As a mentor teach me lens for neet pg 2026
🔬 LENS - Complete NEET PG 2026 Master Guide
Your Mentor's Session — Ophthalmology High-Yield
MODULE 1: EMBRYOLOGY OF THE LENS
- Surface ectoderm overlying the optic vesicle thickens → lens placode
- Lens placode invaginates → lens pit → pinches off → lens vesicle
- Anterior wall of vesicle = cuboidal cells → becomes subcapsular lens epithelium
- Posterior wall cells elongate, nuclei dissolve → become primary lens fibers (fill the vesicle cavity)
- Equatorial zone cells → proliferate and elongate → become secondary lens fibers (added throughout life)
- PAX6 + SOX2 - required for lens induction
- PITX3, GATA3, FOXE3 - regulate lens fiber formation and differentiation
- During development: hyaloid artery (distal part) via tunica vasculosa lentis
- Fetal period: hyaloid artery degenerates → lens becomes avascular (unique!)
- Adult lens: nourished by diffusion from aqueous humor (anterior) and vitreous humor (posterior)
- Hyaloid canal = remnant of hyaloid artery in vitreous body
- Persistent pupillary membrane = incomplete regression of tunica vasculosa lentis anterior part
- Persistent hyaloid artery = Mittendorf's dot (on posterior lens capsule)
Lens capsule = greatly thickened basement membrane of lens epithelium + lens fibers. Composed of type IV collagen + proteoglycans.
- The Developing Human (Clinically Oriented Embryology), p. 1136
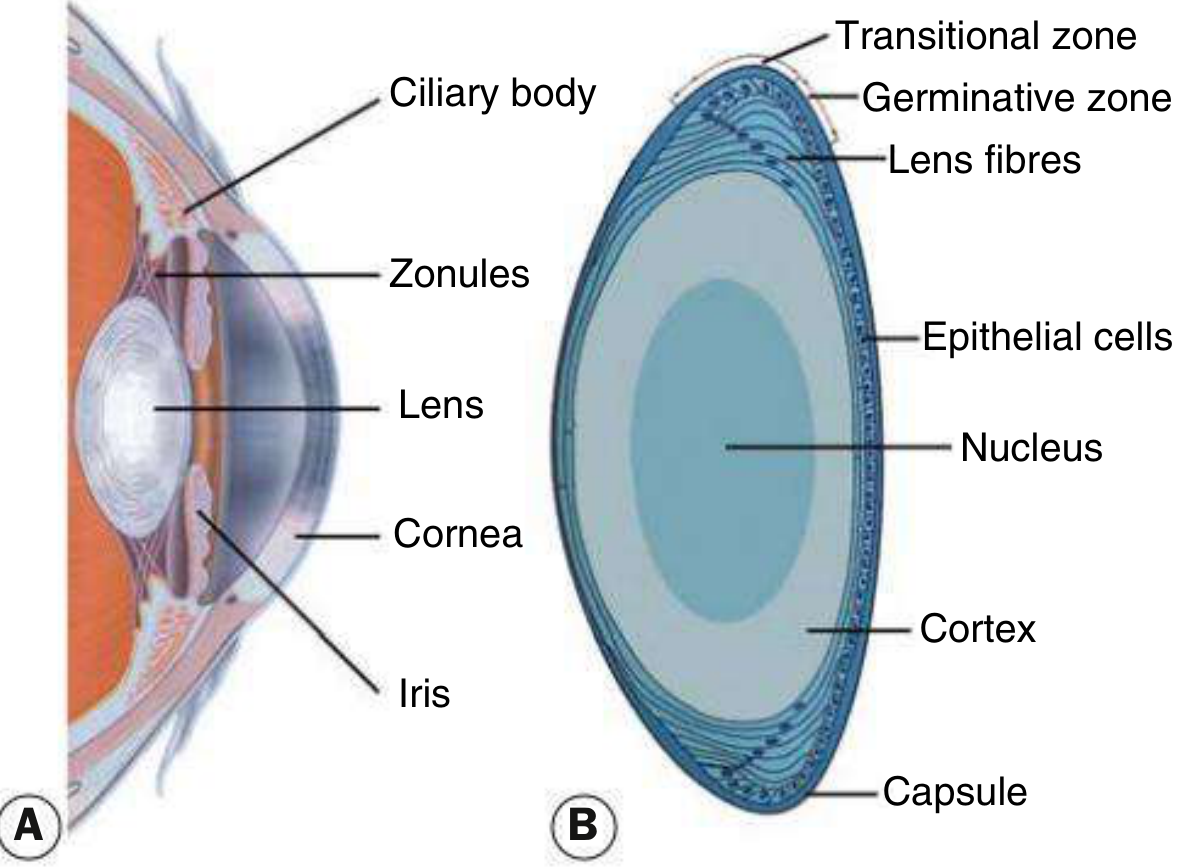
MODULE 2: ANATOMY OF THE LENS
| Feature | Detail |
|---|---|
| Shape | Biconvex, transparent, elastic |
| Position | Behind iris, in front of vitreous |
| Suspension | Zonules of Zinn (from ciliary body) |
| Blood supply | None (avascular) |
| Nerve supply | None |
| Thickness (adult) | ~4 mm at rest; ~4.5 mm on accommodation |
| Refractive power | ~18-20 D (at rest); cornea contributes ~44 D |
1. Lens Capsule
- Acellular, homogeneous, elastic membrane
- Composed of type IV collagen + proteoglycans
- Thickest: anterior capsule near equator (14 μm)
- Thinnest: posterior pole (~2-4 μm) - clinically important! (posterior capsule ruptures more easily)
- Zonular fibers attach here
2. Anterior Lens Epithelium
- Single layer of cuboidal cells - ONLY on anterior surface (NOT posterior!)
- Cells rest on capsule basally; apices directed inward
- Germinative zone: cells at equator divide continuously → differentiate into lens fibers
- These are the cells responsible for all lens growth throughout life
3. Lens Fibers
- Highly elongated, terminally differentiated cells
- 7-10 mm long; 2×8 μm cross-section
- Cytoplasm fills with crystallins (structural proteins giving transparency)
- Mature lens fibers: lose organelles AND nucleus (another unique feature - like red blood cells)
- Packed tightly in regular arrays → perfect transparency
- Embryonic nucleus (center, oldest)
- Fetal nucleus
- Infantile nucleus
- Adult nucleus
- Cortex (periphery, newest fibers)
Nucleus = older, central fibers. Cortex = newer, peripheral fibers. The nucleus undergoes sclerosis (hardening) with age.
4. Histology (H&E Section)

- Junqueira's Basic Histology, 17e, p. 1192
MODULE 3: PHYSIOLOGY - ACCOMMODATION
- Ciliary muscle contracts → ciliary body moves forward and inward
- Zonular fibers relax (become slack)
- Lens becomes more spherical/convex (elastic recoil) → increased refractive power
- Pupil constricts (miosis) → sharper image
- Eyes converge (convergence)
- Gradual loss of accommodation with age
- Cause: loss of lens elasticity (lens becomes harder/sclerotic)
- Also: weakening of ciliary muscle
- Onset: ~40-45 years
- Treatment: reading glasses (convex/plus lens), multifocals, or refractive surgery
-
Normal lens refractive index: ~1.40 (nucleus) to ~1.36 (cortex)
-
Nuclear sclerosis → increased refractive index → myopic shift ("second sight of the aged" - elderly can read without glasses again, but distance vision worsens)
-
Hyperglycemia → glucose → sorbitol accumulates → osmotic swelling → myopic shift (fluctuating refraction with blood sugar)
-
Hypoglycemia → opposite → hypermetropic shift
-
Kanski's Clinical Ophthalmology, 10th ed., p. 322
MODULE 4: CATARACT - THE HIGH-YIELD CORE
"Cataract is the commonest cause of reversible blindness worldwide" - This fact appears repeatedly in MCQs.
