Tinnitus
Reading File
Finding Sources
Searching PubMed
tinnitus management treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have enough information for a comprehensive answer. Let me compile the full response.
Tinnitus
Definition
Tinnitus is the perception of sound in the absence of an external acoustic source. It affects an estimated 50 million adults in the United States, with roughly 16 million experiencing frequent or chronic tinnitus. Only about 20% find it bothersome enough to seek treatment, but in those cases it significantly impacts quality of life - causing insomnia, impaired concentration, difficulty understanding speech, and depression. - Cummings Otolaryngology Head and Neck Surgery
Classification
Three key distinctions guide evaluation:
1. Subjective vs. Objective
- Subjective: Heard only by the patient. Accounts for ~98.5% of tinnitus.
- Objective: Audible to both patient and examiner (only 1.5% of otolaryngology referrals). Implies an identifiable sound source - turbulent blood flow, muscle/joint movement, or otoacoustic emissions.
2. Pulsatile vs. Nonpulsatile
- Nonpulsatile: Most common (~90% of referrals). Described as ringing, hissing, buzzing, or roaring. Almost exclusively subjective.
- Pulsatile: Rhythmic, pulse-synchronous. Can be subjective or objective. May change with position.
3. Primary vs. Secondary
- Primary: No identifiable cause; may or may not be associated with sensorineural hearing loss (SNHL).
- Secondary: Has an underlying condition (auditory or non-auditory).
Etiology / Causes
| System | Examples |
|---|---|
| Inner ear | SNHL, Meniere disease, presbycusis, noise-induced hearing loss |
| Middle ear | Otosclerosis, cholesteatoma, ossicular/TM abnormalities |
| External ear | Cerumen impaction, canal occlusion |
| Infection | Otitis media, labyrinthitis, herpes zoster oticus |
| Vascular | AVM, glomus tumor, stenotic carotid, dehiscent jugular bulb, hypertension |
| Neurologic | MS, vestibular schwannoma, migraine |
| Ototoxic drugs | Aminoglycosides, NSAIDs, loop diuretics, aspirin, antineoplastics |
| Metabolic | Hypothyroidism, hyperthyroidism, diabetes, hyperlipidemia |
| Musculoskeletal | TMJ disorder, palatal/stapedial myoclonus |
| Psychiatric | Anxiety, depression |
| Social | Caffeine, nicotine, alcohol |
- Textbook of Family Medicine 9e; Cummings Otolaryngology
Pathophysiology (Subjective Nonpulsatile Tinnitus)
The leading model proposes that a peripheral cochlear insult - most often noise damage or age-related degeneration - triggers neural hyperexcitability and aberrant central auditory plasticity. Tinnitus becomes conscious when this reorganized central auditory system induces further neuroplasticity in cortical networks, and becomes bothersome when linked through learned associations to unpleasant emotions. This explains why many people have tinnitus without obvious peripheral pathology and why central nervous system-targeted therapies are a focus of research. - Cummings Otolaryngology
Clinical Evaluation
History
Key questions to ask:
- Unilateral or bilateral? (Asymmetric = red flag)
- Pulsatile or non-pulsatile?
- Onset, duration, severity
- Associated symptoms: hearing loss, vertigo, headache, focal neurologic changes
- Medication review (ototoxic drugs)
- Noise exposure history
Physical Examination
- Full ENT examination
- Auscultation of neck, periauricular region, and chest for bruits/murmurs
- Otoscopy (retrotympanic mass? Normal TM?)
Audiometry
Mandatory for all patients with tinnitus. - Textbook of Family Medicine 9e
Investigations
| Scenario | Investigation |
|---|---|
| Bilateral, symmetric hearing loss, non-pulsatile | Audiogram only; likely secondary to SNHL, no further imaging needed |
| Asymmetric hearing loss | MRI with contrast (to rule out vestibular schwannoma) |
| Pulsatile tinnitus + normal otoscopy | MR angiography (to evaluate vascular anomalies) |
| Retrotympanic mass on otoscopy | CT temporal bone |
| Suspicion of anemia/thyroid disease | Blood tests (CBC, TFTs) |
| Bruit/murmur found on auscultation | Carotid duplex ultrasound or echocardiogram |
Important: Most arterial pulsatile tinnitus is due to atherosclerotic carotid disease. Venous pulsatile tinnitus often improves with digital compression of the internal jugular vein and may be due to a high-riding jugular bulb or benign intracranial hypertension.
