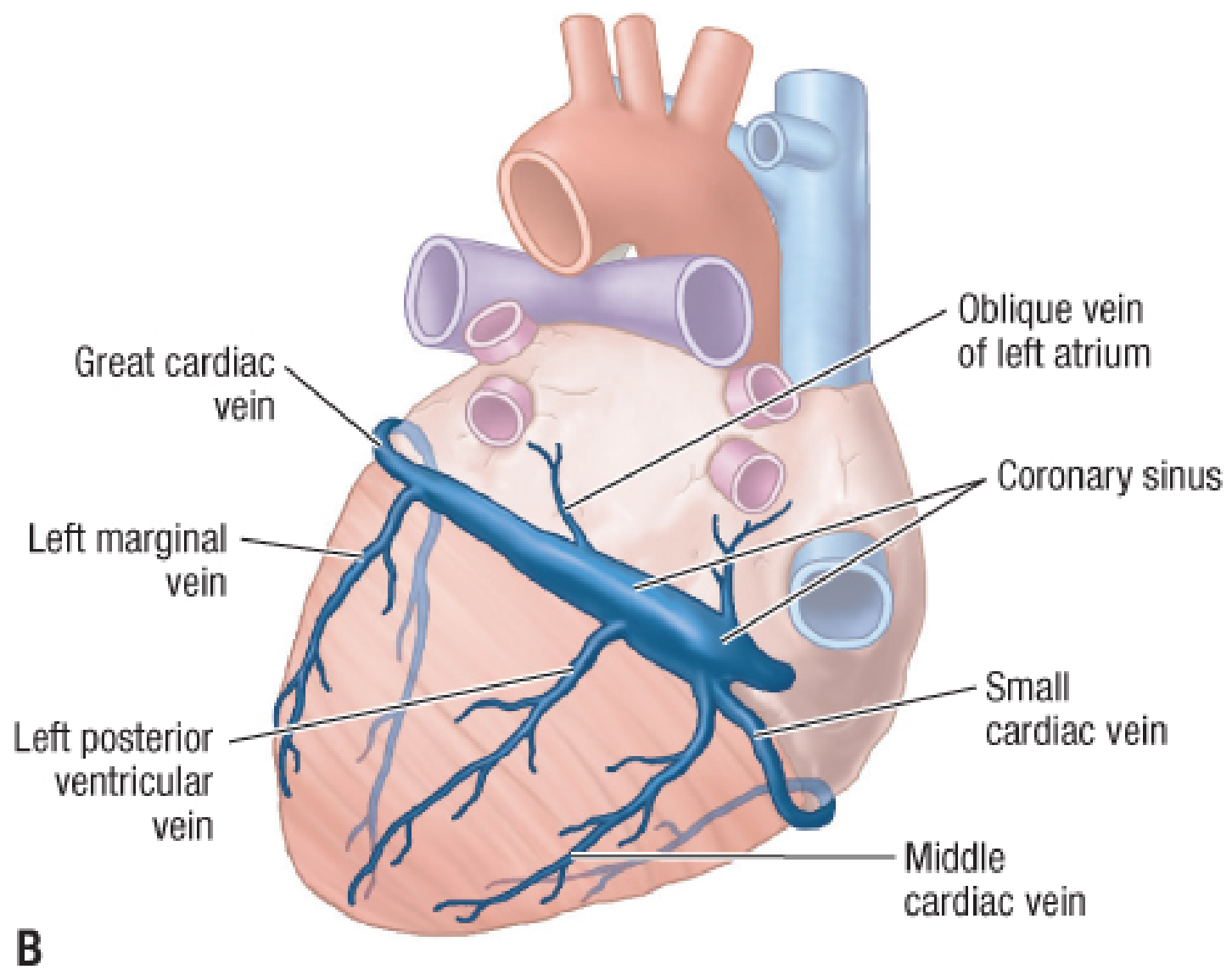
Fig. 273.7B - Cardiac veins, posteroinferior view. Fischer's Mastery of Surgery
The Coronary Sinus
- A wide venous channel running left to right in the posterior part of the coronary sulcus
- Ostium diameter: 5-15 mm
- Drains into the right atrium (between the tricuspid valve orifice and the inferior vena cava)
- Its transition from the great cardiac vein is marked by the valve of Vieussens (present in 80-90% of hearts) and entrance of the vein/ligament of Marshall (embryonic remnant of left SVC)
Major Tributaries of the Coronary Sinus
| Vein | Course | Corresponding Artery |
|---|---|---|
| Great cardiac vein | Starts at apex → ascends in anterior interventricular sulcus → turns left in coronary sulcus to coronary sinus | Accompanies LAD (anterior interventricular branch) |
| Middle cardiac vein | Starts at apex → posterior interventricular sulcus → right end of coronary sinus | Accompanies posterior interventricular artery (PDA) |
| Small cardiac vein | Begins as marginal vein → right coronary sulcus → right end of coronary sinus | Accompanies right marginal branch |
| Oblique vein of left atrium | Runs on posterior surface of left atrium | Remnant of embryonic left SVC |
| Left posterior ventricular vein | Left ventricular posterior surface | Left ventricular branches |
| Left marginal vein | Along obtuse margin | Left marginal branch |
Direct Drainage (Bypassing Coronary Sinus)
-
Anterior cardiac veins: Drain the anterior right ventricular wall, open directly into the right atrium
-
Thebesian (smallest cardiac) veins: Tiny vessels that open directly into all four cardiac chambers, especially the right atrium and right ventricle
-
Fischer's Mastery of Surgery, p. 7365; Fuster and Hurst's The Heart, p. 1070
Lymphatic Drainage
The heart has three overlapping lymphatic networks:
- Deep endocardial network
- Middle myocardial network
- Superficial epicardial network
Larger collecting vessels travel in the epicardium, accompanying the aorta and pulmonary trunk, and drain to the tracheobronchial and anterior mediastinal lymph nodes.
- Color Atlas of Human Anatomy Vol 2, p. 59
Clinical Terminology (Cardiology vs. Anatomy)
| Anatomical Name | Clinical Name |
|---|---|
| Short left coronary artery | Left main stem |
| Anterior interventricular branch | LAD (Left Anterior Descending) |
| Posterior interventricular branch | PDA (Posterior Descending Artery) |
| Circumflex branch | LCx |
Clinical Correlates
| Condition | Vessel involved | Anatomical basis |
|---|---|---|
| Anterior STEMI | LAD occlusion | Supplies anterior LV wall and anterior 2/3 of IVS |
| Inferior STEMI | RCA occlusion (right dominant) | Supplies inferior/posterior LV wall via PDA |
| Lateral STEMI | Circumflex occlusion | Supplies lateral and posterior LV wall |
| Complete heart block after inferior MI | RCA - AV nodal branch | RCA usually supplies AV node |
| Angina | Coronary stenosis | Coronaries are functional end arteries; collaterals insufficient for acute occlusion |
| Coronary artery bypass graft (CABG) | Bypasses stenosed coronaries | Great saphenous vein, internal thoracic artery, or radial artery used as conduits |
| Cardiac referred pain | MI visceral afferents | Follow sympathetic fibers entering spinal cord at T1-T4; pain referred to chest wall, left arm, jaw |
- Gray's Anatomy for Students, p. 242-244; Color Atlas of Human Anatomy Vol 2, p. 58
This is a shared conversation. Sign in to Orris to start your own chat.