A. Types of Age-Related Cataract
| Type | Key Feature | High-Yield Point |
|---|---|---|
| Posterior Subcapsular (PSC) | Just in front of posterior capsule; granular/plaque appearance; black + vacuolated on retroillumination | Worst effect on vision (at nodal point); worse with miosis (near work, bright light); caused by steroids, radiation, diabetes |
| Nuclear Sclerotic | Yellow/brown nucleus; best seen on oblique slit lamp | Causes myopic shift; "second sight of aged"; brown = brunescent; black = black cataract |
| Cortical | Cuneiform (wedge-shaped) / spoke-like opacities; starts inferonasal | Vacuoles/clefts due to cortical hydration |
| Anterior Subcapsular | Under anterior capsule; fibrous metaplasia of epithelium | Less common; associated with atopic disease |
B. Grades of Cataract Maturity (High-Yield MCQ!)
| Stage | Lens Appearance | Key Distinguishing Feature |
|---|---|---|
| Immature | Partially opaque | Shadow on iris when light shone |
| Mature | Completely opaque | No shadow (absent iris shadow); no red reflex |
| Hypermature | Shrunken, wrinkled anterior capsule | Water leaks out of lens |
| Morgagnian | Hypermature + liquefied cortex | Nucleus sinks inferiorly (gravity) |
- Immature cataract → iris shadow present (lens not fully opaque)
- Mature cataract → no iris shadow (lens fully opaque)
C. Cataract in Systemic Diseases
| Disease | Cataract Type | Mechanism/Notes |
|---|---|---|
| Diabetes mellitus | Snowflake cortical (classic, young); nuclear sclerosis (common) | Glucose → sorbitol (aldose reductase) → osmotic overhydration → cortical vacuoles/opacities |
| Myotonic dystrophy | Fine iridescent cortical → star-shaped/wedge (later) | ~90% develop it by 3rd decade; resembles Christmas tree initially |
| Down syndrome | Various, including "sunflower" | Trisomy 21 |
| Wilson's disease | "Sunflower cataract" | Due to copper deposition; anterior subcapsular; also seen in chalcosis |
| Galactosemia | Oil droplet (lamellar) cataract | Galactitol accumulation; early-onset congenital; enzyme: galactose-1-P uridyl transferase |
| Fabry's disease | Posterior spoke-like opacity | X-linked; alpha-galactosidase deficiency |
| Atopic dermatitis | Anterior or posterior subcapsular | Typically anterior shield-like |
| Hypoparathyroidism | Lamellar/zonular | Low calcium → lens opacification |
| Retinitis pigmentosa + other fundus dystrophies | Posterior subcapsular | Most hereditary retinal dystrophies |
D. Drug-Induced Cataracts
| Drug | Cataract Type |
|---|---|
| Steroids (systemic or topical) | Posterior subcapsular |
| Chlorpromazine (phenothiazine) | Anterior star-shaped opacity |
| Busulfan | Posterior subcapsular |
| Amiodarone | Anterior subcapsular stellate |
| Miotics (long-acting, e.g., echothiophate) | Anterior subcapsular |
E. Traumatic Cataract
| Trauma Type | Cataract Pattern |
|---|---|
| Blunt trauma | Rosette/flower-shaped (posterior sutures); Vossius ring (ring opacity from iris pigment imprint on anterior lens) |
| Penetrating trauma | Rapid opacification at injury site |
| Electric shock | Diffuse milky-white; stellate subcapsular |
| Infrared radiation (glassblowers) | True exfoliation of anterior lens capsule |
| Ionizing radiation | Posterior subcapsular (months to years later) |
- Kanski's Clinical Ophthalmology, 10th ed., pp. 323-327
MODULE 5: LENS DISLOCATION (ECTOPIA LENTIS)
- Subluxation: partial dislocation (zonules partially torn)
- Luxation: complete dislocation (all zonules torn)
| Condition | Direction of Dislocation | Key Association |
|---|---|---|
| Marfan syndrome | Upward and outward (superotemporal) | FBN1 gene; fibrillin-1 defect |
| Homocystinuria | Downward and inward (inferonasal) | CBS gene; thromboembolism risk; AR |
| Weill-Marchesani | Downward | Microspherophakia + short stature |
| Trauma | Any direction (toward intact zonules) | Most common cause of unilateral dislocation |
| Syphilis | Downward | |
| Sulfite oxidase deficiency | Downward |
- Iridodonesis (trembling iris) and phakodonesis (trembling lens) on ocular movement
- Visible lens edge under mydriasis
- Uniocular diplopia (if pupil partly aphakic)
- Lenticular astigmatism (from tilting)
- Anterior luxation → acute angle closure glaucoma (pupil block)
- Posterior luxation into vitreous → vitreous floaters, later phacoanaphylactic uveitis
MODULE 6: CONGENITAL LENS ABNORMALITIES
| Condition | Description | High-Yield Point |
|---|---|---|
| Anterior lenticonus | Anterior surface protrudes | Associated with Alport syndrome (X-linked nephritis + deafness) |
| Posterior lenticonus | Posterior surface protrudes | Most common; causes progressive myopia; may → cataract |
| Lentiglobus | Spherical lens | Generalized protrusion |
| Microspherophakia | Small spherical lens | Weill-Marchesani; may cause angle-closure glaucoma; accommodation impaired |
| Microphakia | Small lens | |
| Coloboma | Notch in lens (inferonasal) | Due to incomplete closure of fetal fissure |
MODULE 7: LENS-RELATED GLAUCOMAS
| Type | Mechanism |
|---|---|
| Phacomorphic glaucoma | Intumescent (swollen) mature cataract → pupil block → acute angle closure |
| Phacolytic glaucoma | Hypermature cataract leaks lens proteins → macrophages block trabecular meshwork → OPEN angle glaucoma |
| Phacoanaphylactic uveitis | Lens protein leaks → immune response → granulomatous uveitis |
| Lens particle glaucoma | After trauma/surgery - free cortical material blocks trabeculum |
| Subluxated lens glaucoma | Pupil block by anteriorly displaced lens |
- Phacomorphic = Morphology (size/shape) problem → angle CLOSURE
- Phacolytic = Lens leaks (lysis) → OPEN angle
MODULE 8: CATARACT SURGERY (NEET PG Clinical Questions)
- Commonest surgical procedure in the world
- Uses ultrasound energy to emulsify nucleus
- Small incision (~2-3 mm), self-sealing
- Extracapsular technique: removes lens content, leaves posterior capsule intact for IOL support
- Posterior capsule left intact → later may develop posterior capsular opacification (PCO) = "after-cataract" - treated with Nd:YAG laser capsulotomy
