Explain Heart disease in pregnancy
"heart disease" AND "pregnancy" AND management
Heart Disease in Pregnancy
- In the developed world: congenital heart disease (CHD) is the most common etiology
- In the developing world: rheumatic heart disease predominates
- Other causes include connective tissue disorders, cardiomyopathies, and ischemic disease
Hemodynamic Changes of Normal Pregnancy
| Parameter | Change |
|---|---|
| Plasma volume | +40% by 24 weeks |
| Cardiac output | +30-50% (rises from week 5, peaks at 28-34 weeks) |
| Stroke volume | +40% (peaks 28-31 weeks) |
| Heart rate | +10-20 bpm (main driver in 3rd trimester) |
| Systemic vascular resistance | Decreased (due to progesterone, prostaglandins) |
| Blood pressure | Decreases in 1st/2nd trimester, returns to baseline in 3rd |
Diagnosis: Normal vs. Pathological Findings
- Dyspnea (very common)
- Orthopnea
- Easy fatigability, dizziness, occasional syncope
- Dependent edema, basal lung rales
- Systolic murmurs (>95% of pregnant women)
- S3 gallop, small pericardial effusion
- Venous hums and mammary flow murmurs
- Severe dyspnea or dyspnea at rest
- Syncope with exertion
- Hemoptysis
- Paroxysmal nocturnal dyspnea
- Exertional chest pain
- Diastolic murmurs
- S4 gallop, cyanosis, clubbing
- Sustained cardiac arrhythmias
- Loud, harsh systolic murmurs
- ECG: non-specific ST/T changes and axis shifts are normal in pregnancy; interpret cautiously
- Echocardiography: safe and useful - chambers appear enlarged, EF and stroke volume are higher than non-pregnant norms
- Chest X-ray and radionuclide imaging: avoid unless essential for maternal safety
- A small pericardial effusion is a normal finding in pregnancy
Preconception Counseling
- Complete workup: history and exam (including O2 saturation), ECG, echocardiogram, CT/MR angiography where aortic evaluation is needed, and consideration of cardiopulmonary stress testing
- Medication review: adjust or discontinue teratogenic/contraindicated drugs
- Functional capacity: exercise capacity >80% of predicted is associated with more favorable outcomes (European guidelines)
- Fetal echocardiogram at 20-22 weeks if a parent has CHD (risk of CHD in offspring increases from 0.8% to 2-6%)
- Genetic counseling for heritable conditions (Marfan syndrome, HCM, long-QT syndrome)
- Large intracardiac shunt with significant chamber enlargement, mild pulmonary hypertension, or arrhythmia
- Severe coarctation of the aorta
- Severe mitral or aortic stenosis/regurgitation
- Residual or uncorrected congenital heart disease
Conditions Where Pregnancy is Contraindicated (WHO Class IV)
| Condition | Reason |
|---|---|
| Pulmonary arterial hypertension | Maternal mortality 25-50% |
| Severe systemic ventricular dysfunction (EF <30% or NYHA III-IV) | Decompensation, death |
| Previous peripartum cardiomyopathy with residual LV impairment | High recurrence risk |
| Severe symptomatic aortic stenosis | Fixed outflow obstruction |
| Systemic RV with moderate/severe dysfunction | Cannot handle volume load |
| Severe aortic dilatation (>45 mm Marfan/HTAD, >50 mm bicuspid AoV, Turner ASI >25 mm/m²) | Dissection risk |
| Severe mitral stenosis | Cannot tolerate volume/rate increase |
| Vascular Ehlers-Danlos syndrome | Rupture risk |
| Severe/re-coarctation | Hypertension, rupture |
| Fontan circulation with any complication | Hemodynamic deterioration, death |
Risk Stratification Models
Modified WHO Classification
- Class I: No detectable risk (e.g., small VSD, repaired simple lesions)
- Class II: Small increased risk (e.g., repaired TOF, most arrhythmias)
- Class III: Significantly increased risk - requires expert care (e.g., mechanical valve, Fontan, systemic RV)
- Class IV: Extremely high risk - pregnancy contraindicated (listed above)
CARPREG II Score
- 0-1 points: 5% cardiac event rate
-
4 points: 41% cardiac event rate
- Events predominantly: heart failure and arrhythmias
Specific Heart Diseases in Pregnancy
Valvular Heart Disease
- The rise in cardiac output + heart rate shortens diastolic filling time, dramatically raising left atrial pressure
- Risk: pulmonary edema, atrial fibrillation, systemic embolism
- Management: heart rate control (beta-blockers), diuretics for congestion; percutaneous balloon commissurotomy if severe and refractory; anticoagulation if AF develops
- Moderate-to-severe symptomatic AS poorly tolerated (fixed obstruction in the face of increased demands)
- Pregnancy contraindicated if severe and symptomatic; consider balloon valvuloplasty pre-pregnancy
- Bioprosthetic: no anticoagulation issues, but accelerated structural valve deterioration during pregnancy
- Mechanical: require anticoagulation throughout - this is a major management challenge (see below)
Anticoagulation with Mechanical Valves
- Warfarin throughout: lowest maternal thrombosis risk but warfarin embryopathy (6-10 weeks), fetal hemorrhage, miscarriage
- LMWH in 1st trimester, warfarin in 2nd/3rd: reduces embryopathy; anti-Xa monitoring essential
- UFH throughout: no fetal risk but high maternal thrombosis rates with mechanical valves
Congenital Heart Disease
Cardiomyopathies
- LV dysfunction developing in the last month of pregnancy or within 5 months postpartum, without another identifiable cause
- Incidence 1:3000-1:4000 in the US (higher in Africa, Haiti)
- Risk factors: multiparity, advanced maternal age, multiple gestation, preeclampsia, African descent
- Presentation: heart failure symptoms
- Treatment: standard heart failure therapy adapted for pregnancy/lactation; bromocriptine may accelerate LV recovery
- Recovery: ~50% recover LV function; future pregnancy carries high recurrence risk if LV function has not normalized
- Generally tolerated, though volume depletion and tachycardia are poorly tolerated (worsen obstruction)
- Beta-blockers continued throughout pregnancy
Hypertensive Disorders of Pregnancy
- Complicates ~10% of pregnancies
- Gestational hypertension: BP ≥140/90 mmHg after 20 weeks, no proteinuria
- Preeclampsia: hypertension + proteinuria/end-organ damage - systemic syndrome with placental origin; can progress to seizures (eclampsia)
- Severe if BP ≥160/110 mmHg - requires urgent treatment
- First-line antihypertensives: labetalol, nifedipine, alpha-methyldopa
- Preeclampsia/eclampsia history increases future risk of cardiovascular disease
Cardiac Arrhythmias
Ischemic Heart Disease and Spontaneous Coronary Artery Dissection (SCAD)
- Acute MI in pregnancy is rare but increasing (older mothers, more risk factors)
- SCAD is the most common cause of ACS in young pregnant/postpartum women - treat conservatively when possible (PCI preferred over thrombolytics if intervention needed)
- Thrombolytics are relatively contraindicated during pregnancy
Pulmonary Arterial Hypertension
- Maternal mortality 25-50%; pregnancy is contraindicated
- If pregnancy occurs, manage in expert center; advanced PAH therapies; planned early delivery
Infective Endocarditis in Pregnancy
- Rare but associated with high maternal and fetal mortality
- Management follows standard principles; surgery can be performed in 2nd trimester if necessary
Cardiovascular Medications: Safety in Pregnancy
| Drug/Class | Status |
|---|---|
| ACE inhibitors | Contraindicated (fetal renal dysgenesis, oligohydramnios) |
| ARBs | Contraindicated |
| Aldosterone antagonists (spironolactone) | Contraindicated |
| NOACs (direct oral anticoagulants) | Contraindicated |
| Endothelin receptor antagonists (bosentan) | Contraindicated |
| Riociguat | Contraindicated |
| Amiodarone | Last resort only (fetal hypothyroidism, growth restriction) |
| Nitroprusside | Last resort only (cyanide toxicity risk) |
| Atenolol | Requires shared decision-making (fetal growth restriction) |
| Labetalol, metoprolol, beta-blockers | Generally acceptable; monitor fetal growth |
| Nifedipine, other dihydropyridines | Safe for hypertension |
| Alpha-methyldopa | Safe; first-line for chronic hypertension |
| Digoxin | Safe |
| Heparin (UFH, LMWH) | Safe (do not cross placenta) |
| Warfarin | Use with caution; embryopathy risk 1st trimester |
| Low-dose aspirin | Safe; used in preeclampsia prevention |
| Furosemide | Use with caution; risk of placental underperfusion |
Delivery Planning
- Mode of delivery should be guided primarily by obstetric indications - most women with CVD can deliver vaginally
- Continuous hemodynamic monitoring during labor is recommended for high-risk patients
- Epidural analgesia reduces hemodynamic fluctuations from pain - beneficial in most cardiac conditions (use cautiously with severe AS or obstructive physiology)
- The second stage (Valsalva) is the highest-risk phase - assisted delivery (forceps/vacuum) considered selectively; passive laboring down reduces Valsalva requirement
- Postpartum period: highest risk window due to autotransfusion - close monitoring for at least 24-48 hours; pulmonary edema and decompensation most common here
Cardiopulmonary Resuscitation in Pregnancy
- Follow standard ACLS protocols - life-saving medications must not be withheld
- Critical modification: displace the uterus 15 degrees to the left (left lateral tilt ~1.5 cm) to relieve aortocaval compression and improve venous return
- Perimortem cesarean section (within 4-5 minutes of arrest) may improve maternal resuscitation by relieving caval compression
Multidisciplinary Care
- Cardiologist (with expertise in pregnancy)
- Maternal-fetal medicine specialist
- Obstetric anesthesiologist
- Neonatologist (for high-risk deliveries)
- Cardiac surgery availability when needed
Mediators of preeclampsia
"preeclampsia" AND "pathogenesis" AND "mediators"
Mediators of Preeclampsia
Stage 1: Defective Trophoblast Invasion and Placental Ischemia
- Abnormal expression of implantation-related adhesion molecules and receptors on trophoblasts
- Failure of trophoblasts to undergo "pseudovasculogenesis" (acquiring endothelial cell surface markers)
- Abnormal HLA-G expression by invasive cytotrophoblasts - HLA-G normally induces immune tolerance at the maternal-fetal interface; its loss may provoke rejection-like immunologic damage
- Complement deposition within decidual vessels (resembling transplant rejection)
- Elevated hypoxia-inducible factor 1α (HIF-1α) - a marker of placental cellular oxygen deprivation
Stage 2: Systemic Mediators Released into the Maternal Circulation
A. Angiogenic Imbalance (Central Pathway)
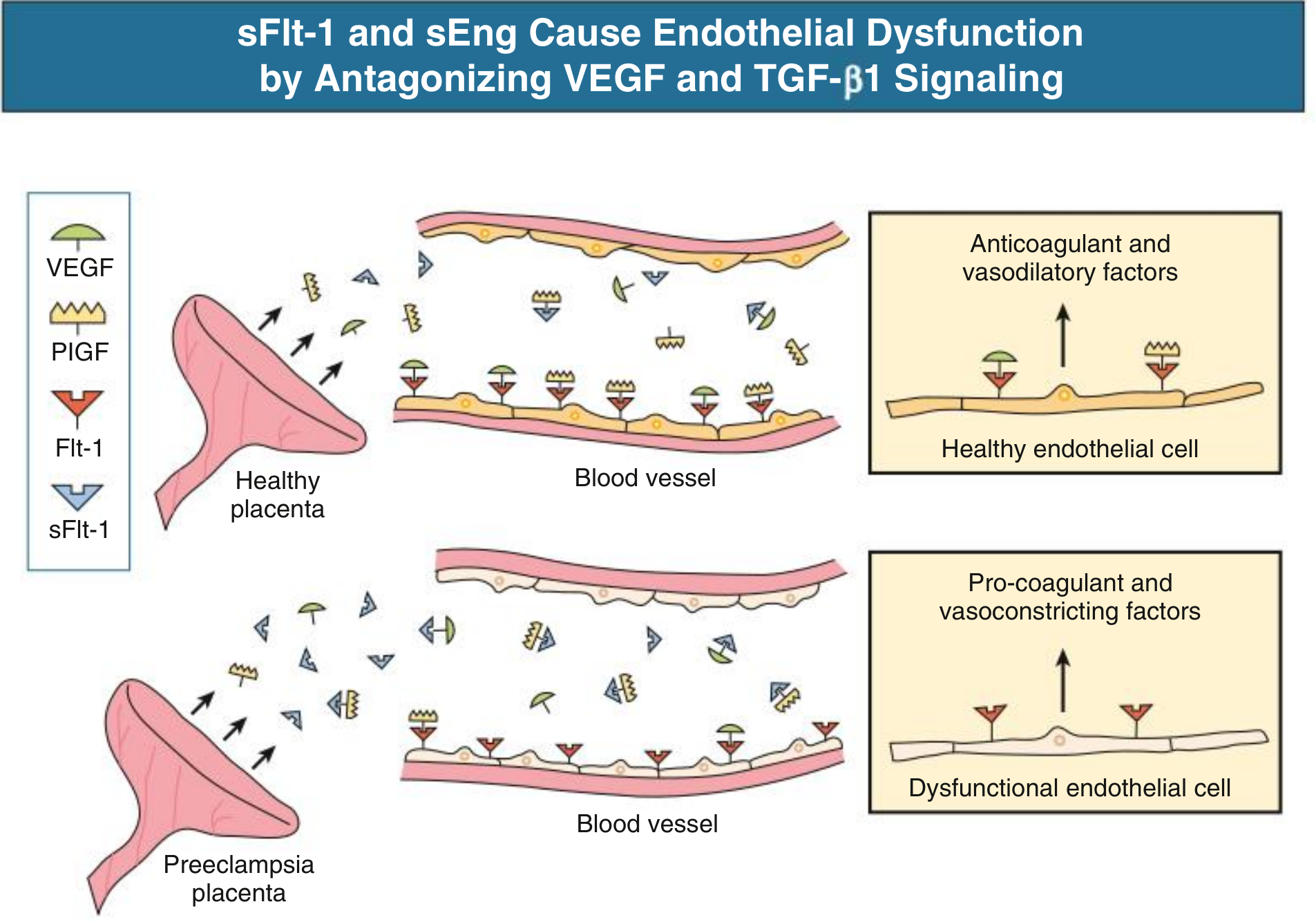
1. sFlt-1 (Soluble Fms-like Tyrosine Kinase-1) - the key villain