Somatic Tinnitus
A special subtype where the loudness, laterality, or tonality of tinnitus can be modulated by head/neck maneuvers. This is a diagnostically useful finding and links tinnitus to the somatosensory system.
Management
Effective treatment is challenging and usually requires a multimodal approach. The priority is identifying and eliminating the underlying cause.
Non-pharmacological (First Line - Best Evidence)
- Cognitive Behavioral Therapy (CBT): Strong evidence for reducing tinnitus distress and improving quality of life.
- Tinnitus Retraining Therapy (TRT): Combines directive counseling and sound therapy to habituate the patient to tinnitus. Clinical trials support its efficacy.
- Sound Masking / Tinnitus Maskers: Devices that produce competing noise to mask tinnitus. Helpful especially when co-existing hearing loss is present.
- Hearing aids: Beneficial in patients with hearing loss - masking the tinnitus is a side benefit.
- Counseling / Education: Reducing anxiety around tinnitus is itself therapeutic.
- Avoidance: Caffeine, nicotine, and ototoxic agents should be eliminated or minimized.
Pharmacological (Limited Evidence)
- Antidepressants (SSRIs, TCAs, trazodone): Modest, inconsistent benefit. May reflect improvement in comorbid depression/anxiety rather than a direct effect on tinnitus. Routine use is not recommended.
- Benzodiazepines (alprazolam, oxazepam): Some reduction in tinnitus severity on VAS scales, but no significant benefit on validated instruments (Tinnitus Handicap Inventory). Abuse potential and adverse effects, especially in the elderly, mean routine use is not recommended.
- Anticonvulsants / Gabapentin: Seven placebo-controlled trials and systematic reviews show no benefit. Not recommended.
- Acamprosate: Two small promising RCTs, but insufficient evidence to recommend routinely.
- Intratympanic steroids/lidocaine: Three RCTs showed no benefit over placebo. IT lidocaine carries significant vestibular side effects and is generally discouraged.
- IV lidocaine: Historical interest only; short duration and adverse effects limit use.
- Zinc, Ginkgo biloba, melatonin, multivitamins: No clear demonstrated benefit in RCTs. Ginkgo biloba carries bleeding risk with anticoagulants/antiplatelets. Routine use not recommended.
- Cummings Otolaryngology Head and Neck Surgery
Assessment Tool
The Tinnitus Handicap Inventory (THI) is a validated 25-item questionnaire scored 0-100, with higher scores indicating greater severity. It is used to quantify impact and monitor treatment response. - Shambaugh Surgery of the Ear
Prognosis
Approximately 28% of acute tinnitus (duration < 6 months) resolves spontaneously. Chronic tinnitus is less likely to resolve but can be habituated with appropriate therapy. - Cummings Otolaryngology
Recent Evidence (2025)
Three major reviews published in 2025 are relevant:
- The VA/DoD Clinical Practice Guideline (JAMA Otolaryngol, 2025) provides updated evidence-based recommendations for tinnitus management (PMID: 40111327).
- A network meta-analysis in BMJ Open (2025) systematically reviewed pharmacotherapy options for subjective tinnitus (PMID: 40441764).
- An umbrella review in Am J Otolaryngol (2025) synthesized evidence across all tinnitus treatment modalities (PMID: 40712351).
These recent reviews reinforce the textbook picture: behavioral interventions (CBT, TRT) remain the cornerstone of management, while pharmacotherapy has limited and inconsistent evidence.
Arrhythmia
Finding Sources
Searching PubMed
cardiac arrhythmia management guidelines
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have all the material needed for a comprehensive answer, including two high-quality diagrams from the textbooks.
Cardiac Arrhythmia
Definition
A cardiac arrhythmia is any abnormality in the initiation or propagation of the cardiac electrical impulse. The term encompasses a vast spectrum - from benign ectopic beats to life-threatening ventricular fibrillation. - Harrison's Principles of Internal Medicine, 22nd ed.