- Caused by residual lens epithelial cells migrating to posterior capsule → Elschnig pearls (bladder/Wedl cells)
- Most common complication after cataract surgery
- Treatment: Nd:YAG posterior capsulotomy
- Standard position: in the bag (capsular bag)
- Power calculated using biometry: SRK/T formula, Holladay, Haigis
- Aphakia = absence of lens (after surgery or trauma)
- Pseudophakia = artificial IOL in place
- Dense unilateral cataract: surgery within 6-8 weeks of birth (to prevent amblyopia)
- Bilateral: within first few months
- Post-operative: aggressive amblyopia treatment (patching) required
MODULE 9: HIGH-YIELD MCQ SUMMARY TABLE
| Question Theme | Answer |
|---|---|
| Lens develops from | Surface ectoderm |
| Lens blood supply in adult | None - avascular; nourished by aqueous humor |
| Lens epithelium location | Anterior surface only |
| Thinnest part of lens capsule | Posterior pole |
| Commonest cause of reversible blindness | Cataract |
| Cataract type worst affected by miosis | Posterior subcapsular |
| Morgagnian cataract feature | Nucleus sinks inferiorly in liquefied cortex |
| "Second sight of aged" | Nuclear sclerosis → myopic shift |
| Marfan lens dislocation direction | Superotemporal (up + out) |
| Homocystinuria lens dislocation direction | Inferonasal (down + in) |
| Anterior lenticonus association | Alport syndrome |
| Sunflower cataract | Wilson's disease / chalcosis |
| Snowflake cataract | Diabetes mellitus (young) |
| Steroid cataract type | Posterior subcapsular |
| Chlorpromazine cataract | Anterior star-shaped |
| Traumatic cataract pattern (blunt) | Rosette/flower-shaped |
| Vossius ring | Iris pigment ring on anterior lens after blunt trauma |
| Phacomorphic glaucoma mechanism | Intumescent cataract → pupil block → angle closure |
| Phacolytic glaucoma mechanism | Hypermature cataract leaks proteins → open angle |
| After-cataract (PCO) treatment | Nd:YAG laser capsulotomy |
| Galactosemia cataract type | Oil droplet cataract |
MODULE 10: QUICK REVISION - ASSOCIATIONS TO MEMORIZE
Alport syndrome → Anterior lenticonus
Marfan → Upward dislocation
Homocystinuria → Downward dislocation
Wilson disease → Sunflower cataract
Myotonic dystrophy → Iridescent/Christmas tree → star shaped
Galactosemia → Oil drop cataract (early, reversible if treated)
Steroids → Posterior subcapsular
Chlorpromazine → Anterior star cataract
Blunt trauma → Rosette cataract + Vossius ring
Glassblower → True exfoliation (infrared)
Radiation → Posterior subcapsular (delayed)
Retinitis pigmentosa → Posterior subcapsular
Fabry disease → Posterior spoke-like (propeller cataract)
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
- Junqueira's Basic Histology, 17th Edition
- The Developing Human: Clinically Oriented Embryology
I want to according PREVIOUS YEAR TOPICS AND NEET PG PRIENTED
NEET PG previous year questions lens ophthalmology 2019 2020 2021 2022 2023 2024
NEET PG ophthalmology lens cataract previous year MCQ topics high yield 2024 2025
🎯 LENS - NEET PG 2026: PYQ-ORIENTED MASTER SESSION
Every topic mapped to Previous Year Questions (2015-2025)
📊 LENS IN NEET PG: THE NUMBERS
- Ophthalmology = 10 questions in NEET PG paper
- Lens/Cataract = 2-3 questions every year (the single highest-yielding topic in Ophtho)
- Question style: Clinical scenario + image-based (since 2020 onwards)
- Lens PYQ themes repeat every 2-3 years
⭐ PYQ TOPIC 1: CONGENITAL CATARACT - MANAGEMENT TIMING
(Asked NEET PG 2024, 2022, 2019, AIIMS multiple times)
"2-month-old infant with white reflex/absent red reflex in one eye. What is ideal management?" Answer: Operate immediately ✅
Why the urgency? - Amblyopia deprivation
- Dense unilateral cataract → visual cortex does not develop → permanent amblyopia
- Window of plasticity: first 8-10 weeks of life
- Rule of thumb: surgery within 6-8 weeks of birth for dense unilateral cataract
- After surgery: optical correction + patching of the good eye (amblyopia therapy mandatory)
Congenital Cataract Causes - PYQ Table:
| Cause | Cataract Type | Key Fact |
|---|---|---|
| Rubella (TORCH) | Dense nuclear (leukocoria) | First trimester infection; "salt and pepper" retinopathy also present; Pearl: rubella = most common cause of congenital cataract in developing countries |
| Galactosemia | Oil-droplet (lamellar) - REVERSIBLE | Galactose-1-P uridyltransferase deficiency; treated with galactose-free diet → cataract can regress |
| Galactokinase deficiency | Oil-droplet cataract ONLY (no liver/brain) | Milder; cataracts only |
| Lowe syndrome (oculocerebrorenal) | Dense nuclear | X-linked; aminoaciduria + intellectual disability |
| Down syndrome | Lamellar/sutural/snowflake | Trisomy 21 |
| Persistent Fetal Vasculature (PFV) | Posterior + total; unilateral | Failed hyaloid regression; microphthalmia |
⭐ PYQ TOPIC 2: PSEUDOEXFOLIATION SYNDROME
(Asked NEET PG 2024 - exact question confirmed)
"Elderly patient with white, dandruff-like deposits on anterior lens surface on slit lamp. Diagnosis?" Answer: Pseudoexfoliation syndrome ✅
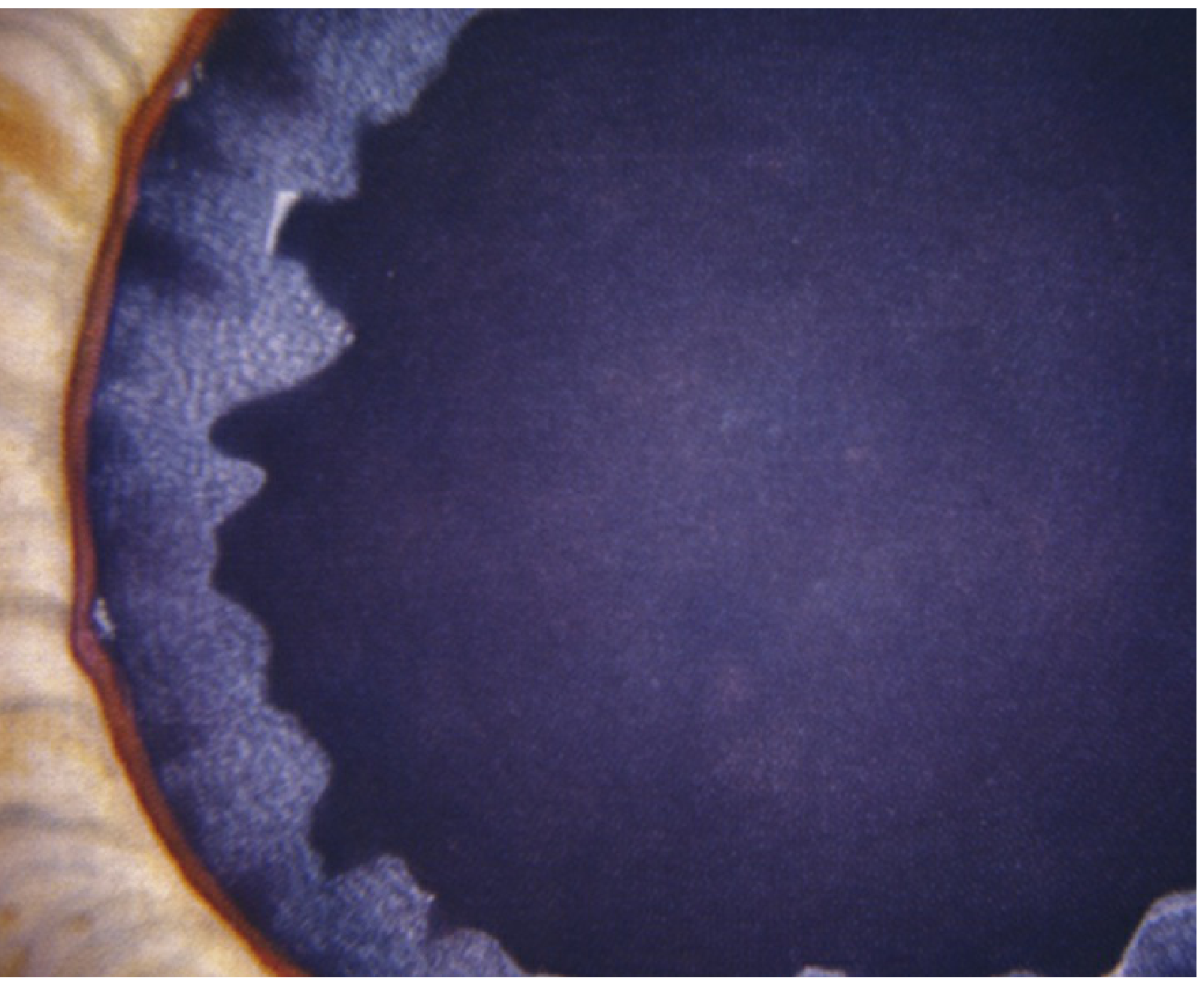
- White flaky material on: anterior lens capsule (target pattern: central disc + middle clear zone + peripheral ring) + pupillary margin
- Associated with: open-angle glaucoma (exfoliative glaucoma - hardest to control IOP)
- Sampaolesi line (pigment anterior to Schwalbe line) on gonioscopy
- Poor pupil dilation (iris dilator atrophy) → difficult cataract surgery
- Zonular weakness → lens subluxation risk during phaco
- Bilateral but asymmetric
-
True exfoliation (capsular delamination): Glassblower's cataract, infrared heat, trauma → thin membrane peels off anterior lens capsule. Glaucoma uncommon.
-
Pigment dispersion: Krukenberg spindle on cornea; pigment on POSTERIOR lens equator; deep AC; myope
-
Wills Eye Manual, p. 596
⭐ PYQ TOPIC 3: LENS DISLOCATION DIRECTIONS
(The most repeated PYQ - asked almost every year)
"Marfan syndrome: lens dislocates in which direction?" Answer: Superotemporal (upward + outward) ✅