- sFlt-1 is a splice variant of the full-length VEGF receptor FLT-1, lacking the transmembrane and cytoplasmic domains
- It acts as a soluble decoy receptor - circulating freely in plasma and binding VEGF and PlGF with high affinity, preventing them from reaching endothelial cell-surface receptors
- The ischemic placenta massively upregulates sFlt-1 production weeks before clinical preeclampsia manifests
- Elevated sFlt-1 → decreased free VEGF and free PlGF → endothelial dysfunction
- In the kidney: loss of VEGF signaling causes glomerular endotheliosis (swelling of fenestrated endothelial cells, obliterating capillary lumens) - the pathognomonic renal lesion of preeclampsia - leading to proteinuria
2. PlGF (Placental Growth Factor) - depleted
- PlGF is a proangiogenic VEGF family member secreted by the placenta
- Normally promotes endothelial survival, vasodilation, and normal placental angiogenesis
- In preeclampsia: PlGF is decreased both due to reduced placental production and increased scavenging by sFlt-1
- The sFlt-1:PlGF ratio ≥40 is associated with a high risk of developing preeclampsia with severe features within 2 weeks - used clinically for risk prediction
3. VEGF (Vascular Endothelial Growth Factor) - depleted
- Required for endothelial cell homeostasis and survival
- Free VEGF is scavenged by excess sFlt-1
- Loss of VEGF signaling → decreased prostacyclin and NO production → endothelial dysfunction, vasoconstriction, proteinuria
4. Soluble Endoglin (sEng) - the co-conspirator
- sEng is the soluble form of endoglin, a TGF-β co-receptor expressed on syncytiotrophoblasts and endothelial cells
- In preeclampsia, placental sEng is elevated and released into the circulation
- sEng blocks TGF-β1 signaling on endothelial cells - TGF-β1 normally promotes vasodilation via eNOS activation
- Acts synergistically with sFlt-1 to worsen endothelial dysfunction; in animal models, combined sFlt-1 + sEng infusion produces a severe HELLP-like syndrome
| Factor | Direction in Preeclampsia | Role |
|---|---|---|
| sFlt-1 | ↑↑ (excess) | Antiangiogenic - scavenges VEGF/PlGF |
| sEng | ↑ (excess) | Antiangiogenic - blocks TGF-β1 |
| PlGF | ↓ (depleted) | Proangiogenic - needed for endothelial health |
| VEGF | ↓ (scavenged) | Endothelial survival, vasodilation |
B. Prostacyclin-Thromboxane Imbalance
- Prostacyclin (PGI₂) is decreased - less endothelial production
- Thromboxane A2 (TXA₂) is increased - a potent vasoconstrictor and platelet activator, produced by platelets and trophoblasts
- The TXA₂/PGI₂ ratio is shifted toward vasoconstriction and platelet aggregation
- This imbalance also increases sensitivity to angiotensin II (normally pregnant women are relatively resistant to Ang II; preeclamptic women become highly sensitive)
- Aspirin (low-dose) acts by inhibiting TXA₂ production from platelets >> PGI₂ inhibition → restores the balance → this is the basis for aspirin prophylaxis in high-risk women
C. Nitric Oxide (NO) Deficiency
- Endothelial nitric oxide synthase (eNOS) is the major source of vascular NO - a critical vasodilator and inhibitor of platelet aggregation
- In normal pregnancy, NO is a major mediator of the fall in systemic vascular resistance
- In preeclampsia: NO production is reduced due to endothelial injury/dysfunction
- Additionally, NOS becomes uncoupled (producing superoxide instead of NO), contributing to oxidative stress
- Evidence: elevated tissue nitrotyrosine (a product of NO reacting with superoxide) in placenta and vasculature of preeclamptic women
- The loss of NO → impaired vasodilation → hypertension + platelet activation
D. Endothelin-1 (ET-1) - the Final Common Vasoconstrictor Pathway
- ET-1 is a potent endothelium-derived vasoconstrictor
- In preeclampsia: ET-1 levels are markedly elevated in placental tissue and plasma
- Multiple experimental models (placental ischemia, sFlt-1 infusion, TNF-α infusion, AT1-AA infusion) all produce elevated tissue ET-1
- Hypertension in these models can be attenuated by ET receptor antagonism - strongly suggesting ET-1 is a final common pathway linking placental ischemia to elevated BP
- ET-1 also promotes sodium retention in the kidney, contributing to volume expansion
E. Angiotensin II Hypersensitivity and AT1-AA (Autoantibodies)
- Preeclamptic women have markedly increased vascular sensitivity to angiotensin II compared to normal pregnant women
- A key mechanism: AT1-receptor agonistic autoantibodies (AT1-AA) - IgG autoantibodies identified in preeclamptic women that bind and activate the AT1 receptor
- AT1-AA can:
- Stimulate production of sFlt-1 from trophoblasts and vascular smooth muscle cells
- Activate NADPH oxidase → reactive oxygen species
- Promote ET-1 production
- Stimulate plasminogen activator inhibitor-1 (PAI-1) → impaired fibrinolysis, thrombosis
- Heterodimerization of AT1 receptors with bradykinin B2 receptors has also been proposed as a mechanism of Ang II hypersensitivity
- This autoimmune component links the immunologic tolerance failure with the vasoconstrictor phenotype
F. Oxidative Stress and Reactive Oxygen Species (ROS)
- The ischemic placenta generates excess reactive oxygen species (ROS) through xanthine oxidase, NADPH oxidase, and uncoupled eNOS
- Superoxide quenches NO (forming peroxynitrite/nitrotyrosine) → reduces bioavailable NO
- Oxidative stress activates NF-κB → proinflammatory cytokine production
- Activates lipid peroxidation → oxidized LDL, lipid peroxides detected in preeclampsia
- Excess ROS causes syncytiotrophoblast necrosis/apoptosis → release of trophoblastic fragments (microparticles) into the maternal circulation → endothelial activation
G. Inflammatory Cytokines and Immune Dysregulation
- Placental ischemia and oxidative stress trigger release of TNF-α, IL-6, IL-1β into the maternal circulation
- TNF-α: directly promotes endothelial dysfunction, stimulates sFlt-1 production, activates AT1-AA effects
- Impaired Treg-mediated immune tolerance: normal pregnancy requires regulatory T cells (Tregs) to establish tolerance to paternal antigens; in preeclampsia this tolerance is reduced
- NK cell dysregulation: decidual NK cells normally guide trophoblast invasion; aberrant NK activity contributes to poor spiral artery remodeling
- Dendritic cells and macrophages: abnormal polarization promotes a proinflammatory M1 phenotype in the decidua
- Abnormal HLA-C/KIR interactions between trophoblasts and decidual NK cells are genetically linked to preeclampsia risk
- Complement activation (C3d, C4d deposition in spiral arteries) resembling allograft rejection
H. Coagulation Activation
- Decreased prostacyclin and NO → platelet activation and aggregation
- Release of von Willebrand factor (vWF) from activated endothelium → enhanced platelet adhesion
- Elevated fibronectin (marker of endothelial damage)
- Elevated PAI-1 (promoted by AT1-AA, sFlt-1, and TNF-α) → impaired fibrinolysis
- Microthrombi formation → end-organ ischemia (liver, kidney, brain)
- Severe form: HELLP syndrome (hemolysis, elevated liver enzymes, low platelets)
Integrated Pathophysiologic Model
Genetic predisposition + Paternal factors + Immunologic intolerance
↓
Defective trophoblast invasion of spiral arteries
↓
Uteroplacental ischemia → hypoxia, oxidative stress, NF-κB activation
↓
Placenta releases into maternal circulation:
• ↑ sFlt-1 (scavenges VEGF, PlGF) → endothelial dysfunction
• ↑ sEng (blocks TGF-β1) → endothelial dysfunction
• ↑ TNF-α, IL-6, trophoblast microparticles → inflammation
• ↑ AT1-AA (activates AT1 receptor) → Ang II hypersensitivity
↓
Maternal systemic endothelial dysfunction
• ↓ Prostacyclin, ↓ NO → vasoconstriction, platelet activation
• ↑ Thromboxane A2, ↑ ET-1 → vasoconstriction
• ↑ Oxidative stress, ↑ coagulation activation
↓
Clinical syndrome:
Hypertension | Proteinuria (glomerular endotheliosis)
Thrombocytopenia | Liver dysfunction (HELLP)
Cerebral edema/seizures (eclampsia) | Pulmonary edema
Clinical Significance of Mediators
| Mediator | Clinical Use |
|---|---|
| sFlt-1/PlGF ratio ≥40 | Predicts imminent severe preeclampsia (within 2 weeks) |
| Low-dose aspirin prophylaxis | Corrects TXA₂/PGI₂ imbalance; prevents preeclampsia in high-risk women |
| Anti-VEGF therapy (e.g., bevacizumab) | Known to cause preeclampsia-like syndrome - validates VEGF mechanism |
| Magnesium sulfate | Anticonvulsant for eclampsia; may also reduce ET-1 effects |
| Calcium supplementation | Low calcium → high renin → AngII activation; supplementation reduces risk |
Mediators of preeclampsia
Mediators of Preeclampsia - Summary
Stage 1: Failed Spiral Artery Remodeling
- Shallow trophoblast invasion leaves spiral arteries narrow and vasoactive
- Results in uteroplacental ischemia, oxidative stress, and NF-κB activation
- Complement deposition and HLA-G loss reflect the immunologic tolerance failure
Stage 2: Circulating Mediators
| Mediator | Source | Effect |
|---|---|---|
| ↑ sFlt-1 (soluble VEGF receptor) | Ischemic placenta | Scavenges free VEGF and PlGF → endothelial dysfunction, glomerular endotheliosis |
| ↓ PlGF | Depleted by sFlt-1 | Loss of proangiogenic signaling |
| ↑ sEng (soluble endoglin) | Syncytiotrophoblast | Blocks TGF-β1 → synergizes with sFlt-1 |
| ↓ Prostacyclin (PGI₂) | Dysfunctional endothelium | Loss of vasodilation + platelet inhibition |
| ↑ Thromboxane A₂ | Platelets/trophoblasts | Vasoconstriction + platelet aggregation |
| ↓ Nitric oxide (NO) | Uncoupled eNOS | Loss of vasodilation; excess superoxide → oxidative stress |
| ↑ Endothelin-1 (ET-1) | Endothelium | Final common vasoconstrictor pathway; blocked by ET antagonists in animal models |
| ↑ AT1-AA (AT1 receptor autoantibodies) | Maternal immune response | Activates AT1R → ↑ Ang II sensitivity, ↑ sFlt-1, ↑ PAI-1, ↑ ROS |
| ↑ TNF-α, IL-6, IL-1β | Placenta/macrophages | Endothelial inflammation, further sFlt-1 upregulation |
| ↑ Reactive oxygen species | NADPH oxidase, uncoupled eNOS | Quench NO, lipid peroxidation, trophoblast necrosis |
| ↑ PAI-1 | Endothelium (AT1-AA driven) | Impaired fibrinolysis → microthrombi → HELLP |
The Central Diagram
Clinical Correlates
- sFlt-1:PlGF ratio ≥40 → predicts severe preeclampsia within 2 weeks (used clinically)
- Low-dose aspirin → shifts TXA₂/PGI₂ balance back toward vasodilation (prophylaxis)
- Anti-VEGF cancer drugs (bevacizumab) → mimic preeclampsia, validating the VEGF pathway
- Magnesium sulfate → prevents eclamptic seizures (also attenuates ET-1 effects)
Anemia in pregnancy
"anemia" AND "pregnancy" AND management