Mechanisms
There are three fundamental electrophysiologic mechanisms that underlie all arrhythmias:
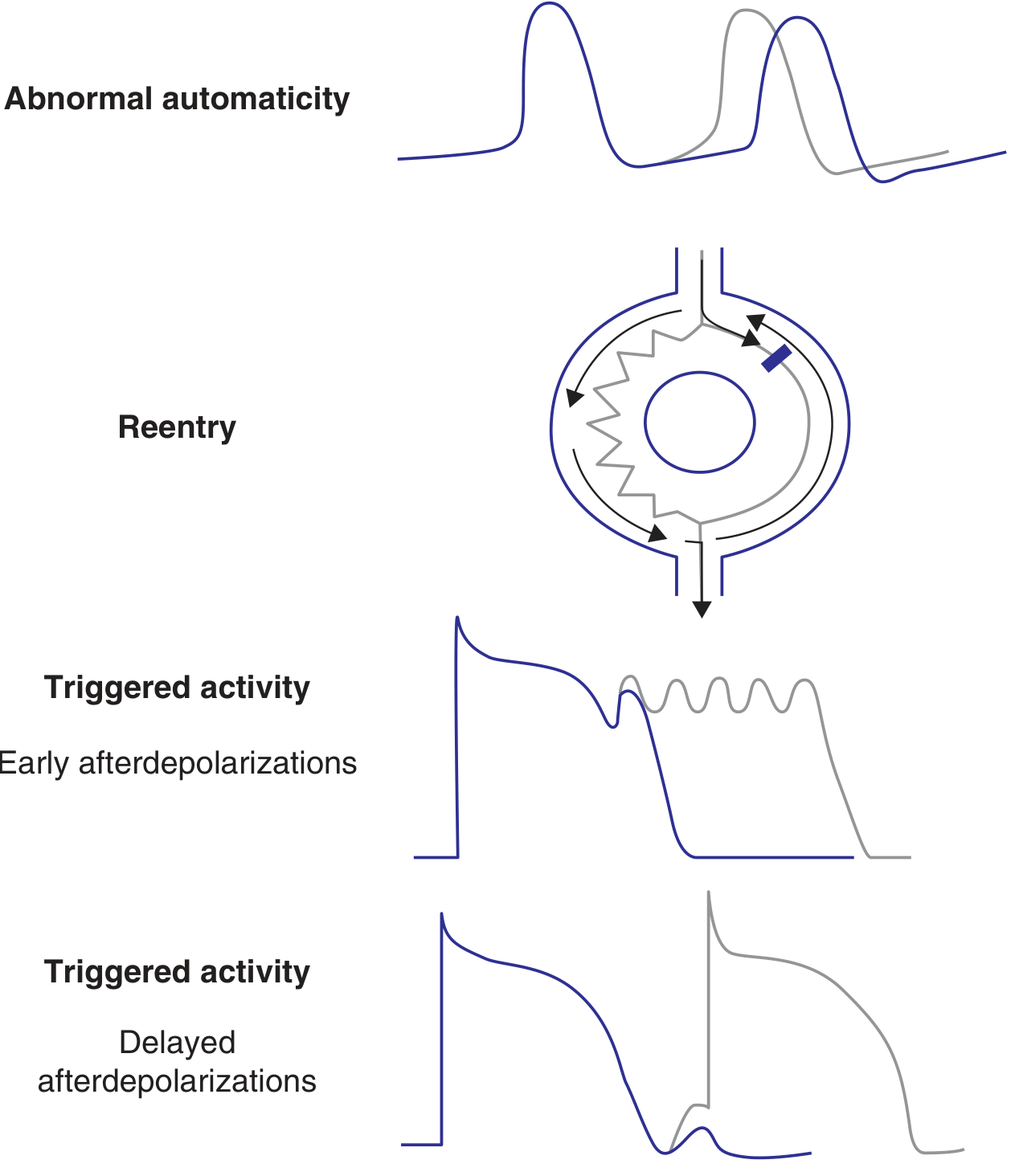
Figure: The three main tachyarrhythmia mechanisms - abnormal automaticity (top), reentry (middle), and triggered activity via early and delayed afterdepolarizations (bottom). - Harrison's Principles of Internal Medicine
1. Abnormal Automaticity
Automaticity is the ability of cardiac cells to spontaneously depolarize during phase 4 of the action potential (AP). This is a normal property of the SA node, AV node, and His-Purkinje system. Pathologic automaticity can arise when:
- The SA node fires inappropriately fast (e.g., inappropriate sinus tachycardia)
- Other sites in the heart acquire automatic firing (pulmonary veins in AF, ventricular outflow tracts in idiopathic VT, ischemic border zones causing PVCs)
- The SA node fails, and a lower escape rhythm takes over
Autonomic regulation is central: parasympathetic (ACh) input hyperpolarizes nodal cells via IKAch channels, slowing automaticity; sympathetic input via beta-1 adrenergic receptors enhances L-type Ca channel activation, accelerating automaticity.