"Homocystinuria: lens dislocates in which direction?" Answer: Inferonasal (downward + inward) ✅
Complete Dislocation Table - PYQ Ready:
| Condition | Direction | Extra PYQ Fact |
|---|---|---|
| Marfan syndrome | Superotemporal | Autosomal dominant; FBN1 gene; fibrillin-1; also aortic aneurysm |
| Homocystinuria | Inferonasal | Autosomal recessive; CBS gene; thromboembolism risk (surgery/GA dangerous); methionine-free diet |
| Weill-Marchesani | Inferonasal | Microspherophakia + short stature + brachydactyly; reverse of Marfan |
| Trauma | Toward intact zonules (any direction) | Commonest cause of unilateral lens dislocation |
| Syphilis | Inferonasal | |
| Hyperlysinemia | Any |
- Anteriorly luxated lens → Pupil block → Acute angle closure glaucoma (emergency - lens extraction/iridotomy)
- Posteriorly luxated lens into vitreous → Phacoanaphylactic uveitis (later)
- Iridodonesis = iris trembling; Phakodonesis = lens trembling (both = zonular weakness)
⭐ PYQ TOPIC 4: CATARACT TYPES WITH SYSTEMIC DISEASE
(2-3 variations every exam cycle)
The PYQ Association Table (Memorize This Completely):
| Disease | Cataract | Mechanism | Trick |
|---|---|---|---|
| Diabetes | Snowflake (young, classic, RARE) / Nuclear sclerosis (old, common) | Aldose reductase: glucose → sorbitol → osmotic hydration | Hyperglycemia → myopia ("fluctuating refraction") |
| Myotonic dystrophy | Iridescent cortical → "Christmas tree" → star-shaped wedge | Multisystem disease | 90% develop cataract |
| Wilson's disease | "Sunflower cataract" | Copper deposition; anterior subcapsular | Also seen in chalcosis (copper IOFB) |
| Atopic dermatitis | "Shield cataract" - anterior subcapsular | Repeated eye rubbing? | Associated with retinal detachment too |
| Hypocalcemia/Hypoparathyroidism | Lamellar/zonular | Low Ca²⁺ → lens opacification | Tetany + cataracts |
| Steroids | Posterior subcapsular | Posterior migration of lens epithelium | Even topical eye drops → PSC |
| Chlorpromazine | Anterior star-shaped (stellate) | Phenothiazine deposition | "Stars at the front" |
| Fabry disease | Spoke-like/propeller (posterior) | X-linked; alpha-galactosidase A | "Cornea verticillata" also |
| Retinitis pigmentosa | Posterior subcapsular | Hereditary fundus dystrophy | Gyrate atrophy, Stickler, Leber also → PSC |
| Infrared (glassblower) | True exfoliation (NOT pseudoexfoliation) | Anterior capsule peels as thin membrane | Heat → anterior capsule delamination |
| Ionizing radiation | Posterior subcapsular | Delayed (months-years) | Radiation therapy for tumors |
| Blunt trauma | Rosette/flower-shaped | Posterior suture opacification | + Vossius ring on anterior capsule |
⭐ PYQ TOPIC 5: CATARACT MATURITY STAGES
(Classic theory MCQ - repeated in image form since 2021)
| Stage | Lens | Iris Shadow | Red Reflex | AC Depth |
|---|---|---|---|---|
| Immature | Partial opacity | Present | Present | Normal |
| Mature | Complete opacity | Absent | Absent | Normal/shallow |
| Hypermature | Shrunken + wrinkled capsule | Absent | Absent | May vary |
| Morgagnian | Liquefied cortex + nucleus sunk inferiorly | Absent | Absent | Normal/deep |
| Intumescent | Swollen (water-logged) | Absent | Absent | Shallow (pupil block risk) |
- Mature → No iris shadow (because lens is fully opaque - no light travels through to cast shadow)
- Morgagnian → Nucleus visible at bottom of liquefied cortex (pathognomonic)
- Intumescent = swollen immature/mature → risk of phacomorphic glaucoma
⭐ PYQ TOPIC 6: LENS-INDUCED GLAUCOMAS
(High yield - mechanism-based questions)
| Type | Stage of Cataract | Angle | Mechanism | Key |
|---|---|---|---|---|
| Phacomorphic | Intumescent/swollen cataract | CLOSED (acute) | Enlarged lens → pupil block → AC angle closure | Emergency - urgent cataract surgery |
| Phacolytic | Hypermature / Mature (leaking) | OPEN | Lens proteins leak → macrophages laden with proteins block TM | High IOP; milky AC flare; absent red reflex |
| Phacoanaphylactic uveitis | After lens rupture/surgery | Variable | Immune reaction to lens proteins → granulomatous uveitis | Mutton-fat KPs |
| Lens particle | Post-trauma / post-surgery | OPEN | Free cortical lens material blocks TM | Corticosteroids + surgery |
| Subluxation-related | Any dislocated lens | Depends | Pupil block by anteriorly displaced lens OR vitreous prolapse |
⭐ PYQ TOPIC 7: CATARACT SURGERY COMPLICATIONS
(Increasingly clinical, image-based since 2022)
Posterior Capsular Opacification (PCO) = "After-Cataract"
- Commonest long-term complication of cataract surgery
- Residual lens epithelial cells migrate posteriorly → Elschnig pearls (bladder/Wedl cells)
- Presents: months to years after surgery with painless gradual visual loss (same as cataract)
- Treatment: Nd:YAG laser posterior capsulotomy (definitive)
- PYQ: "Best treatment for posterior capsular opacification" = Nd:YAG laser
Aphakia Correction:
| Method | Notes |
|---|---|
| Spectacles | +10D convex lens; jack-in-box effect, barrel distortion, ring scotoma; magnification +25-33% |
| Contact lens | Magnification +7%; better than spectacles |
| IOL (intraocular lens) | Gold standard; magnification +1-2%; best visual quality |
Important IOL facts:
- Standard IOL position: In the bag (posterior capsular bag)
- If posterior capsule torn: sulcus fixation or anterior chamber IOL
- Foldable IOL → phacoemulsification (small incision)
- PMMA (rigid) → ECCE (large incision)
- Biometry formulas: SRK/T (standard), Haigis (post-refractive), Holladay
⭐ PYQ TOPIC 8: PRESBYOPIA
(Theory + optics combination question)
- Loss of accommodation due to reduced lens elasticity (hardening of lens nucleus)
- Age of onset: 40-45 years (Indian pop: may be 35-40 years)
- Near point recedes progressively
- Correction: Convex (plus) lens for near work
- Reading glasses: typically +1D at 40 yrs, increasing by ~+0.5D every 5 years
- Not a disease - physiological aging change
- PYQ: "Mechanism of presbyopia" = Loss of lens elasticity (NOT ciliary muscle weakness alone)