Anemia in Pregnancy
Physiologic (Dilutional) Anemia of Pregnancy
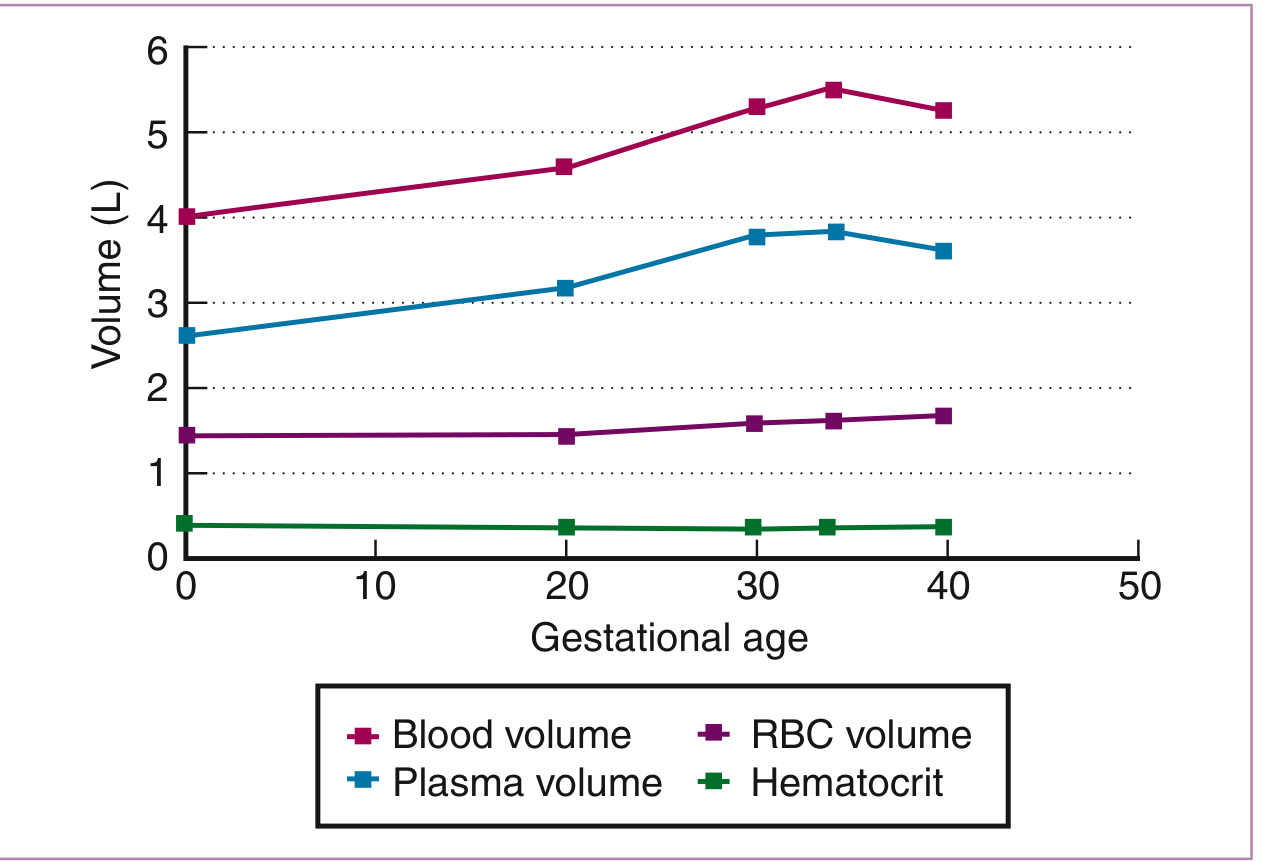
- Blood volume increases by 40-45% by 34 weeks, driven disproportionately by plasma volume expansion (+47%) versus red cell mass expansion (+17%)
- This "hemodilution" lowers Hb, hematocrit, and RBC count - but does not change MCV or MCHC (key distinguishing feature from iron deficiency)
- Physiologic anemia peaks at 28-34 weeks
| Trimester | Hb (g/dL) - Normal Lower Limit |
|---|---|
| 1st trimester | ≥11.0 g/dL |
| 2nd & 3rd trimester | ≥10.0 g/dL |
- Normocytic anemia with Hb >11 g/dL (1st trimester) or >10 g/dL (2nd/3rd) → physiologic anemia, no further workup needed
- Lower values, or microcytic or macrocytic morphology → must investigate
Iron Deficiency Anemia (IDA) - Most Common Pathologic Cause
Iron Demands of Pregnancy
| Iron Required For | Average (mg) |
|---|---|
| External iron loss | 170 |
| Expansion of RBC mass | 450 |
| Fetal iron | 270 |
| Placenta and cord | 90 |
| Blood loss at delivery | 150 |
| Total requirement | ~1130 mg |
Iron Transfer to the Fetus
- The fetal compartment preferentially extracts iron from the mother via transferrin receptors on placental syncytiotrophoblast
- If maternal iron is low, placental transferrin receptor expression upregulates to maintain fetal supply
- Iron deficiency detectable in ~11% of pregnant women in the third trimester (Harrison's 22e)
Stages of Iron Deficiency
- Prelatent - depleted marrow stores; ↓ serum ferritin only; Hb normal
- Latent - ↓ serum iron, ↑ TIBC, ↓ transferrin saturation; Hb still normal
- Overt IDA - ↓ Hb, eventually ↓ MCV (microcytic hypochromic anemia)
Diagnosis
| Test | Finding in IDA |
|---|---|
| Serum ferritin | Best single test - <12 μg/L = IDA; <20 μg/L = iron depletion |
| Serum iron | Decreased |
| TIBC | Increased (rises through pregnancy) |
| Transferrin saturation | Decreased (<16%) |
| MCV | Decreased (late finding) |
| Blood smear | Microcytic, hypochromic RBCs |
| Soluble transferrin receptor (sTfR) | Increased - useful when ferritin is unreliable (e.g., inflammatory states, as ferritin is an acute phase reactant) |
Note: Ferritin is an acute phase reactant - it may be falsely elevated in chronic inflammatory disease, masking iron deficiency. In such cases, sTfR is more reliable.
Effects on Mother and Fetus
- Preterm delivery
- Low birth weight (LBW)
- Perinatal death
- Impaired maternal immune function and fatigue
- Maternal anemia → neonatal anemia (Cochrane 2024 meta-analysis confirms the association)
- Postpartum hemorrhage risk is magnified
Treatment
- Recommended daily dose: 60 mg of elemental iron during 2nd and 3rd trimesters
- Standard preparations: ferrous sulfate (325 mg tablet = ~65 mg elemental iron), ferrous gluconate, ferrous fumarate
- Take on empty stomach with vitamin C (ascorbic acid) to enhance absorption; avoid with calcium, antacids, tea
- Side effects: nausea, constipation - dose can be split or given on alternate days to improve tolerance
- Iron supplementation reduces incidence of anemia by up to 73%
- The Cochrane review (2024, PMID 39145520) confirms daily oral iron improves maternal hemoglobin and reduces IDA rates
- Indications: failure or intolerance of oral iron, severe anemia in late pregnancy, malabsorption, inflammatory bowel disease
- Options: iron sucrose, ferric carboxymaltose, low molecular weight iron dextran
- More rapid repletion; ferric carboxymaltose allows a single large-dose infusion
- Safe in 2nd and 3rd trimester; avoid in 1st trimester
- Reserved for severe, symptomatic anemia (Hb <7 g/dL) or hemodynamic instability
- Each unit of packed RBCs raises Hb by ~1 g/dL
- 1st trimester and again at 24-28 weeks (Harrison's)
- Measure ferritin alongside Hb to detect pre-anemic iron depletion
Megaloblastic Anemia - Second Most Common Nutritional Anemia
Folate Deficiency
- Non-pregnant: 400 μg/day
- Pregnant: 600 μg/day (a ~50% increase)
- Increase is driven by: enhanced fetal demand, increased erythropoiesis, and hemodilution
- Dietary polyglutamate folates require intestinal conjugase for absorption - activity reduced by anticonvulsants, oral contraceptives, alcohol, sulfa drugs
- Multiple gestation multiplies the demand further
- Hemolytic anemias also increase folate requirements
- Megaloblastic anemia
- Neural tube defects (NTDs) - spina bifida, anencephaly (risk reduced by 50-70% with periconceptional folic acid supplementation)
- Increased risk of placental abruption, preterm delivery
- Prophylaxis: 0.4-0.8 mg (400-800 μg) folic acid daily starting at least 1 month before conception and through the first 12 weeks
- Women with previous NTD-affected pregnancy: 4-5 mg/day (high-dose)
- Treatment of established deficiency: 1-5 mg/day
- In countries with food fortification (e.g., US), 0.8 mg/day is sufficient to prevent deficiency in most women
Vitamin B12 Deficiency
- Less common than folate deficiency in pregnancy but important
- Risk groups: strict vegetarians/vegans, women with pernicious anemia (anti-intrinsic factor antibodies), prior gastric surgery, Crohn's disease
- Presents with macrocytic anemia + neurologic symptoms (subacute combined degeneration - peripheral neuropathy, posterior column signs)
- Important distinction: treating B12 deficiency with folate alone corrects anemia but does not prevent neurological damage - B12 must be replaced
- Diagnosis: serum B12 <118-130 pg/mL (range varies by trimester); positive anti-intrinsic factor antibody in pernicious anemia
- Treatment: parenteral cyanocobalamin or hydroxocobalamin; oral high-dose B12 may be used if parenteral is not available
Laboratory Reference Ranges in Pregnancy (Creasy & Resnik)
| Test | Range |
|---|---|
| MCV | 81-99 μm³ (varies by trimester) |
| MCHC | 32-35 g/dL |
| Serum ferritin | >20 μg/L (1st); decreases through pregnancy |
| Serum iron | 30-178 μg/dL (varies by trimester) |
| TIBC | 235-597 μg/dL (rises through pregnancy) |
| Transferrin saturation | 16-60% |
| Serum folate | 8-240 μg/L (varies) |
| Serum B12 | 99-656 pg/mL (varies) |
| Reticulocyte count | 0.5-1.5% |
| Direct Coombs | Negative |
Hemolytic Anemias in Pregnancy
Hemoglobinopathies
- Particularly high-risk in pregnancy
- Maternal complications: increased vaso-occlusive crises (pain), acute chest syndrome, stroke, infection, pulmonary hypertension, preeclampsia, peripartum cardiomyopathy
- Fetal complications: growth restriction, preterm birth, fetal death
- Management: multidisciplinary team; prophylactic blood transfusions in severe cases; hydroxyurea is teratogenic - must be discontinued before conception; folic acid supplementation; aggressive pain management (avoid NSAIDs in 3rd trimester); Pneumococcal/meningococcal vaccination
- Hemoglobinopathy screening (MCV, MCH, Hb electrophoresis) is recommended for all pregnant women
- Generally uncomplicated; no increased hemolysis, but slight increased risk of UTI and hematuria
- Alpha-thalassemia trait/beta-thalassemia trait: usually tolerated, microcytic hypochromic picture
- Beta-thalassemia major: severe anemia requiring transfusion
- Hemoglobin H disease (α-thalassemia): moderate hemolytic anemia; may worsen in pregnancy
Hereditary Spherocytosis (HS)
- Autosomal dominant structural defect in RBC membrane
- Can cause hemolytic crises in pregnancy (precipitated by infection, trauma, increased splenic blood flow)
- Diagnosis: EMA flow cytometry (most sensitive/specific) - more reliable than older osmotic fragility test
- Pre-pregnancy splenectomy reduces morbidity; folic acid supplementation essential
Autoimmune Hemolytic Anemia (AIHA)
- Warm-reactive IgG antibodies (Rh system) - associated with lupus, lymphoproliferative disorders, drugs (penicillin, α-methyldopa), viral infections
- Cold-reactive IgM antibodies (anti-I/i) - mycoplasma, infectious mononucleosis
- Diagnosis: positive direct Coombs (direct antiglobulin) test, macrocytic/hyperproliferative smear with spherocytes
- Treatment: corticosteroids, blood transfusion, IV immunoglobulin; rarely splenectomy
- Pregnancy-induced AIHA (rare): resolves spontaneously after delivery
Aplastic Anemia
- Rare; pancytopenia from bone marrow failure
- Management: transfusion support; immunosuppression (cyclosporine); stem cell transplantation deferred if possible; folic acid supplementation
- Pregnancy itself can trigger or worsen aplastic anemia
Approach to Anemia in Pregnancy
Hb < 11 g/dL (1st trimester) or < 10 g/dL (2nd/3rd trimester)
↓
Check MCV, blood smear, ferritin
↓
┌──────────────┬──────────────┬──────────────┐
Microcytic Normocytic Macrocytic
(↓ MCV) (normal MCV) (↑ MCV)
↓ ↓ ↓
Iron deficiency Dilutional Folate deficiency
(↓ ferritin, anemia Vit B12 deficiency
↑ TIBC) Hemolysis Hypothyroidism
Thalassemia (↑ retics, Drug effect
Sideroblastic Coombs test, (anticonvulsants,
anemia ↑ LDH, ↓Hb) methotrexate)
Blood loss
Anemia of
chronic disease
- Hb electrophoresis: all women (screen for hemoglobinopathy)
- Peripheral blood smear: always useful for morphology
- Reticulocyte count: distinguishes hypo- vs. hyperproliferative anemia
- Direct Coombs: if hemolysis suspected
Maternal and Fetal Consequences of Anemia
| Maternal | Fetal/Neonatal |
|---|---|
| Fatigue, dyspnea, palpitations | Low birth weight |
| Increased risk of infection | Preterm delivery |
| Cardiac decompensation (severe) | Perinatal death |
| Poor tolerance of hemorrhage at delivery | Neonatal anemia (especially from severe maternal IDA) |
| Increased perioperative risk | Impaired neurodevelopment (iron/folate) |
| Postpartum depression (linked to iron deficiency) | Neural tube defects (folate deficiency) |
Anemia in pregnancy
Anemia in Pregnancy — Summary
Definition (WHO)
- Hb <11 g/dL at any point in pregnancy
- Severe: Hb <7–8 g/dL
1. Physiologic (Dilutional) Anemia
- Plasma volume ↑ 47% vs. RBC mass ↑ only 17% → hemodilution
- Nadir at 28–34 weeks
- MCV and MCHC remain normal (key distinguishing feature from IDA)
- Hb >11 g/dL (1st trimester) or >10 g/dL (2nd/3rd) = physiologic; no treatment needed
2. Iron Deficiency Anemia (IDA) — Most Common
| Feature | Detail |
|---|---|
| Total iron required in pregnancy | ~1130 mg |
| Most common cause | Inadequate pre-pregnancy stores + increased fetal demand |
| Prevalence | 18% (1st trimester) → 29% (3rd trimester) in US women |
| Diagnosis | ↓ Ferritin (best single test; <12 μg/L = IDA, <20 μg/L = depletion) + ↓ Fe, ↑ TIBC, ↓ MCV (late) |
| Fetal effects | LBW, preterm birth, perinatal death, neonatal anemia |
- Prelatent - ↓ ferritin only; Hb normal