2. Triggered Activity (Afterdepolarizations)
Triggered arrhythmias depend on prior stimulation and are caused by abnormal afterdepolarizations:
- Early afterdepolarizations (EADs): Occur during phase 2 or 3 of the AP (before full repolarization). Seen with QT prolongation, hypokalemia, bradycardia, or drugs that prolong the AP (sotalol, dofetilide). Classic example: Torsades de Pointes (TdP).
- Delayed afterdepolarizations (DADs): Occur in phase 4 (after complete repolarization). Caused by intracellular calcium overload. Seen with digoxin toxicity, catecholamine excess, reperfusion arrhythmias.
3. Reentry
The most common mechanism for sustained tachyarrhythmias. Requires:
- Two electrically distinct pathways forming a circuit
- Unidirectional block in one pathway (the impulse goes one way only)
- Slow enough conduction in the alternate pathway that by the time it completes the circuit, the blocked pathway has recovered excitability
The circuit perpetuates itself in a circus movement. Examples: AVNRT, AVRT (WPW), atrial flutter, scar-related VT.
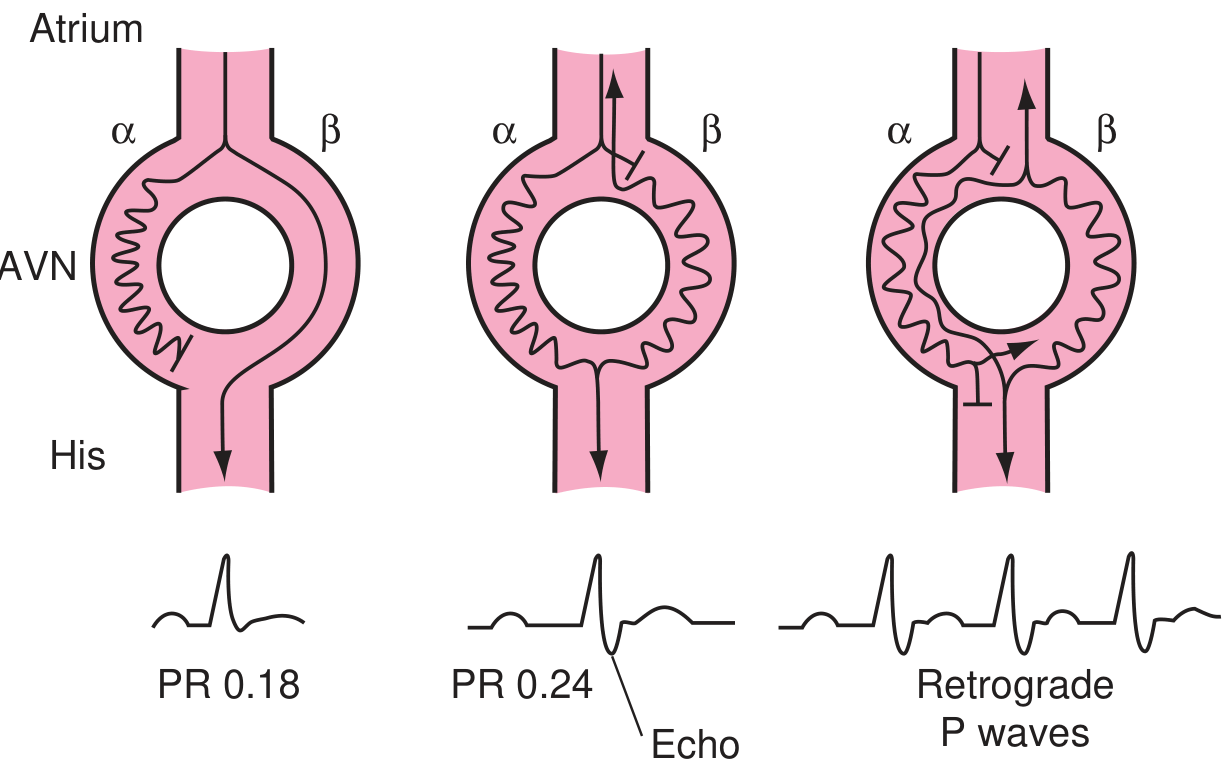
Figure: Mechanism of AVNRT. Left - normal conduction via both fast and slow pathways, PR 0.18. Centre - block in fast pathway, slow pathway conducts with PR 0.24, echo beat forms as fast pathway recovers retrograde. Right - sustained reentry with retrograde P waves. - Textbook of Family Medicine 9e
| Tachyarrhythmia Category | Mechanism | Prototypical Arrhythmias |
|---|---|---|
| Abnormal automaticity | Enhanced phase 4 depolarization | Idiopathic VT, atrial tachycardia |
| EADs (triggered) | Depolarization during repolarization | TdP in long QT syndrome, PVCs |
| DADs (triggered) | Depolarization after repolarization | Digoxin toxicity AT/VT, reperfusion VT |
| Reentry | Anatomic or functional circuit with unidirectional block | AVNRT, AVRT, atrial flutter, scar VT |
- Harrison's Principles of Internal Medicine, 22nd ed.