⭐ PYQ TOPIC 9: ANTERIOR LENTICONUS - ALPORT SYNDROME
(A classic association question - repeats every 2-3 years)
"Anterior lenticonus is associated with?" Answer: Alport syndrome ✅
- Alport syndrome: X-linked dominant (mostly); COL4A5 mutation → Type IV collagen defect
- Features: Hematuria + Sensorineural deafness + Anterior lenticonus
- Anterior lenticonus → progressive myopia → rupture of anterior capsule → cataract
- Posterior lenticonus: More common; usually sporadic; isolated; causes progressive myopia
⭐ PYQ TOPIC 10: LENS PROTEINS / CRYSTALLINS
(Biochemistry-Ophthalmology crossover - increasingly tested)
- Crystallins = major structural proteins of lens (90% of dry weight)
- Alpha-crystallin = also functions as molecular chaperone (prevents protein aggregation → transparency)
- Beta/gamma crystallins = structural packing proteins
- Lens is avascular and anucleate (mature fibers) - most unique structure in body
- Glucose metabolism: predominantly anaerobic glycolysis (80%) - because avascular
- Sorbitol pathway (aldose reductase): the cause of diabetic cataract
- Glutathione (antioxidant) protects lens; depletion → cataract
🧠 PYQ SIMULATION - SOLVE THESE NOW
📋 RAPID FIRE PYQ RECALL SHEET
"Dandruff on lens" slit lamp → Pseudoexfoliation syndrome
White flaky + Sampaolesi line + poor dilation → Pseudoexfoliation
Oil-droplet cataract + reducing urine → Galactosemia (reversible!)
Newborn dense unilateral cataract → Operate IMMEDIATELY (amblyopia)
Lens UP+OUT → Marfan | Lens DOWN+IN → Homocystinuria
Anterior lenticonus → Alport (hematuria + deafness)
Sunflower cataract → Wilson's disease / chalcosis
Rosette cataract → Blunt trauma
Vossius ring → Blunt trauma (iris pigment ring)
True exfoliation → Glassblower (infrared heat)
PSC → Steroids / Radiation / RP / Fabry
Christmas tree cataract → Myotonic dystrophy
Shield cataract → Atopic dermatitis
Snowflake cataract → Diabetes (young, rare, classic)
Nuclear sclerosis → MOST COMMON diabetes cataract (elderly)
Myopic shift in elderly → Nuclear sclerotic cataract
"Second sight of aged" → Nuclear sclerosis → myopic shift
Morgagnian cataract → Nucleus sinks down
Phacomorphic → Closed angle (swollen lens)
Phacolytic → OPEN angle (leaking hypermature)
Most common complication post-phaco → PCO (after-cataract)
After-cataract treatment → Nd:YAG laser
Aphakic spectacle complication → Ring scotoma
Amblyopia surgery timing (dense unilateral) → Within 6-8 weeks
🏆 EXAM STRATEGY FOR LENS QUESTIONS
- Image questions: If you see white deposits on lens capsule = pseudoexfoliation. If pupil is white (leukocoria) = cataract/retinoblastoma/PFV - look for age and laterality.
- Clinical scenario questions: Age of patient + laterality + associated systemic features = the key to correct diagnosis.
- "Management" questions: Surgical timing for congenital cataract = always appears. Answer = immediate/urgent.
- Mechanism questions: Phacomorphic vs Phacolytic = must distinguish by angle status.
- Drug association questions: Steroid → PSC (Posterior). Chlorpromazine → Anterior star.
Create a flashcard deck of lens-related MCQs with detailed explanations for NEET PG
ls /home/daytona/workspace/ 2>/dev/null && echo "---" && node --version
mkdir -p /home/daytona/workspace/lens-flashcards && ls /home/daytona/workspace/l…
~/lens-flashcards/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Lens MCQ Flashcards - NEET PG 2026";
pres.author = "Orris Medical Mentor";
// ─── COLOR PALETTE ─────────────────────────────────────
const C = {
darkBg: "0D1B2A", // deep navy - question slides
answerBg: "1B3A2D", // deep green - answer slides
coverBg: "0D1B2A",
accent: "F5A623", // amber
correct: "4CAF50", // green
white: "FFFFFF",
lightGrey: "D0D8E0",
softGold: "FFD580",
optionBg: "162232", // slightly lighter navy for option boxes
wrongOpt: "1E2D3D",
rightOpt: "1B3A2D",
tagBg: "1C2F45",
};
// ─── MCQ DATA ───────────────────────────────────────────
// Each card: { id, tag, question, options:[A,B,C,D], answer:"A"|"B"|"C"|"D", explanation, memory }
const cards = [
{
id: 1,
tag: "Embryology",
question: "The crystalline lens develops from which embryological layer?",
options: [
"A. Neural ectoderm",
"B. Surface ectoderm",
"C. Mesoderm",
"D. Neural crest cells"
],
answer: "B",
explanation: "The lens develops from the SURFACE ECTODERM via the lens placode → lens pit → lens vesicle sequence. Neural ectoderm forms the retina and optic nerve. Neural crest cells form the stroma of the cornea and uveal tissues. This is a classic embryology MCQ that repeats every 2-3 years.",
memory: "\"Surface → See → Lens\" — the lens is for SEEING and comes from SURFACE ectoderm"
},
{
id: 2,
tag: "Embryology",
question: "The adult lens receives its nutrition from which source?",
options: [
"A. Hyaloid artery",
"B. Central retinal artery",
"C. Aqueous humor (diffusion)",
"D. Ciliary arteries"
],
answer: "C",
explanation: "The adult lens is AVASCULAR and anuclleate (mature fibers). During development, it receives blood from the hyaloid artery via the tunica vasculosa lentis. After the hyaloid artery degenerates in the fetal period, the lens depends entirely on DIFFUSION from aqueous humor (anterior) and vitreous humor (posterior). This makes it metabolically unique — predominantly anaerobic glycolysis.",
memory: "No vessels, no nerves — lens lives on 'aqueous room service' (diffusion)"
},
{
id: 3,
tag: "Anatomy",
question: "Which part of the lens capsule is the THINNEST?",
options: [
"A. Anterior pole",
"B. Anterior equator",
"C. Posterior pole",
"D. Equatorial zone"
],
answer: "C",
explanation: "The POSTERIOR POLE of the lens capsule is the thinnest (~2–4 μm). The anterior capsule near the equator is the thickest (~14 μm). This is clinically crucial: during cataract surgery, the posterior capsule is most vulnerable to rupture. Phacoemulsification is designed to PRESERVE the posterior capsule for IOL support. PCO (after-cataract) occurs when residual cells populate this retained capsule.",
memory: "POSTERIOR = thinnest. Surgeons fear posterior capsule rupture most!"