- Latent - ↓ serum iron, ↑ TIBC, ↓ transferrin saturation; Hb normal
- Overt IDA - ↓ Hb, eventually ↓ MCV
- Oral iron: 60 mg elemental iron/day (2nd and 3rd trimester) - reduces anemia incidence by up to 73% (Cochrane 2024, PMID 39145520)
- IV iron (iron sucrose, ferric carboxymaltose): for oral failure/intolerance, severe anemia, malabsorption
- Blood transfusion: Hb <7 g/dL or hemodynamic instability
3. Megaloblastic Anemia — Second Most Common
Folate Deficiency
- Requirements increase from 400 → 600 μg/day in pregnancy
- Risk factors: anticonvulsants, alcohol, sulfa drugs, multiple gestation, hemolytic anemia
- Consequences: megaloblastic anemia + neural tube defects (NTDs)
- Prophylaxis: 400–800 μg/day folic acid starting ≥1 month before conception
- High-risk women (prior NTD): 4–5 mg/day
Vitamin B12 Deficiency
- Risk groups: vegans, pernicious anemia, prior gastric surgery, Crohn's disease
- Presents: macrocytic anemia + neurologic symptoms (subacute combined degeneration)
- Treating with folate alone corrects anemia but will not prevent neurologic damage - B12 must be replaced
- Diagnosis: ↓ serum B12, positive anti-intrinsic factor antibody (pernicious anemia)
- Treatment: parenteral cyanocobalamin/hydroxocobalamin
4. Hemolytic Anemias
| Type | Key Points |
|---|---|
| Sickle Cell Disease | Highest risk hemoglobinopathy; vaso-occlusive crises, ACS, preeclampsia; stop hydroxyurea pre-conception; transfusion support |
| Thalassemia | Microcytic picture; β-thalassemia major requires transfusions |
| Hereditary Spherocytosis | Hemolytic crises in pregnancy; EMA flow cytometry for diagnosis; folate supplementation |
| AIHA | Warm (IgG, Rh system) or cold (IgM); positive direct Coombs test; treat with steroids, IVIG |
| Aplastic Anemia | Pancytopenia; rare but serious; transfusion support |
5. Diagnostic Approach
Hb low → Check MCV + ferritin + smear
↓
Microcytic → IDA, thalassemia
Normocytic → Physiologic dilution, hemolysis, blood loss, chronic disease
Macrocytic → Folate/B12 deficiency, hypothyroidism, drug effect
Screening Schedule
- 1st trimester + again at 24–28 weeks (Harrison's 22e)
- Measure ferritin alongside Hb to detect pre-anemic iron depletion
Create a quick reference chart for anemia management in pregnancy
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or missing"
mkdir -p /home/daytona/workspace/anemia-pregnancy-chart
~/anemia-pregnancy-chart/create_chart.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" x 7.5"
pres.title = "Anemia Management in Pregnancy - Quick Reference";
pres.author = "Orris Medical";
// ── COLOUR PALETTE ──────────────────────────────────────────
const C = {
navy: "0D2B55", // dominant dark navy
teal: "1A7A8A", // section headers
mint: "E6F5F7", // light teal bg for rows
gold: "D4A017", // accent / warning
red: "C0392B", // danger / contraindicated
green: "1E7A4A", // safe / treat
white: "FFFFFF",
offwhite: "F4F8FA",
gray: "5A6473",
lightgray: "D9E2EA",
black: "0A0A0A",
};
// ════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE SLIDE
// ════════════════════════════════════════════════════════════════
let s1 = pres.addSlide();
// Full-bleed background
s1.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: C.navy } });
// Decorative accent bar
s1.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.5, h: "100%", fill: { color: C.teal } });
// Red/gold accent stripe
s1.addShape(pres.ShapeType.rect, { x: 0.5, y: 3.4, w: 12.8, h: 0.06, fill: { color: C.gold } });
// Main title
s1.addText("ANEMIA IN PREGNANCY", {
x: 0.8, y: 1.6, w: 11.5, h: 1.0,
fontSize: 44, bold: true, color: C.white,
fontFace: "Calibri", charSpacing: 4, align: "left",
});
// Subtitle
s1.addText("Quick Reference Management Chart", {
x: 0.8, y: 2.65, w: 11.5, h: 0.7,
fontSize: 24, color: C.mint, fontFace: "Calibri", align: "left",
});
// Bottom tag line
s1.addText("WHO Definition: Hb < 11 g/dL | Severe: Hb < 7 g/dL | Screen at 1st trimester & 24–28 weeks", {
x: 0.8, y: 6.7, w: 12, h: 0.5,
fontSize: 13, color: C.lightgray, fontFace: "Calibri", align: "left",
});
// Source tag
s1.addText("Sources: Creasy & Resnik; Harrison's 22e; Goldman-Cecil; Cochrane 2024", {
x: 0.8, y: 7.1, w: 12, h: 0.3,
fontSize: 10, color: C.gray, fontFace: "Calibri", italic: true,
});
// ════════════════════════════════════════════════════════════════
// SLIDE 2 — PHYSIOLOGIC vs PATHOLOGIC OVERVIEW
// ════════════════════════════════════════════════════════════════
let s2 = pres.addSlide();
s2.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: C.offwhite } });
// Header bar
s2.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.75, fill: { color: C.navy } });
s2.addText("OVERVIEW: Physiologic vs Pathologic Anemia", {
x: 0.3, y: 0, w: 12.7, h: 0.75, fontSize: 18, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle",
});
// ── LEFT PANEL: Physiologic ──────────────────────────────────
s2.addShape(pres.ShapeType.roundRect, {
x: 0.3, y: 0.9, w: 5.9, h: 5.9,
fill: { color: C.white }, line: { color: C.teal, width: 2 }, rectRadius: 0.1,
});
s2.addShape(pres.ShapeType.rect, { x: 0.3, y: 0.9, w: 5.9, h: 0.6, fill: { color: C.teal } });
s2.addText("PHYSIOLOGIC (DILUTIONAL)", {
x: 0.35, y: 0.9, w: 5.8, h: 0.6, fontSize: 14, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const physRows = [
["Mechanism", "Plasma vol ↑47% >> RBC mass ↑17%"],
["Peak", "28–34 weeks gestation"],
["Hb lower limit", "≥11 g/dL (1st), ≥10 g/dL (2nd/3rd)"],
["MCV/MCHC", "Normal (key differentiator!)"],
["Treatment", "NONE — physiologic adaptation"],
["Fetal risk", "None if Hb within acceptable range"],
];
physRows.forEach(([label, val], i) => {
const yy = 1.6 + i * 0.75;
const bg = i % 2 === 0 ? C.mint : C.white;
s2.addShape(pres.ShapeType.rect, { x: 0.35, y: yy, w: 5.8, h: 0.68, fill: { color: bg } });
s2.addText(label, {
x: 0.45, y: yy, w: 1.9, h: 0.68, fontSize: 11, bold: true,
color: C.navy, fontFace: "Calibri", valign: "middle",
});
s2.addText(val, {
x: 2.35, y: yy, w: 3.7, h: 0.68, fontSize: 11,
color: C.black, fontFace: "Calibri", valign: "middle",
});
});
// ── RIGHT PANEL: Causes of True Anemia ───────────────────────
s2.addShape(pres.ShapeType.roundRect, {
x: 6.5, y: 0.9, w: 6.5, h: 5.9,
fill: { color: C.white }, line: { color: C.navy, width: 2 }, rectRadius: 0.1,
});
s2.addShape(pres.ShapeType.rect, { x: 6.5, y: 0.9, w: 6.5, h: 0.6, fill: { color: C.navy } });
s2.addText("CAUSES OF TRUE ANEMIA IN PREGNANCY", {
x: 6.55, y: 0.9, w: 6.4, h: 0.6, fontSize: 13, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const causesData = [
[C.red, "Iron Deficiency", "Most common (18–29% of pregnancies)"],
[C.teal, "Folate Deficiency", "2nd most common nutritional cause"],
[C.teal, "Vitamin B12 Deficiency", "Vegans, pernicious anemia, IBD"],
[C.gold, "Sickle Cell Disease", "Highest-risk hemoglobinopathy"],
[C.gold, "Thalassemia", "Microcytic; varies by type"],
[C.gray, "AIHA", "Warm (IgG) or cold (IgM) antibodies"],
[C.gray, "Aplastic Anemia", "Rare; pancytopenia"],
];
causesData.forEach(([dot, label, desc], i) => {
const yy = 1.62 + i * 0.72;
const bg = i % 2 === 0 ? C.mint : C.white;
s2.addShape(pres.ShapeType.rect, { x: 6.55, y: yy, w: 6.4, h: 0.66, fill: { color: bg } });
s2.addShape(pres.ShapeType.ellipse, { x: 6.65, y: yy + 0.2, w: 0.25, h: 0.25, fill: { color: dot } });
s2.addText(label, {
x: 7.0, y: yy, w: 2.2, h: 0.66, fontSize: 11, bold: true,
color: C.navy, fontFace: "Calibri", valign: "middle",
});
s2.addText(desc, {
x: 9.2, y: yy, w: 3.7, h: 0.66, fontSize: 10,
color: C.gray, fontFace: "Calibri", valign: "middle",
});
});
// ════════════════════════════════════════════════════════════════
// SLIDE 3 — IRON DEFICIENCY ANEMIA
// ════════════════════════════════════════════════════════════════
let s3 = pres.addSlide();
s3.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: C.offwhite } });
s3.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.75, fill: { color: C.red } });
s3.addText("IRON DEFICIENCY ANEMIA — Diagnosis & Management", {
x: 0.3, y: 0, w: 12.7, h: 0.75, fontSize: 17, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle",
});
// ── Stages of IDA ─────────────────────────────────────────
s3.addText("STAGES OF IRON DEFICIENCY", {
x: 0.3, y: 0.9, w: 5.7, h: 0.4, fontSize: 13, bold: true,
color: C.navy, fontFace: "Calibri",
});
const stages = [
["Stage 1 — Prelatent", "↓ Ferritin only; Hb NORMAL", C.gold],
["Stage 2 — Latent", "↓ Fe, ↑ TIBC, ↓ Transferrin sat; Hb still NORMAL", C.gold],
["Stage 3 — Overt IDA", "↓ Hb + ↓ MCV (microcytic, hypochromic)", C.red],
];
stages.forEach(([title, desc, color], i) => {
const yy = 1.38 + i * 0.82;
s3.addShape(pres.ShapeType.rect, { x: 0.3, y: yy, w: 0.15, h: 0.65, fill: { color } });
s3.addShape(pres.ShapeType.roundRect, {
x: 0.48, y: yy, w: 5.55, h: 0.65,
fill: { color: C.white }, line: { color: C.lightgray, width: 1 }, rectRadius: 0.05,
});
s3.addText(title, { x: 0.58, y: yy + 0.02, w: 5.3, h: 0.28, fontSize: 11, bold: true, color, fontFace: "Calibri" });
s3.addText(desc, { x: 0.58, y: yy + 0.32, w: 5.3, h: 0.28, fontSize: 10, color: C.black, fontFace: "Calibri" });
});
// ── Diagnostic Tests ─────────────────────────────────────────
s3.addShape(pres.ShapeType.rect, { x: 6.2, y: 0.85, w: 6.8, h: 0.45, fill: { color: C.navy } });
s3.addText("DIAGNOSTIC TESTS", {
x: 6.2, y: 0.85, w: 6.8, h: 0.45, fontSize: 13, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const diagTests = [
["Serum Ferritin", "<12 μg/L = IDA; <20 μg/L = depletion", "Best single test ★"],
["Serum Iron", "Decreased", "Affected by diurnal variation"],
["TIBC", "Increased (rises through pregnancy)", "Inversely relates to iron stores"],
["Transferrin Sat", "<16%", "Fe / TIBC × 100"],
["MCV", "Decreased (late finding)", "Also ↓ in thalassemia"],
["sTfR", "Increased", "Useful if ferritin unreliable (inflammation)"],
["Peripheral Smear", "Microcytic, hypochromic RBCs", "Pencil cells, target cells"],
];
diagTests.forEach(([test, result, note], i) => {
const yy = 1.38 + i * 0.56;
const bg = i % 2 === 0 ? C.mint : C.white;
s3.addShape(pres.ShapeType.rect, { x: 6.2, y: yy, w: 6.8, h: 0.54, fill: { color: bg } });
s3.addText(test, { x: 6.3, y: yy, w: 1.8, h: 0.54, fontSize: 10, bold: true, color: C.navy, fontFace: "Calibri", valign: "middle" });
s3.addText(result, { x: 8.1, y: yy, w: 2.4, h: 0.54, fontSize: 10, color: C.red, fontFace: "Calibri", valign: "middle" });
s3.addText(note, { x: 10.5, y: yy, w: 2.4, h: 0.54, fontSize: 9, color: C.gray, fontFace: "Calibri", valign: "middle", italic: true });
});