Classification
Bradyarrhythmias (Rate < 60 bpm)
- Sinus node dysfunction: Sick sinus syndrome, sinoatrial block, sinus pauses
- AV conduction disease: 1st, 2nd (Mobitz I/II), 3rd degree (complete) AV block
- Bundle branch/fascicular block: LBBB, RBBB, hemiblocks - may not cause bradycardia but disrupt conduction
Tachyarrhythmias (Rate > 100 bpm)
Divided by origin:
Supraventricular (SVT) - arise above or at the bundle of His:
- Sinus tachycardia (physiologic or inappropriate)
- Atrial fibrillation (AF)
- Atrial flutter
- Atrial tachycardia (AT)
- AV nodal reentrant tachycardia (AVNRT)
- AV reentrant tachycardia (AVRT) - involves an accessory pathway (WPW)
- Junctional tachycardia
Ventricular - arise below the bundle of His:
- Premature ventricular contractions (PVCs)
- Ventricular tachycardia (VT): monomorphic or polymorphic
- Torsades de Pointes (TdP)
- Ventricular fibrillation (VF)
- Accelerated idioventricular rhythm (AIVR)
Clinical Presentation
Symptoms arise from two sources:
- The arrhythmia itself: Palpitations, awareness of rapid/slow/irregular heartbeat, sensation of "missed beats" from PVCs
- Hemodynamic consequences: Presyncope, syncope, dyspnea, chest discomfort, fatigue, exacerbation of heart failure or angina
Key points from history:
- Arrhythmias triggered by exercise or stress suggest adrenergic (sympathetic) arrhythmias
- Medications (beta-blockers, CCBs) may cause bradycardia; QT-prolonging drugs may cause TdP
- Family history of unexplained sudden death suggests heritable syndromes (long QT, Brugada, CPVT, HCM)
- Demographics matter: AF is rare in young healthy adults; Brugada syndrome predominates in young Southeast Asian males; inappropriate sinus tachycardia almost exclusively affects young women
- Harrison's Principles of Internal Medicine, 22nd ed.