},
{
id: 4,
tag: "Anatomy / Histology",
question: "The lens epithelium (subcapsular epithelium) is present on which surface of the lens?",
options: [
"A. Anterior surface only",
"B. Posterior surface only",
"C. Both anterior and posterior surfaces",
"D. Only at the equator"
],
answer: "A",
explanation: "Lens epithelium exists ONLY on the ANTERIOR surface — a single layer of cuboidal cells beneath the anterior capsule. There is NO epithelium on the posterior surface. The germinative zone (equatorial region of this anterior epithelium) is where cells divide continuously to form new lens fibers. This is why anterior subcapsular cataract involves fibrous metaplasia of these epithelial cells.",
memory: "One-sided: epithelium on ANTERIOR only. Posterior = naked capsule."
},
{
id: 5,
tag: "Physiology",
question: "A 45-year-old teacher notices difficulty reading the blackboard while wearing reading glasses. She requires a change in spectacle prescription every year. This condition is most likely due to?",
options: [
"A. Increasing myopia",
"B. Ciliary muscle spasm",
"C. Progressive loss of lens elasticity",
"D. Zonular laxity"
],
answer: "C",
explanation: "This is PRESBYOPIA. The primary mechanism is progressive loss of LENS ELASTICITY as the lens nucleus hardens (nuclear sclerosis) — the lens can no longer increase its curvature for near vision. Ciliary muscle weakness may contribute but is secondary. Zonular laxity would cause lens dislocation, not presbyopia. Onset is typically 40–45 years; treatment is convex (+) reading glasses.",
memory: "Presbyopia = 'Old eye' in Greek. Hard lens = can't squeeze for near = needs PLUS lens"
},
{
id: 6,
tag: "Physiology",
question: "A diabetic patient presents with sudden onset of blurred distance vision after a period of very high blood sugar. His glasses that usually help for distance now make vision worse. What is the mechanism?",
options: [
"A. Diabetic retinopathy",
"B. Hyperglycemia → sorbitol → myopic shift",
"C. Macular edema",
"D. Cataract formation"
],
answer: "B",
explanation: "Hyperglycemia → excess glucose enters the lens → converted by ALDOSE REDUCTASE to SORBITOL → sorbitol accumulates (impermeable to cell membrane) → OSMOTIC OVERHYDRATION of lens fibers → increased refractive index of nucleus → MYOPIC SHIFT. This causes sudden blurred distance vision. Distance glasses now over-correct. With hypoglycemia, the opposite occurs (hypermetropic shift). This classic 'fluctuating refraction' in diabetics is tested frequently.",
memory: "HIGH sugar → sorbitol → swollen lens → MYOPIA. LOW sugar → shrunk lens → HYPERMETROPIA"
},
{
id: 7,
tag: "Age-related Cataract",
question: "Which type of age-related cataract causes the WORST visual symptoms in bright light and during near work, despite relatively preserved distance visual acuity?",
options: [
"A. Nuclear sclerotic cataract",
"B. Cortical cataract",
"C. Posterior subcapsular cataract (PSC)",
"D. Anterior subcapsular cataract"
],
answer: "C",
explanation: "POSTERIOR SUBCAPSULAR CATARACT (PSC) is located at the nodal point of the eye. It causes: (1) Severe GLARE in bright light / oncoming headlights, (2) Worsened vision in MIOSIS (near work, bright sunlight — pupil constricts exposing the central opacity), (3) Disproportionately poor vision despite relatively preserved distant acuity. PSC is associated with steroids, radiation, diabetes, and retinitis pigmentosa. The vacuolated bladder (Wedl) cells on retroillumination are pathognomonic.",
memory: "PSC = worst in BRIGHT LIGHT and NEAR WORK = 'pupil shrinks, exposing the opacity'"
},
{
id: 8,
tag: "Age-related Cataract",
question: "An elderly patient with nuclear sclerotic cataract says he can now read his newspaper without glasses for the first time in years. This phenomenon is called?",
options: [
"A. Accommodation recovery",
"B. Second sight of the aged",
"C. Pseudoaccommodation",
"D. Miotic pupil effect"
],
answer: "B",
explanation: "'SECOND SIGHT OF THE AGED' — Nuclear sclerosis increases the refractive index of the lens nucleus, causing a MYOPIC SHIFT. Patients who were previously hypermetropic (needing reading glasses) find they can suddenly read without glasses. However, distance vision worsens. This is temporary — as the cataract progresses, all vision declines. This is a classic NEET PG trap: it sounds like vision is improving, but the lens is becoming more cataractous.",
memory: "Nuclear sclerosis → MYOPIA → hypermetrope reads again → 'Second Sight' — but it's still a cataract!"