// ── Treatment ─────────────────────────────────────────
s3.addShape(pres.ShapeType.rect, { x: 0.3, y: 4.25, w: 5.7, h: 0.45, fill: { color: C.green } });
s3.addText("TREATMENT", {
x: 0.3, y: 4.25, w: 5.7, h: 0.45, fontSize: 13, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const txRows = [
["Oral Iron", "60 mg elemental iron/day (2nd + 3rd tri)", "Ferrous sulfate 325 mg; take with vit C"],
["IV Iron", "Iron sucrose / ferric carboxymaltose", "If oral fails, severe anemia, malabsorption"],
["Transfusion","Packed RBCs (1 unit = +1 g/dL Hb)", "Hb <7 g/dL or haemodynamic instability"],
];
txRows.forEach(([route, dose, indication], i) => {
const yy = 4.78 + i * 0.77;
const bg = i % 2 === 0 ? C.white : C.mint;
s3.addShape(pres.ShapeType.rect, { x: 0.3, y: yy, w: 5.7, h: 0.72, fill: { color: bg }, line: { color: C.lightgray, width: 0.5 } });
s3.addText(route, { x: 0.4, y: yy, w: 1.4, h: 0.72, fontSize: 11, bold: true, color: C.green, fontFace: "Calibri", valign: "middle" });
s3.addText(dose, { x: 1.85, y: yy, w: 2.3, h: 0.72, fontSize: 10, color: C.black, fontFace: "Calibri", valign: "middle" });
s3.addText(indication, { x: 4.15, y: yy, w: 1.75, h: 0.72, fontSize: 9, color: C.gray, fontFace: "Calibri", valign: "middle", italic: true });
});
// ════════════════════════════════════════════════════════════════
// SLIDE 4 — MEGALOBLASTIC ANEMIA (FOLATE + B12)
// ════════════════════════════════════════════════════════════════
let s4 = pres.addSlide();
s4.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: C.offwhite } });
s4.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.75, fill: { color: C.teal } });
s4.addText("MEGALOBLASTIC ANEMIA — Folate & Vitamin B12 Deficiency", {
x: 0.3, y: 0, w: 12.7, h: 0.75, fontSize: 17, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle",
});
// FOLATE section
s4.addShape(pres.ShapeType.rect, { x: 0.3, y: 0.88, w: 6.1, h: 0.5, fill: { color: C.teal } });
s4.addText("FOLATE DEFICIENCY", {
x: 0.3, y: 0.88, w: 6.1, h: 0.5, fontSize: 14, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const folateRows = [
["Daily requirement", "400 μg (non-pregnant) → 600 μg (pregnant)"],
["Why deficient", "Increased erythropoiesis; fetal demand; drugs reducing conjugase (anticonvulsants, sulfa, alcohol, OCP)"],
["Smear/labs", "Macrocytic RBCs; hypersegmented neutrophils; ↓ serum folate (<2.5 ng/mL)"],
["Complications", "Megaloblastic anemia + Neural Tube Defects (NTDs)"],
["Prophylaxis", "0.4–0.8 mg/day folic acid — start ≥1 month BEFORE conception, continue through 1st trimester"],
["High-risk prophylaxis","4–5 mg/day (prior NTD, anticonvulsant use, multiple gestation, haemolytic anaemia)"],
["Treatment", "1–5 mg/day folic acid orally until resolution"],
];
folateRows.forEach(([label, val], i) => {
const yy = 1.46 + i * 0.58;
const bg = i % 2 === 0 ? C.mint : C.white;
s4.addShape(pres.ShapeType.rect, { x: 0.3, y: yy, w: 6.1, h: 0.55, fill: { color: bg } });
s4.addText(label, { x: 0.4, y: yy, w: 1.85, h: 0.55, fontSize: 10, bold: true, color: C.teal, fontFace: "Calibri", valign: "middle" });
s4.addText(val, { x: 2.28, y: yy, w: 4.05, h: 0.55, fontSize: 10, color: C.black, fontFace: "Calibri", valign: "middle", wrap: true });
});
// B12 section
s4.addShape(pres.ShapeType.rect, { x: 6.8, y: 0.88, w: 6.2, h: 0.5, fill: { color: C.navy } });
s4.addText("VITAMIN B12 DEFICIENCY", {
x: 6.8, y: 0.88, w: 6.2, h: 0.5, fontSize: 14, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const b12Rows = [
["Risk groups", "Vegans/vegetarians, pernicious anaemia, Crohn's disease, prior gastric surgery"],
["Clinical features","Macrocytic anemia + neurological symptoms (peripheral neuropathy, posterior column signs)"],
["Critical warning", "⚠ Treating with folate alone corrects anaemia but WILL NOT prevent neurological damage — replace B12!"],
["Diagnosis", "Serum B12 <130 pg/mL; anti-intrinsic factor antibody (positive in pernicious anaemia)"],
["Treatment", "Parenteral cyanocobalamin/hydroxocobalamin (IM); oral high-dose B12 if parenteral unavailable"],
["Fetal risk", "NTDs, impaired neurodevelopment if untreated"],
];
b12Rows.forEach(([label, val], i) => {
const yy = 1.46 + i * 0.66;
const bg = i % 2 === 0 ? C.mint : C.white;
const isWarning = i === 2;
s4.addShape(pres.ShapeType.rect, { x: 6.8, y: yy, w: 6.2, h: 0.62, fill: { color: isWarning ? "#FFF3CD" : bg } });
s4.addText(label, { x: 6.9, y: yy, w: 1.7, h: 0.62, fontSize: 10, bold: true, color: isWarning ? C.red : C.navy, fontFace: "Calibri", valign: "middle" });
s4.addText(val, { x: 8.65, y: yy, w: 4.25, h: 0.62, fontSize: 10, color: isWarning ? C.red : C.black, fontFace: "Calibri", valign: "middle", bold: isWarning, wrap: true });
});
// ════════════════════════════════════════════════════════════════
// SLIDE 5 — HEMOGLOBINOPATHIES & OTHER CAUSES
// ════════════════════════════════════════════════════════════════
let s5 = pres.addSlide();
s5.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: C.offwhite } });
s5.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.75, fill: { color: C.navy } });
s5.addText("HEMOGLOBINOPATHIES & OTHER CAUSES", {
x: 0.3, y: 0, w: 12.7, h: 0.75, fontSize: 17, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle",
});
const hemoData = [
{
title: "SICKLE CELL DISEASE",
color: C.red,
rows: [
["Risk", "Highest-risk hemoglobinopathy in pregnancy"],
["Complications","Vaso-occlusive crises, ACS, stroke, preeclampsia, peripartum cardiomyopathy; FGR, preterm birth"],
["Management", "Multidisciplinary care; prophylactic transfusions; folic acid; aggressive pain Mx; avoid NSAIDs (3rd tri)"],
["Drugs", "Hydroxyurea is TERATOGENIC — discontinue before conception; exchange transfusion for severe cases"],
["Vaccination", "Pneumococcal, meningococcal, Haemophilus influenzae vaccines"],
]
},
{
title: "THALASSEMIA",
color: C.gold,
rows: [
["α-thal trait / β-thal trait", "Microcytic picture; usually tolerated; folic acid supplementation"],
["β-thal major", "Severe anemia; regular transfusions; iron chelation paused in pregnancy"],
["Hb H disease (α-thal)", "Moderate hemolytic anemia; may worsen in pregnancy"],
["Screening", "Hb electrophoresis for all pregnant women with low MCV/MCH"],
]
},
];
hemoData.forEach((section, col) => {
const xBase = col === 0 ? 0.3 : 6.8;
const w = 6.1;
s5.addShape(pres.ShapeType.rect, { x: xBase, y: 0.88, w, h: 0.48, fill: { color: section.color } });
s5.addText(section.title, {
x: xBase, y: 0.88, w, h: 0.48, fontSize: 13, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
section.rows.forEach(([label, val], i) => {
const yy = 1.44 + i * 0.68;
const bg = i % 2 === 0 ? C.mint : C.white;
s5.addShape(pres.ShapeType.rect, { x: xBase, y: yy, w, h: 0.64, fill: { color: bg } });
s5.addText(label, { x: xBase + 0.1, y: yy, w: 2.0, h: 0.64, fontSize: 10, bold: true, color: section.color, fontFace: "Calibri", valign: "middle" });
s5.addText(val, { x: xBase + 2.1, y: yy, w: w - 2.2, h: 0.64, fontSize: 9.5, color: C.black, fontFace: "Calibri", valign: "middle", wrap: true });
});
});
// Bottom row — AIHA + Aplastic
const bottomCauses = [
{
title: "AUTOIMMUNE HEMOLYTIC ANEMIA (AIHA)",
color: C.gray,
rows: [
["Types", "Warm IgG (anti-Rh) → associated with SLE, lymphoma, drugs (penicillin, methyldopa) | Cold IgM (anti-I) → Mycoplasma, EBV"],
["Diagnosis","Positive direct Coombs test; macrocytic/hyperproliferative smear with spherocytes"],
["Treatment","Corticosteroids; blood transfusion; IVIG; rarely splenectomy"],
]
},
{
title: "APLASTIC ANEMIA",
color: C.gray,
rows: [
["Features", "Rare; bone marrow failure; pancytopenia (↓ WBC, ↓ platelets, ↓ Hb)"],
["Management","Transfusion support; cyclosporine; SCT deferred if possible; folic acid"],
["Notes", "Pregnancy itself can trigger or worsen aplastic anemia"],
]
},
];
bottomCauses.forEach((section, col) => {
const xBase = col === 0 ? 0.3 : 6.8;
const w = 6.1;
const yStart = 5.1;
s5.addShape(pres.ShapeType.rect, { x: xBase, y: yStart, w, h: 0.38, fill: { color: section.color } });
s5.addText(section.title, {
x: xBase, y: yStart, w, h: 0.38, fontSize: 11, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
section.rows.forEach(([label, val], i) => {
const yy = yStart + 0.42 + i * 0.52;
const bg = i % 2 === 0 ? C.mint : C.white;
s5.addShape(pres.ShapeType.rect, { x: xBase, y: yy, w, h: 0.48, fill: { color: bg } });
s5.addText(label, { x: xBase + 0.1, y: yy, w: 1.5, h: 0.48, fontSize: 9.5, bold: true, color: C.gray, fontFace: "Calibri", valign: "middle" });
s5.addText(val, { x: xBase + 1.6, y: yy, w: w - 1.7, h: 0.48, fontSize: 9, color: C.black, fontFace: "Calibri", valign: "middle", wrap: true });
});
});
// ════════════════════════════════════════════════════════════════
// SLIDE 6 — DIAGNOSTIC ALGORITHM + REFERENCE RANGES
// ════════════════════════════════════════════════════════════════
let s6 = pres.addSlide();
s6.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: C.offwhite } });
s6.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.75, fill: { color: C.teal } });
s6.addText("DIAGNOSTIC ALGORITHM & LABORATORY REFERENCE RANGES", {
x: 0.3, y: 0, w: 12.7, h: 0.75, fontSize: 17, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle",
});
// Algorithm boxes
const algoX = 0.3;
s6.addShape(pres.ShapeType.roundRect, { x: algoX, y: 0.9, w: 5.5, h: 0.6, fill: { color: C.navy }, rectRadius: 0.1 });
s6.addText("Hb < 11 g/dL (1st tri) or < 10 g/dL (2nd/3rd tri)", {
x: algoX, y: 0.9, w: 5.5, h: 0.6, fontSize: 11, bold: true,
color: C.white, fontFace: "Calibri", align: "center", valign: "middle",
});
// Arrow down
s6.addShape(pres.ShapeType.rect, { x: algoX + 2.65, y: 1.54, w: 0.2, h: 0.3, fill: { color: C.navy } });
s6.addShape(pres.ShapeType.roundRect, { x: algoX, y: 1.86, w: 5.5, h: 0.55, fill: { color: C.teal }, rectRadius: 0.1 });
s6.addText("Check: MCV + Ferritin + Peripheral Smear + Reticulocyte count", {
x: algoX, y: 1.86, w: 5.5, h: 0.55, fontSize: 10, bold: true,
color: C.white, fontFace: "Calibri", align: "center", valign: "middle",
});
// Arrow down
s6.addShape(pres.ShapeType.rect, { x: algoX + 2.65, y: 2.44, w: 0.2, h: 0.25, fill: { color: C.teal } });
// Three branches
const branches = [
{ x: 0.3, label: "MICROCYTIC\n(↓ MCV)", sub: "IDA (check ferritin)\nThalassemia\nSideroblastic anemia", color: C.red },
{ x: 2.2, label: "NORMOCYTIC\n(normal MCV)", sub: "Physiologic dilution\nBlood loss / Hemolysis\nAnemia of chronic disease", color: C.teal },
{ x: 4.05, label: "MACROCYTIC\n(↑ MCV)", sub: "Folate deficiency\nVit B12 deficiency\nHypothyroidism / drugs", color: C.gold },