Diagnosis
| Investigation | Purpose |
|---|---|
| 12-lead ECG | First-line in all patients; identifies rhythm, QRS morphology, QT interval, delta waves (WPW), ST changes |
| Ambulatory ECG monitoring (Holter 24-48h, event recorder, implantable loop recorder) | Correlates symptoms with arrhythmia; duration chosen based on frequency of symptoms |
| Exercise treadmill test (ETT) | Provokes exercise-induced arrhythmias; evaluates QT response to rate in long QT |
| Echocardiography | Assesses structural heart disease, LV function, atrial dimensions |
| Electrophysiology (EP) study | Most definitive test; intracardiac recordings + programmed electrical stimulation; maps circuits; performed pre-ablation |
| Cardiac MRI/CT | Assesses for scar, cardiomyopathy, infiltrative disease, coronary anatomy |
| Pharmacologic provocation | E.g., sodium channel blocker (ajmaline/flecainide) challenge to unmask Brugada pattern |
| Tilt table testing (TTT) | Evaluates vasovagal/neurocardiogenic syncope (limited sensitivity/specificity) |
Treatment
1. Antiarrhythmic Drug Therapy (Vaughan-Williams Classification)
| Class | Target | Key Drugs | Main Use |
|---|---|---|---|
| IA | Na channel (intermediate kinetics) | Procainamide, Quinidine, Disopyramide | Pre-excited AF (WPW), ventricular arrhythmias |
| IB | Na channel (fast kinetics, low potency) | Lidocaine, Mexiletine | Ventricular arrhythmias, reperfusion VT |
| IC | Na channel (slow kinetics, high potency) | Flecainide, Propafenone | SVT in structurally normal heart; AVOID post-MI |
| II | Beta-adrenergic receptors | Metoprolol, Atenolol, Esmolol | Rate control in AF, VT prevention, post-MI |
| III | K channels (prolong AP/refractory period) | Amiodarone, Sotalol, Dofetilide, Ibutilide, Dronedarone | Ventricular arrhythmias, AF rhythm control |
| IV | L-type Ca channels | Verapamil, Diltiazem | Rate control in AF, AVNRT, AVRT |
| Other | Adenosine receptor | Adenosine | Acute termination of AVNRT/AVRT |
Important caveats:
- Antiarrhythmic drugs carry a narrow therapeutic index and are proarrhythmic in their own right (e.g., flecainide can promote reentrant flutter, sotalol/dofetilide cause TdP)
- Many carry multiorgan toxicity: amiodarone causes pulmonary, hepatic, thyroid, and corneal toxicity with long-term use
- Class IC agents are contraindicated in ischemic heart disease (CAST trial mortality harm)
- Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology; Harrison's
2. Electrical Cardioversion / Defibrillation
- Synchronized DC cardioversion: Used for hemodynamically unstable tachyarrhythmias or elective cardioversion of AF/flutter; delivers shock synchronized to the R wave to avoid the vulnerable T-wave period
- Defibrillation (unsynchronized): Used for VF and pulseless VT; cornerstone of ACLS
3. Catheter Ablation
- Radiofrequency (RF) energy or cryotherapy delivered via catheter to ablate the critical isthmus or focus of arrhythmia
- Indications: AVNRT (curative), AVRT/WPW (curative), AF (pulmonary vein isolation), atrial flutter (cavotricuspid isthmus ablation), scar-related VT
- Pulsed field ablation (PFA) is an emerging non-thermal modality for pulmonary vein isolation
- Modern EP studies are almost always performed in conjunction with planned ablation
4. Implanted Devices
- Pacemakers: Primary therapy for symptomatic sinus node dysfunction and symptomatic AV conduction disease; rate-adaptive pacing maintains cardiac output. Leadless pacemakers now available.
- Implantable Cardioverter-Defibrillators (ICDs): Sense malignant ventricular arrhythmias and deliver anti-tachycardia pacing (ATP) or shock; used for primary prevention (e.g., EF ≤35% with NYHA Class II-III HF) and secondary prevention (survivors of VF/hemodynamically unstable VT). Subcutaneous ICD systems avoid intravenous leads.
5. Autonomic Modulation (Refractory VT)
- Stellate ganglion blockade or thoracic epidural anesthesia for VT storm
- Bilateral cardiac sympathetic denervation for refractory ventricular arrhythmias
- Renal denervation: Emerging data for reducing ventricular arrhythmia burden
- Harrison's Principles of Internal Medicine, 22nd ed.; Braunwald's Heart Disease
Proarrhythmia - A Critical Concept
Antiarrhythmic drugs can cause arrhythmias as well as suppress them. The CAST trial showed that class IC agents (flecainide, encainide) increased mortality post-MI despite suppressing PVCs. Drugs that prolong the QT interval (sotalol, dofetilide, quinidine) can precipitate TdP, particularly at slow heart rates. This underscores that the decision to treat must weigh the risk of the arrhythmia against the risk of the treatment itself.
Recent Guidelines (2024-2025)
- The 2024 ESC Guidelines for AF management (Eur Heart J, 2024) provide updated recommendations on rhythm vs. rate control, stroke prevention, and catheter ablation for AF (PMID: 39210723).
- The 2025 AHA CPR & Emergency Cardiovascular Care Guidelines (Circulation, 2025) update management of pulseless VT/VF in cardiac arrest (PMID: 41122893).
This is a shared conversation. Sign in to Orris to start your own chat.