},
{
id: 9,
tag: "Cataract Maturity",
question: "In which stage of cataract maturity does the IRIS SHADOW test become NEGATIVE (absent shadow)?",
options: [
"A. Immature cataract",
"B. Mature cataract",
"C. Only Morgagnian cataract",
"D. Hypermature cataract"
],
answer: "B",
explanation: "The iris shadow test: a light is shone obliquely on the eye. In IMMATURE cataract (partially opaque), light passing through the clear anterior portion casts a SHADOW of the iris on the opaque posterior portion — POSITIVE shadow. In MATURE cataract (completely opaque), no light can pass through — NO SHADOW (NEGATIVE). In Morgagnian and hypermature cataracts, shadow is also absent. The iris shadow test differentiates mature from immature clinically without instruments.",
memory: "IMMATURE = shadow PRESENT (clear part allows light). MATURE = shadow ABSENT (full opacity)"
},
{
id: 10,
tag: "Cataract Maturity",
question: "A hypermature cataract in which the cortex has liquefied and the nucleus has sunk to the bottom is called?",
options: [
"A. Intumescent cataract",
"B. Morgagnian cataract",
"C. Brunescent cataract",
"D. Mature cataract"
],
answer: "B",
explanation: "MORGAGNIAN CATARACT is a hypermature cataract where the cortex has completely liquefied (milky white fluid), and the brown-black sclerotic nucleus sinks INFERIORLY under gravity. It appears as a dark nucleus floating at the bottom of a white lens. This is one of the most visually striking and high-yield cataract images in NEET PG. Intumescent = swollen (early mature/immature). Brunescent = brown-colored nucleus (advanced nuclear sclerosis).",
memory: "MORGAGNIAN = Morgan's cataract (the nucleus 'drowns' in liquefied cortex and sinks)"
},
{
id: 11,
tag: "Systemic Associations",
question: "A 25-year-old presents with bilateral posterior subcapsular cataract and is found to have haematuria and bilateral sensorineural hearing loss. Slit lamp shows a forward protrusion of the anterior lens surface. Diagnosis?",
options: [
"A. Marfan syndrome",
"B. Alport syndrome",
"C. Homocystinuria",
"D. Lowe syndrome"
],
answer: "B",
explanation: "ALPORT SYNDROME triad: (1) HAEMATURIA (glomerulonephritis — Type IV collagen defect in GBM), (2) SENSORINEURAL DEAFNESS, (3) ANTERIOR LENTICONUS (forward conical protrusion of anterior lens surface → progressive myopia → cataract). X-linked dominant (COL4A5 mutation). Marfan: lens dislocation upward. Homocystinuria: lens dislocation downward + thromboembolism. Lowe: X-linked, amino aciduria + intellectual disability + cataract.",
memory: "ALPORT: 'A-E-I' — Anterior lenticonus, Ears (deafness), hematUrIa (blood in urine)"
},
{
id: 12,
tag: "Systemic Associations",
question: "Sunflower cataract is MOST CHARACTERISTICALLY seen in which condition?",
options: [
"A. Diabetes mellitus",
"B. Wilson's disease",
"C. Myotonic dystrophy",
"D. Atopic dermatitis"
],
answer: "B",
explanation: "SUNFLOWER CATARACT — a disc-shaped, greenish-brown anterior subcapsular opacity with petal-like extensions — is pathognomonic of WILSON'S DISEASE (hepatolenticular degeneration). Copper deposition in the lens creates this pattern. It is also seen in CHALCOSIS (copper IOFB — intraocular foreign body). Wilson's also shows Kayser-Fleischer rings (copper in Descemet's membrane of cornea). The cataract is visible on slit lamp but does not significantly impair vision usually.",
memory: "Wilson's = 'Wilson SUNFLOWER' + KF rings. Copper deposits make 'flower patterns'"
},
{
id: 13,
tag: "Systemic Associations",
question: "Classic 'snowflake' cortical cataract in a 22-year-old is most closely associated with?",
options: [
"A. Steroid therapy",
"B. Diabetes mellitus",
"C. Myotonic dystrophy",
"D. Hypoparathyroidism"
],
answer: "B",
explanation: "CLASSIC DIABETIC CATARACT (snowflake/stellate cortical opacities) occurs in YOUNG diabetics and may mature within a few DAYS — this is the classic/textbook diabetic cataract. It is actually RARE. The COMMON diabetic cataract is nuclear sclerosis in the elderly. Mechanism: glucose → aldose reductase → sorbitol → osmotic cortical vacuoles → frank snowflake opacities. This is a 'classic' question that tests whether you know the difference between the CLASSIC (rare, young) and COMMON (nuclear, elderly) forms.",
memory: "SNOWFLAKE cataract → Young DIABETIC → Classic form (RARE but heavily tested!)"
},
{
id: 14,
tag: "Systemic Associations",
question: "A patient on long-term systemic steroids for nephrotic syndrome develops cataract. Which type is MOST LIKELY?",
options: [
"A. Nuclear sclerotic",
"B. Anterior subcapsular",
"C. Posterior subcapsular (PSC)",
"D. Cortical wedge-shaped"
],
answer: "C",
explanation: "STEROID-INDUCED CATARACT is ALWAYS POSTERIOR SUBCAPSULAR (PSC) — regardless of route (oral, topical eye drops, inhaled). Mechanism: steroids may affect lens epithelial cell metabolism and cause posterior migration of lens epithelial cells → PSC. The PSC due to steroids is characteristically visually debilitating (at the nodal point), causing severe glare and near vision problems. Duration and dose of steroid use correlate with risk. This is one of the most frequently repeated drug-cataract associations.",
memory: "STEROID → PSC (Posterior SubCapsular). S-S: Steroid → Subcapsular Posterior"
},
{
id: 15,
tag: "Drug-induced Cataract",
question: "Long-term chlorpromazine use leads to which type of cataract?",
options: [
"A. Posterior subcapsular",
"B. Anterior star-shaped (stellate) opacity",
"C. Nuclear brunescent",
"D. Cortical spoke-like"
],
answer: "B",
explanation: "CHLORPROMAZINE (a phenothiazine antipsychotic) causes a characteristic ANTERIOR STAR-SHAPED (stellate) opacity in the anterior lens capsule and anterior cortex. Phenothiazines deposit pigment granules in exposed tissues (lens, cornea, skin). This is opposite to steroids (PSC). Memory hook: 'Chlor = CLEAR FRONT gets stars.' Other phenothiazines (thioridazine) affect the RETINA. Long-term miotics like echothiophate can also cause anterior subcapsular cataract.",
memory: "ChlorPROMazine = FRONT (anterior) STAR. Steroid = BACK (posterior) subcapsular."
},
{
id: 16,
tag: "Traumatic Cataract",
question: "A 30-year-old cricketer is hit by a ball on the eye. Slit lamp shows a ring-shaped brownish-red deposit on the anterior lens capsule. What is this called?",
options: [
"A. Rosette cataract",
"B. Vossius ring",
"C. Sunflower cataract",
"D. True exfoliation"
],
answer: "B",
explanation: "VOSSIUS RING — a ring-shaped opacity on the anterior lens capsule at the pupillary margin, resulting from blunt ocular trauma. The iris pigment and uveal tissue are imprinted onto the anterior lens surface at the moment of impact (the iris is crushed against the lens). It is brownish-red due to pigment. It does not significantly affect vision. Rosette cataract = flower/stellate shaped opacity at the posterior sutures (also from blunt trauma). Both are classic traumatic cataract patterns.",
memory: "VOSSIUS RING = 'iris stamp' on lens after blunt hit. Ring-shaped = iris outline."
},
{
id: 17,
tag: "Traumatic Cataract",
question: "A glassblower develops a condition where a thin membrane peels off the ANTERIOR LENS CAPSULE. This is known as?",
options: [
"A. Pseudoexfoliation",
"B. True exfoliation (capsular delamination)",
"C. Phacomorphic change",
"D. Anterior subcapsular cataract"
],
answer: "B",
explanation: "TRUE EXFOLIATION (capsular delamination) — intense INFRARED RADIATION (as in glassblowers, iron foundry workers) causes a thin lamellar sheet to peel off the anterior lens capsule. This is distinct from PSEUDOEXFOLIATION, which is a systemic fibrillopathy where abnormal extracellular material (NOT the capsule itself) is deposited on the lens surface. Glaucoma is UNCOMMON with true exfoliation. True exfoliation can also occur with severe uveitis or trauma.",
memory: "TRUE exfoliation = CAPSULE PEELS (glassblower, heat). PSEUDO exfoliation = dandruff deposits ON capsule."