];
// horizontal bar
s6.addShape(pres.ShapeType.rect, { x: 0.3, y: 2.68, w: 5.5, h: 0.07, fill: { color: C.lightgray } });
branches.forEach(({ x, label, sub, color }) => {
s6.addShape(pres.ShapeType.rect, { x: x, y: 2.68, w: 0.07, h: 0.3, fill: { color: C.lightgray } });
s6.addShape(pres.ShapeType.roundRect, { x: x - 0.1, y: 3.0, w: 1.75, h: 0.75, fill: { color }, rectRadius: 0.1 });
s6.addText(label, {
x: x - 0.08, y: 3.0, w: 1.72, h: 0.75, fontSize: 10, bold: true,
color: C.white, fontFace: "Calibri", align: "center", valign: "middle",
});
s6.addShape(pres.ShapeType.roundRect, {
x: x - 0.1, y: 3.78, w: 1.75, h: 1.05,
fill: { color: C.white }, line: { color, width: 1.5 }, rectRadius: 0.05,
});
s6.addText(sub, {
x: x, y: 3.82, w: 1.55, h: 0.98, fontSize: 9, color: C.black,
fontFace: "Calibri", align: "left", valign: "top",
bullet: true,
});
});
// Additional test note
s6.addText("Also check: Hb electrophoresis (all women), Direct Coombs (if hemolysis), Anti-IF antibody (if pernicious anemia suspected)", {
x: 0.3, y: 4.93, w: 5.5, h: 0.55, fontSize: 9.5, color: C.gray,
fontFace: "Calibri", italic: true,
});
// ── Reference ranges table ──────────────────────────
s6.addShape(pres.ShapeType.rect, { x: 6.2, y: 0.88, w: 6.8, h: 0.48, fill: { color: C.navy } });
s6.addText("LABORATORY REFERENCE RANGES IN PREGNANCY (Creasy & Resnik)", {
x: 6.2, y: 0.88, w: 6.8, h: 0.48, fontSize: 11, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const labs = [
["Test", "1st Trimester", "2nd Trimester", "3rd Trimester"],
["Hb (g/dL)", "≥11.0", "≥10.0", "≥10.0"],
["MCV (μm³)", "81–96", "82–97", "81–99"],
["MCHC (g/dL)", "32–35", "32–35", "32–35"],
["Ferritin (μg/L)", ">20 (1st)", "Declines", "May be low"],
["Serum Iron (μg/dL)","72–143", "44–178", "30–193"],
["TIBC (μg/dL)", "235–408", "302–519", "580–597"],
["Transferrin Sat", "16–60%", "16–60%", "16–60%"],
["Serum Folate", "26–150 μg/L", "8–240 μg/L", "14–207 μg/L"],
["Serum B12 (pg/mL)","118–438", "130–656", "99–526"],
["Reticulocytes", "0.5–1.5%", "0.5–1.5%", "0.5–1.5%"],
];
labs.forEach((row, i) => {
const yy = 1.44 + i * 0.52;
const isHeader = i === 0;
const bg = isHeader ? C.teal : (i % 2 === 0 ? C.mint : C.white);
const textColor = isHeader ? C.white : C.black;
const fw = isHeader;
s6.addShape(pres.ShapeType.rect, { x: 6.2, y: yy, w: 6.8, h: 0.5, fill: { color: bg } });
const cols = [1.9, 1.55, 1.65, 1.6];
const xs = [6.25, 8.15, 9.7, 11.35];
row.forEach((cell, ci) => {
s6.addText(cell, {
x: xs[ci], y: yy, w: cols[ci], h: 0.5, fontSize: isHeader ? 10 : 9.5,
bold: fw, color: textColor, fontFace: "Calibri", valign: "middle",
});
});
});
// ════════════════════════════════════════════════════════════════
// SLIDE 7 — OUTCOMES + CONTRAINDICATED DRUGS + SCREENING
// ════════════════════════════════════════════════════════════════
let s7 = pres.addSlide();
s7.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: C.offwhite } });
s7.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.75, fill: { color: C.navy } });
s7.addText("OUTCOMES, DRUG SAFETY & SCREENING", {
x: 0.3, y: 0, w: 12.7, h: 0.75, fontSize: 17, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle",
});
// Maternal outcomes
s7.addShape(pres.ShapeType.rect, { x: 0.3, y: 0.88, w: 4.0, h: 0.48, fill: { color: C.red } });
s7.addText("MATERNAL OUTCOMES", {
x: 0.3, y: 0.88, w: 4.0, h: 0.48, fontSize: 12, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const maternalOutcomes = [
"Fatigue, dyspnea, palpitations",
"Increased susceptibility to infection",
"Cardiac decompensation (severe anemia)",
"Reduced tolerance to peripartum hemorrhage",
"Higher perioperative risk",
"Postpartum depression (linked to IDA)",
];
s7.addText(maternalOutcomes.map(t => ({ text: t, options: { bullet: true, breakLine: true } })), {
x: 0.35, y: 1.4, w: 3.9, h: 3.0, fontSize: 10, color: C.black, fontFace: "Calibri",
});
// Fetal outcomes
s7.addShape(pres.ShapeType.rect, { x: 4.6, y: 0.88, w: 4.0, h: 0.48, fill: { color: C.gold } });
s7.addText("FETAL / NEONATAL OUTCOMES", {
x: 4.6, y: 0.88, w: 4.0, h: 0.48, fontSize: 12, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const fetalOutcomes = [
"Low birth weight (LBW)",
"Preterm delivery",
"Perinatal death",
"Neonatal anemia (especially severe maternal IDA)",
"Neural tube defects (folate deficiency)",
"Impaired neurodevelopment (iron/folate/B12)",
];
s7.addText(fetalOutcomes.map(t => ({ text: t, options: { bullet: true, breakLine: true } })), {
x: 4.65, y: 1.4, w: 3.9, h: 3.0, fontSize: 10, color: C.black, fontFace: "Calibri",
});
// Drug safety + screening
s7.addShape(pres.ShapeType.rect, { x: 9.0, y: 0.88, w: 4.0, h: 0.48, fill: { color: C.navy } });
s7.addText("DRUG SAFETY & SCREENING", {
x: 9.0, y: 0.88, w: 4.0, h: 0.48, fontSize: 12, bold: true,
color: C.white, fontFace: "Calibri", valign: "middle", align: "center",
});
const drugItems = [
{ drug: "Ferrous sulfate", safety: "SAFE", note: "1st-line oral iron" },
{ drug: "Ferric carboxymaltose", safety: "SAFE (2nd/3rd)","note: IV iron; avoid 1st trimester" },
{ drug: "Folic acid 0.4–0.8 mg", safety: "SAFE", note: "Periconceptional" },
{ drug: "Cyanocobalamin (B12 IM)", safety: "SAFE", note: "For pernicious anemia" },
{ drug: "Hydroxyurea", safety: "TERATOGENIC", note: "Stop before conception" },
{ drug: "Methotrexate", safety: "CONTRAIND.", note: "Folate antagonist" },
{ drug: "Iron chelators", safety: "AVOID", note: "Deferoxamine: limited data; pause in pregnancy" },
];
drugItems.forEach(({ drug, safety, note }, i) => {
const yy = 1.44 + i * 0.58;
const bg = i % 2 === 0 ? C.mint : C.white;
const safetyColor = safety === "SAFE" ? C.green : safety.includes("SAFE") ? C.teal : C.red;
s7.addShape(pres.ShapeType.rect, { x: 9.0, y: yy, w: 4.0, h: 0.54, fill: { color: bg } });
s7.addText(drug, { x: 9.05, y: yy, w: 2.0, h: 0.54, fontSize: 9.5, bold: true, color: C.navy, fontFace: "Calibri", valign: "middle" });
s7.addText(safety, { x: 11.0, y: yy, w: 1.0, h: 0.54, fontSize: 9, bold: true, color: safetyColor, fontFace: "Calibri", valign: "middle", align: "center" });
s7.addText(note, { x: 11.95, y: yy, w: 0.9, h: 0.54, fontSize: 8, italic: true, color: C.gray, fontFace: "Calibri", valign: "middle" });
});
// Screening box
s7.addShape(pres.ShapeType.roundRect, {
x: 0.3, y: 4.55, w: 12.7, h: 1.1,
fill: { color: C.navy }, rectRadius: 0.1,
});
s7.addText([
{ text: "SCREENING PROTOCOL: ", options: { bold: true, color: C.gold } },
{ text: "Check Hb at 1st trimester booking visit ", options: { color: C.white } },
{ text: "| ", options: { color: C.lightgray } },
{ text: "Repeat at 24–28 weeks ", options: { color: C.white } },
{ text: "| ", options: { color: C.lightgray } },
{ text: "Hb electrophoresis for ALL women ", options: { color: C.white } },
{ text: "| ", options: { color: C.lightgray } },
{ text: "Measure ferritin alongside Hb to detect pre-anaemic iron depletion", options: { color: C.mint } },
], {
x: 0.5, y: 4.58, w: 12.4, h: 0.55, fontSize: 11, fontFace: "Calibri", valign: "middle",
});
s7.addText("Sources: Creasy & Resnik's MFM; Harrison's 22e (2025); Goldman-Cecil; Cochrane 2024 (PMID 39145520, 38189492) | WHO / ACOG / NICE guidelines", {
x: 0.5, y: 5.1, w: 12.4, h: 0.45, fontSize: 9, color: C.lightgray,
fontFace: "Calibri", italic: true, valign: "middle",
});
// SAVE
pres.writeFile({ fileName: "/home/daytona/workspace/anemia-pregnancy-chart/Anemia_in_Pregnancy_Quick_Reference.pptx" });
console.log("DONE");
cd /home/daytona/workspace/anemia-pregnancy-chart && node create_chart.js 2>&1
~/anemia-pregnancy-chart/create_chart.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/anemia-pregnancy-chart/create_chart.js'
cd /home/daytona/workspace/anemia-pregnancy-chart && node create_chart.js 2>&1
ls -lh /home/daytona/workspace/anemia-pregnancy-chart/
Anemia in Pregnancy Quick Reference
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide - bold navy/teal theme with WHO definition |
| 2 | Overview - Physiologic vs Pathologic anemia side-by-side comparison |
| 3 | Iron Deficiency Anemia - 3 stages, diagnostic tests table, treatment ladder (oral → IV → transfusion) |
| 4 | Megaloblastic Anemia - Folate vs B12 deficiency with a highlighted warning about B12 neurologic damage |
| 5 | Hemoglobinopathies & Other Causes - Sickle cell, thalassemia, AIHA, aplastic anemia |
| 6 | Diagnostic Algorithm - MCV-based flowchart + trimester-specific lab reference ranges |
| 7 | Outcomes, Drug Safety & Screening - Maternal/fetal consequences, drug safety table (safe vs teratogenic), screening protocol |
Other extragenital disorders (medical, surgical illnesses)complicating pregnancies
Extragenital (Medical & Surgical) Disorders Complicating Pregnancy
I. CARDIOVASCULAR DISORDERS
- Complicates 1-4% of pregnancies; leading cause of indirect maternal mortality (37% of non-obstetric deaths, UK)
- Plasma volume ↑40-50%, cardiac output ↑30-50%, HR ↑15-20 bpm → exacerbates any underlying disease
- Hypertension: complicates ~10% of pregnancies; first-line drugs: labetalol, nifedipine, methyldopa; ACE inhibitors and ARBs are contraindicated
- Peripartum cardiomyopathy (PPCM): LV dysfunction in last month or within 5 months postpartum; treated with standard HF therapy (adapted for pregnancy/lactation); bromocriptine may accelerate recovery
- Congenital heart disease: most common etiology in the developed world; management depends on lesion type; WHO Class IV conditions (PAH, EF <30%, severe AS, Fontan complications) contraindicate pregnancy
- Valvular disease: mitral stenosis most dangerous; regurgitant lesions generally better tolerated
II. DIABETES MELLITUS
Types in Pregnancy
- Type 1 DM (T1DM) - pre-existing
- Type 2 DM (T2DM) - pre-existing (increasingly common with obesity epidemic)
- Gestational Diabetes Mellitus (GDM) - glucose intolerance first recognized in pregnancy
Physiologic Basis
- Human placental lactogen (hPL), progesterone, cortisol, and prolactin are counter-regulatory hormones that cause progressive insulin resistance (peaks 3rd trimester: 50-60% reduction in insulin sensitivity)
- Normal beta cells compensate with increased insulin secretion
- GDM occurs when beta cell reserve is insufficient to overcome insulin resistance (shifted down on the DI curve)
- Insulin requirements increase from 0.7-0.8 units/kg (1st trimester) → 0.9-1.2 units/kg (3rd trimester) in T1DM
Screening and Diagnosis (GDM - 8% of pregnancies)
- 50-g glucose challenge test (GCT) → glucose at 60 min; threshold: >7.2 mmol/L (130 mg/dL)
- If positive → 100-g oral GTT (fasting + 1h, 2h, 3h); 2 elevated values = GDM
| Time | Plasma Glucose |
|---|---|
| Fasting | <5.3 mmol/L (<95 mg/dL) |
| 1 hour | <10.0 mmol/L (<180 mg/dL) |
| 2 hours | <8.6 mmol/L (<155 mg/dL) |
| 3 hours | <7.8 mmol/L (<140 mg/dL) |
Maternal Complications of Pregestational Diabetes
- Hypertension (OR 14.2), preeclampsia (OR 3.4)
- Cesarean delivery (OR 11.3), preterm birth (OR 4.4)
- Retinopathy worsening (especially with duration >10 years, poor pre-pregnancy HbA1c; rapid normalization can transiently worsen retinopathy)
- Nephropathy progression
- Hypoglycemia unawareness
- Ketoacidosis (especially T1DM)
- Maternal mortality 60/100,000 pregnancies (vs 7-12/100,000 general population)
Fetal Complications
- Macrosomia (large for gestational age) → shoulder dystocia, birth trauma
- Congenital malformations (cardiac, neural tube, skeletal - risk proportional to 1st trimester HbA1c)
- Intrauterine growth restriction (with vasculopathy)
- Polyhydramnios
- Neonatal hypoglycemia (fetal hyperinsulinism)
- Neonatal respiratory distress syndrome
- Stillbirth (3-4x increased risk with poor control)
- Offspring at lifelong increased risk of obesity, T2DM
Management
- Target HbA1c <6% before conception to minimize congenital malformation risk
- Ophthalmologic, renal, cardiac evaluation
- Stop teratogenic drugs (ACE-I, statins, metformin - safety debated)
- Insulin is the preferred drug in pregnancy - best safety profile, lowest treatment failure
| Measurement | Target |
|---|---|
| Fasting | <5.3 mmol/L (<95 mg/dL) |
| 1-hour postprandial | <7.8 mmol/L (<140 mg/dL) |
| 2-hour postprandial | <6.7 mmol/L (<120 mg/dL) |
- HbA1c is unreliable in pregnancy (accelerated RBC turnover gives falsely low values) - use daily glucose monitoring and continuous glucose monitoring (CGM) instead
- Insulin dose: basal-bolus regimen or insulin pump (CSII); CSII significantly reduces retinopathy progression
- GDM: start with dietary/nutritional therapy; if targets not met → insulin (first-line) or metformin (acceptable per some guidelines)
- Fetal surveillance: growth ultrasounds, biophysical profile, Doppler
- Induction of labor: 37-39 weeks (early term)
- Cesarean: reserved for estimated fetal weight ≥4500 g (macrosomia) or obstetric indications
III. THYROID DISORDERS
Physiologic Changes in Pregnancy
- hCG (structurally similar to TSH) stimulates thyroid → transient ↑ free T4, ↓ TSH in 1st trimester (especially weeks 8-14)
- Thyroxine-binding globulin (TBG) increases (↑ estrogen) → total T4/T3 increased, but free levels change less
- Iodine requirement increases; renal iodine clearance increases
Hypothyroidism in Pregnancy
- Prevalence: 2-3% (overt); 2-5% (subclinical)
- Most common cause: Hashimoto's thyroiditis (autoimmune)
- Risks of untreated hypothyroidism: miscarriage, preterm birth, preeclampsia, placental abruption, LBW, impaired fetal neurodevelopment (fetus depends on maternal T4 in 1st trimester)
- TSH target in pregnancy: 0.1-2.5 mIU/L (1st trimester); 0.2-3.0 mIU/L (2nd/3rd trimester)
- Treatment: levothyroxine - dose usually increases by 25-50% in pregnancy; check TSH every 4 weeks in 1st half, then every 4-6 weeks thereafter
- Screen: TSH at booking in high-risk women (history of thyroid disease, family history, symptoms, goiter, type 1 DM, prior radiation)
Hyperthyroidism in Pregnancy
- Prevalence: ~0.1-0.4%; most common cause: Graves' disease
- Distinguish from physiologic hCG-mediated TSH suppression (gestational transient thyrotoxicosis)
- Risks: miscarriage, preterm birth, FGR, stillbirth, neonatal hyperthyroidism (from maternal TSH receptor antibodies crossing placenta), thyroid storm (life-threatening)
- Treatment:
- Propylthiouracil (PTU): preferred in 1st trimester (crosses placenta less; methimazole associated with aplasia cutis/choanal atresia in 1st trimester)
- Methimazole/carbimazole: preferred in 2nd and 3rd trimesters (PTU associated with hepatotoxicity)
- Target: maintain maternal free T4 at upper normal range (minimizes fetal hypothyroidism)
- Radioiodine: absolutely contraindicated in pregnancy
- Beta-blockers (propranolol): short-term for symptomatic control
- Thyroidectomy: 2nd trimester if drug failure
Postpartum Thyroiditis
- Autoimmune; occurs in 5-10% of women postpartum
- Triphasic: thyrotoxicosis (1-4 months) → hypothyroidism (4-8 months) → resolution (most cases)
- May be permanent hypothyroidism in 25%
IV. RENAL AND URINARY DISORDERS
Physiologic Changes
- GFR increases by 50% by end of 1st trimester (due to ↑ cardiac output, ↑ renal plasma flow)
- Serum creatinine normally falls to 0.4-0.8 mg/dL (normal non-pregnant levels of 0.9-1.0 mg/dL may indicate significant renal impairment in pregnancy)
- Glucosuria can occur with normal glucose (tubular reabsorption cannot keep up with filtered load)
- Physiologic hydronephrosis (right > left) from uterine compression
Urinary Tract Infections (UTI)
- Most common bacterial complication of pregnancy
- Asymptomatic bacteriuria (ASB): 2-7% of pregnant women; higher risk of progression to pyelonephritis (20-30% if untreated vs <1% in non-pregnant)
- Universal screening for ASB by urine culture at first prenatal visit is recommended
- Treatment of ASB: 7-14 days nitrofurantoin, cephalexin, or amoxicillin (avoid nitrofurantoin at term - neonatal hemolysis; avoid trimethoprim in 1st trimester - folate antagonist; avoid fluoroquinolones)
- Pyelonephritis: most common cause of non-obstetric hospitalization in pregnancy; IV ceftriaxone or ampicillin + gentamicin; risk of preterm labor, septic shock, ARDS
Chronic Kidney Disease (CKD) in Pregnancy
- Outcomes depend on degree of renal impairment and hypertension
- Creatinine <125 μmol/L: pregnancy generally tolerated
- Creatinine >180 μmol/L: significant risk of accelerated renal decline, preeclampsia (50%), FGR, preterm birth
- Proteinuria worsens in pregnancy (increased GFR + altered tubular function)
- Monitor BP closely; target <140/90 mmHg
- ACE inhibitors/ARBs must be stopped - switch to labetalol, methyldopa, nifedipine
- Dialysis patients: conception is rare; if pregnant, increase dialysis to >36 hours/week
Nephrolithiasis
- Occurs in 1:200-1:1500 pregnancies; most common in 2nd/3rd trimester
- Increased urinary calcium excretion (↑ intestinal absorption, ↑ GFR)
- Presents: renal/ureteric colic, hematuria
- 70-80% pass spontaneously
- Diagnosis: renal ultrasound first; MRI if needed (avoid CT radiation if possible)
- Management: IV fluids, analgesia (opioids safe; NSAIDs avoid after 20 weeks); urological intervention if obstruction/sepsis
V. RESPIRATORY DISORDERS
Asthma
- Most common obstructive lung disease in pregnancy (~8%)
- Rule of thirds: 1/3 improve, 1/3 unchanged, 1/3 worsen during pregnancy
- Risks of uncontrolled asthma: preeclampsia, preterm birth, FGR, low birth weight, neonatal mortality
- Risks of asthma medications in pregnancy are less than the risk of uncontrolled asthma to mother and fetus
- Treatment:
- Inhaled beta-2 agonists (salbutamol/albuterol): safe; continue
- Inhaled corticosteroids (budesonide preferred): safe; continue
- Oral corticosteroids: use if needed; associated with cleft palate (1st trimester) and preeclampsia at high doses but benefits outweigh risks in severe exacerbations
- Leukotriene receptor antagonists (montelukast): acceptable to continue if already on it
- Systemic steroids for acute severe exacerbation: do not withhold
- Avoid aspirin and NSAIDs in aspirin-sensitive asthmatic patients
- Monitor with peak flow/spirometry; avoid known triggers
Pneumonia
- Most common cause: Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae
- Influenza (H1N1) disproportionately severe in pregnancy (higher mortality, especially with underlying asthma, diabetes, hypertension, renal disease); vaccinate all pregnant women
- Varicella pneumonia: rare but severe (mortality 40% if untreated); treat with IV acyclovir
- Management: hospitalize readily; empirical beta-lactam + macrolide; adjust for gestation
Pulmonary Embolism (PE) and DVT
- Pregnancy is a hypercoagulable state: ↑ factors II, VII, VIII, IX, X, XII, fibrinogen, vWF; ↓ protein S, antithrombin III; venous stasis; endothelial injury
- DVT/PE complicates ~1 in 500 pregnancies; highest risk postpartum
- Diagnosis: compression ultrasound for DVT; V/Q scan or CTPA for PE (both acceptable in pregnancy)
- Treatment: LMWH throughout pregnancy (does not cross placenta; preferred over UFH); warfarin contraindicated (teratogenic in 1st trimester; fetal hemorrhage); NOACs contraindicated
- Inherited thrombophilias (Factor V Leiden, prothrombin gene mutation) and antiphospholipid syndrome increase risk significantly
VI. GASTROINTESTINAL AND LIVER DISORDERS
Nausea and Vomiting / Hyperemesis Gravidarum
- Nausea in 70-80% of pregnancies; vomiting in 50%
- Hyperemesis gravidarum (HG): persistent vomiting with weight loss >5%, dehydration, ketonuria; requires hospitalization
- Pathogenesis: hCG stimulates CTZ; elevated in multiple pregnancy, molar pregnancy, Down syndrome
- Management: IV fluid replacement, antiemetics (ondansetron, metoclopramide, prochlorperazine), thiamine (B1) supplementation (prevent Wernicke encephalopathy), pyridoxine (B6) + doxylamine (first-line combination), nasogastric/parenteral nutrition if severe
Gastroesophageal Reflux Disease (GERD)
- Very common (40-80%); due to ↑ progesterone → lower esophageal sphincter relaxation + mechanical upward displacement of stomach
- Management: antacids, H2 blockers (safe), PPIs (safe if needed); lifestyle modification
Appendicitis
- Most common non-obstetric surgical emergency in pregnancy (1:500-1:1500)
- The appendix migrates upward and laterally as the uterus enlarges - pain is NOT in the classic RIF in later pregnancy (may be RUQ or right flank)
- Diagnosis is more difficult - nausea/vomiting are physiologic; white cell count rises normally in pregnancy; imaging: ultrasound first, then MRI (preferred over CT to avoid radiation)
- Perforation risk is higher if diagnosis delayed (perforation → peritonitis → preterm labor, fetal loss)
- Treatment: prompt appendectomy regardless of gestational age; laparoscopic approach safe in 1st/2nd trimester; avoid delays
Acute Cholecystitis and Cholelithiasis
- Pregnancy increases cholesterol secretion and gallbladder stasis → increased gallstone formation
- Second most common non-obstetric surgical emergency in pregnancy
- Management: initial conservative (IV fluids, antibiotics, analgesia); cholecystectomy in 2nd trimester if conservative management fails or for recurrence; ERCP safe for choledocholithiasis
Inflammatory Bowel Disease (IBD)
- Crohn's disease and ulcerative colitis: flares in pregnancy affect outcomes (preterm birth, FGR)
- Active disease at conception has worse outcomes than quiescent disease
- Medications:
- 5-aminosalicylates (mesalazine): safe
- Corticosteroids: safe for acute flares
- Azathioprine/6-mercaptopurine: generally continued (risks of flare > teratogenicity)
- Anti-TNF agents (infliximab, adalimumab): generally safe through 2nd trimester; discontinue in 3rd trimester to avoid neonatal immunosuppression (but case-by-case)
- Methotrexate: contraindicated - folate antagonist, teratogenic
- Thalidomide: absolutely contraindicated
Liver Diseases Specific to Pregnancy
| Condition | Trimester | Key Features | Management |
|---|---|---|---|
| Intrahepatic cholestasis of pregnancy (ICP) | 3rd | Pruritus (especially palms/soles), ↑ bile acids, ↑ transaminases, jaundice rare | Ursodeoxycholic acid; early delivery at 37 weeks; risk of stillbirth |
| Acute fatty liver of pregnancy (AFLP) | 3rd | Malaise, N/V, RUQ pain, jaundice, ↓ glucose, ↑ PT, encephalopathy; HELLP overlap | Emergent delivery is treatment; ICU support |
| HELLP syndrome | 2nd/3rd | Hemolysis + elevated liver enzymes + low platelets; RUQ/epigastric pain | Delivery; steroids for platelet augmentation |
| Budd-Chiari syndrome | Rare | Thrombosis of hepatic veins; pregnancy is a thrombotic state | Anticoagulation; TIPS if severe |
VII. NEUROLOGICAL DISORDERS
Epilepsy and Seizure Disorders
- Affects ~0.5% of pregnancies
- Pregnancy effects on epilepsy: altered antiepileptic drug (AED) pharmacokinetics (increased volume of distribution, altered protein binding, increased renal clearance) → drug levels may fall → breakthrough seizures
- Uncontrolled seizures are more dangerous to mother and fetus than most AEDs
| Drug | Risk |
|---|---|
| Valproate | Highest risk - neural tube defects (1-2%), cognitive impairment, polydactyly; avoid if possible |
| Carbamazepine | Neural tube defects (0.5-1%); relatively safer than valproate |
| Phenytoin | Fetal hydantoin syndrome (craniofacial, digital abnormalities) |
| Lamotrigine | Relatively safest (oral cleft, low risk); dose must be increased in pregnancy |
| Levetiracetam | Relatively safe; increasing use |
- Folic acid 5 mg/day (high dose) for all women with epilepsy on AEDs from pre-conception
- Monitor AED levels through pregnancy; adjust doses accordingly
- Vitamin K 10 mg/day to mother from 36 weeks (AEDs induce enzyme degradation of clotting factors)
- Neonatal: IV vitamin K at birth
Migraine
- Usually improves in pregnancy (especially those with menstrual migraine - due to stable estrogen)
- Acute treatment: paracetamol (acetaminophen) (safe); codeine (short-term); aspirin/NSAIDs (avoid 3rd trimester); triptans (limited data - use with caution if needed)
- Avoid ergotamine (causes uterine vasoconstriction - contraindicated)
- Prophylaxis: beta-blockers (propranolol); amitriptyline; avoid valproate, topiramate (teratogenic)
Stroke in Pregnancy
- Risk is increased: hypercoagulable state, venous stasis, cerebral vein thrombosis
- Ischemic stroke: IV tPA can be given in pregnancy if clinically indicated (though data limited); thrombus may be considered
- Cerebral vein thrombosis: anticoagulate with LMWH
- Subarachnoid hemorrhage (SAH): aneurysmal rupture risk increases; treat definitively (coiling preferred to clipping in pregnancy)
VIII. AUTOIMMUNE AND RHEUMATOLOGIC DISORDERS
Systemic Lupus Erythematosus (SLE)
- Predominantly affects women of childbearing age
- Pregnancy can trigger lupus flares (immunologic and hormonal changes)
- Clinically significant kidney disease in ~30% of women with SLE
- Poor pregnancy outcomes: miscarriage, preterm birth, FGR, stillbirth, neonatal lupus (anti-Ro/La antibodies)
- Antiphospholipid syndrome (APS): thrombosis, recurrent pregnancy loss; treat with LMWH + low-dose aspirin in pregnancy
- Predictors of poor pregnancy outcomes: active nephritis, hypertension, antiphospholipid antibodies, thrombocytopenia, anti-Ro/SS-A antibodies (neonatal complete heart block risk)
- Safe drugs in pregnancy: hydroxychloroquine (continue - protective against flares), azathioprine, low-dose prednisolone, LMWH, low-dose aspirin
- Avoid: cyclophosphamide (teratogenic), mycophenolate (teratogenic), methotrexate
Rheumatoid Arthritis (RA)
- Often improves dramatically during pregnancy (due to immune tolerance mechanisms)
- Postpartum flares are common (within 3 months)
- Safe drugs: hydroxychloroquine, sulfasalazine, low-dose prednisolone; some anti-TNF agents (stop in 3rd trimester)
- Avoid: methotrexate, leflunomide (teratogenic)
IX. HEMATOLOGIC DISORDERS
Thrombocytopenia in Pregnancy
- Occurs in 5-10% of pregnancies
- Gestational thrombocytopenia (most common, benign): mild, no treatment, resolves postpartum; platelets typically >80-100 × 10⁹/L
- ITP (Immune thrombocytopenic purpura): IgG antiplatelet antibodies cross placenta → neonatal thrombocytopenia; treat mother with steroids/IVIG if platelets <30 × 10⁹/L or bleeding; splenectomy (2nd trimester if refractory)
- Preeclampsia/HELLP: platelet consumption; delivery is treatment
- TTP (Thrombotic thrombocytopenic purpura): ADAMTS13 deficiency; microangiopathic hemolysis; plasma exchange is treatment
- Platelets <100 × 10⁹/L → unlikely to be gestational thrombocytopenia; investigate further
VTE and Thrombophilias (see Pulmonary section above)
Sickle Cell Disease and Thalassemia (see Anemia section)
X. INFECTIOUS DISEASES COMPLICATING PREGNANCY
TORCH Infections
| Pathogen | Fetal Effects | Management |
|---|---|---|
| Toxoplasma gondii | Chorioretinitis, hydrocephalus, intracranial calcifications | Spiramycin (early); pyrimethamine + sulfadiazine (confirmed fetal infection); avoid undercooked meat, cat litter |
| Rubella | Congenital rubella syndrome (cataracts, heart defects, deafness, microcephaly) | Vaccination pre-conception; no treatment in pregnancy |
| CMV | Sensorineural hearing loss, microcephaly, chorioretinitis | No proven treatment; valganciclovir under investigation |
| Herpes simplex (HSV) | Neonatal herpes (encephalitis, disseminated) if primary infection at delivery | Acyclovir suppression from 36 weeks if recurrent HSV; cesarean if active lesions at delivery |
| Varicella-zoster | Fetal varicella syndrome (<20 weeks); neonatal varicella if peripartum | VZIG to exposed non-immune women; oral acyclovir for mild disease; IV acyclovir for severe/pneumonia |
Other Key Infections
- Listeria monocytogenes: foodborne (deli meats, soft cheese); flu-like illness → bacteremia, stillbirth, neonatal meningitis; treat with ampicillin + gentamicin
- Group B Streptococcus (GBS): universal screening at 35-37 weeks; intrapartum IV penicillin prophylaxis if positive
- HIV: antiretroviral therapy (ART) throughout pregnancy; target undetectable viral load; HAART reduces MTCT to <1%; elective cesarean if VL >400 copies/mL; avoid breastfeeding (in resource-rich settings)
- Syphilis: universal screening at booking; benzathine penicillin G (crosses placenta); prevents congenital syphilis
- Malaria: P. falciparum causes severe disease in pregnancy (cerebral malaria, hypoglycemia, severe anemia, placental infection → FGR, preterm birth); chloroquine (safe); artemisinin-based combinations (2nd/3rd trimester); avoid primaquine (hemolysis)
- COVID-19: pregnant women at higher risk of ICU admission, preterm birth; vaccinate; monitor closely
XI. SURGICAL CONDITIONS IN PREGNANCY
General Principles for Surgery in Pregnancy
- 2nd trimester is the optimal time for elective/semi-elective surgery
- 1st trimester: organogenesis risk; avoid if possible
- 3rd trimester: technically difficult; high risk of preterm labor
- General anesthesia is generally safe; maintain left lateral tilt to avoid aortocaval compression
- Fetal monitoring before and after surgery; tocolysis may be needed for preterm contractions
- Continue thromboprophylaxis (LMWH) perioperatively
Appendicitis in Pregnancy
- Most common non-obstetric surgical emergency
- Appendix displaced superolaterally as pregnancy progresses - pain in right flank/RUQ, not RIF
- Delay in diagnosis and perforation rate is higher (10-43%)
- Perforated appendicitis → peritonitis → preterm labor, fetal mortality ~20%
- Prompt surgical intervention is mandatory - risk of delay far exceeds operative risk
- Laparoscopy is safe in 1st and 2nd trimesters; open approach preferred in 3rd trimester
- Antibiotics: metronidazole + cephalosporin
Cholecystitis and Biliary Disease
- Conservative management initially; cholecystectomy in 2nd trimester if needed
- Symptomatic cholelithiasis recurs in 40-70% without definitive treatment
Ovarian Torsion
- Most common gynaecologic emergency in pregnancy
- Ovarian cysts (especially corpus luteum, dermoid, stimulated ovaries from IVF) predispose
- Presents: acute severe unilateral pelvic pain, N/V
- Diagnosis: Doppler ultrasound (absent/reduced blood flow)
- Treatment: laparoscopic detorsion (even if appears necrotic - the ovary often recovers)
Trauma in Pregnancy
- Leading cause of non-obstetric maternal death
- Physical examination unreliable (displaced organs); maintain high suspicion
- Kleihauer-Betke test for feto-maternal hemorrhage in Rh-negative mothers → anti-D immunoglobulin
- Fetal monitoring 4-6 hours after significant trauma (risk of placental abruption)
- DPL, FAST, and CT can be performed when clinically indicated
- Left lateral tilt for all unconscious or supine patients
Summary Table: Key Drug Safety Principles
| Condition | Safe in Pregnancy | Contraindicated |
|---|---|---|
| Diabetes | Insulin, metformin (GDM), glyburide (limited use) | ACE-I, statins, most oral hypoglycemics |
| Hypertension | Labetalol, nifedipine, methyldopa | ACE-I, ARBs, atenolol (caution) |
| Epilepsy | Lamotrigine, levetiracetam | Valproate (highest risk), avoid if alternatives exist |
| Thyroid | Levothyroxine, PTU (1st tri), methimazole (2nd/3rd) | Radioiodine, carbimazole in 1st tri |
| Asthma | Inhaled salbutamol, budesonide | NSAIDs (aspirin-sensitive) |
| SLE/RA | Hydroxychloroquine, azathioprine, prednisolone | Methotrexate, cyclophosphamide, mycophenolate |
| IBD | Mesalazine, corticosteroids, azathioprine | Methotrexate, thalidomide |
| Infections | Penicillins, cephalosporins, macrolides, acyclovir | Tetracyclines, aminoglycosides (prolonged), fluoroquinolones, chloramphenicol |
| VTE | LMWH, UFH | Warfarin (1st tri), NOACs |