},
{
id: 18,
tag: "Pseudoexfoliation",
question: "An elderly patient has 'white dandruff-like material' on the anterior lens capsule in a target pattern on slit lamp. Gonioscopy shows Sampaolesi line. What is the MOST LIKELY glaucoma type associated?",
options: [
"A. Primary angle closure glaucoma",
"B. Pigmentary glaucoma",
"C. Pseudoexfoliative (exfoliative) glaucoma",
"D. Neovascular glaucoma"
],
answer: "C",
explanation: "PSEUDOEXFOLIATION SYNDROME is the COMMONEST identifiable cause of open-angle glaucoma worldwide. Features: (1) White flaky material in target pattern on anterior lens capsule (central disc + clear zone + peripheral ring), (2) Sampaolesi line on gonioscopy (pigment anterior to Schwalbe line), (3) Poor pupil dilation, (4) Zonular weakness → difficult cataract surgery. The associated glaucoma (pseudoexfoliative/exfoliative glaucoma) is an open-angle type with very HIGH, fluctuating IOP — often hardest to control medically.",
memory: "PEX = 'Dandruff on lens + Sampaolesi line + Open angle glaucoma' — the triad!"
},
{
id: 19,
tag: "Lens Dislocation",
question: "A 16-year-old tall boy with arachnodactyly, pectus excavatum, and aortic root dilatation is found to have bilateral lens dislocation. In which direction has the lens most likely dislocated?",
options: [
"A. Inferonasal",
"B. Inferotemporal",
"C. Superotemporal (up and out)",
"D. Directly downward"
],
answer: "C",
explanation: "MARFAN SYNDROME — autosomal dominant, FBN1 gene, fibrillin-1 defect → weak zonular fibers → bilateral lens dislocation SUPEROTEMPORAL (upward and outward) in ~60–70% of cases. Associated features: tall stature, arachnodactyly, pectus deformity, aortic root dilatation (risk of aortic dissection), mitral valve prolapse. The lens dislocation direction is the most repeated Marfan MCQ. Remember: Marfan = UPWARD. Homocystinuria = DOWNWARD.",
memory: "MAR-FAN = Fans above = Lens goes UP (superotemporal). FAN the sky upward!"
},
{
id: 20,
tag: "Lens Dislocation",
question: "A 20-year-old with lens dislocation undergoes elective surgery. Post-op he develops massive pulmonary embolism. Which diagnosis should have been screened for pre-operatively?",
options: [
"A. Marfan syndrome",
"B. Weill-Marchesani syndrome",
"C. Homocystinuria",
"D. Aniridia"
],
answer: "C",
explanation: "HOMOCYSTINURIA (CBS gene defect, autosomal recessive) — the lens dislocates INFERONASAL (down and inward). The CRITICAL distinguishing feature is a HIGH RISK OF THROMBOEMBOLIC EVENTS (DVT, pulmonary embolism, stroke) due to abnormal homocysteine causing endothelial damage and platelet aggregation. General anesthesia and surgery should be done with anticoagulation prophylaxis. Also: intellectual disability, marfanoid habitus, fair hair/skin (unlike Marfan). Diet: methionine-restricted + pyridoxine (B6) supplementation.",
memory: "HOMOCYSTINURIA = DOWNWARD lens + THROMBOSIS risk. 'Goes DOWN, blood CLOTS UP'"
},
{
id: 21,
tag: "Congenital Cataract",
question: "A 6-week-old infant has a unilateral dense white cataract (leukocoria). The most important principle guiding the timing of surgery is?",
options: [
"A. Prevent glaucoma",
"B. Prevent amblyopia",
"C. Wait until child can tolerate GA safely",
"D. Correct associated systemic disease first"
],
answer: "B",
explanation: "PREVENTION OF AMBLYOPIA is the critical driving force for urgent surgery in congenital cataract. Dense unilateral cataract deprives the visual cortex of patterned visual input during the critical period of visual development (first weeks to months of life) → STIMULUS DEPRIVATION AMBLYOPIA. This amblyopia is permanent if the cataract is not removed early. Surgery should be done within 6–8 weeks. After surgery, the child needs optical correction (contact lens preferred) AND aggressive patching of the fellow eye to force use of the amblyopic eye.",
memory: "Congenital cataract URGENCY = 'Race against AMBLYOPIA clock' — operate before cortex is wired wrong"
},
{
id: 22,
tag: "Congenital Cataract",
question: "Which congenital cataract is REVERSIBLE with dietary modification?",
options: [
"A. Rubella cataract",
"B. Galactosemia (galactose-1-P uridyltransferase deficiency)",
"C. Lowe syndrome",
"D. Down syndrome cataract"
],
answer: "B",
explanation: "GALACTOSEMIA cataract (Type I — galactose-1-phosphate uridyltransferase deficiency) — excess galactose is converted by aldose reductase to GALACTITOL, which accumulates in the lens → oil-droplet cataract. If detected early and treated with a GALACTOSE-FREE DIET, the cataract can REGRESS. This makes it unique among congenital cataracts. Galactokinase deficiency (Type II, milder) also causes oil-droplet cataract (cataracts only, no systemic effects). Rubella, Lowe, and Down syndrome cataracts are NOT reversible.",
memory: "GALACTOSEMIA = 'Galactose-free diet = cataract dissolves' — the ONLY reversible congenital cataract!"
},
{
id: 23,
tag: "Lens-Related Glaucoma",
question: "A patient with a mature cataract presents with sudden painful red eye, nausea, corneal edema, and IOP of 54 mmHg. Gonioscopy shows CLOSED angle. What is the diagnosis?",
options: [
"A. Phacolytic glaucoma",
"B. Phacomorphic glaucoma",
"C. Acute primary angle closure glaucoma",
"D. Neovascular glaucoma"
],
answer: "B",
explanation: "PHACOMORPHIC GLAUCOMA — the intumescent (swollen) or large mature cataract pushes the iris-lens diaphragm forward → PUPIL BLOCK → acute angle CLOSURE glaucoma. Key: CLOSED ANGLE on gonioscopy. Clinical features identical to acute angle closure: severe pain, redness, corneal oedema, nausea, fixed mid-dilated pupil, IOP >40. Treatment: URGENT cataract extraction (definitive) + medical management to lower IOP before surgery. This is an ophthalmic emergency. Do NOT confuse with phacolytic (OPEN angle).",
memory: "PhacoMORPHIC = lens MORPHOLOGY (big/swollen) → CLOSES the angle. Emergency!"
},
{
id: 24,
tag: "Lens-Related Glaucoma",
question: "A hypermature cataract patient presents with gradual painless loss of vision, IOP 42 mmHg, white fluff in anterior chamber, and macrophages on gonioscopy blocking the trabecular meshwork. Angle is OPEN. Diagnosis?",
options: [
"A. Phacomorphic glaucoma",
"B. Phacolytic glaucoma",
"C. Phacoanaphylactic uveitis",
"D. Ghost cell glaucoma"
],
answer: "B",
explanation: "PHACOLYTIC GLAUCOMA — hypermature/mature cataract leaks lens proteins through the intact capsule. These high-molecular-weight proteins → macrophages engulf them → macrophage-protein complexes BLOCK the TRABECULAR MESHWORK → OPEN angle glaucoma (very high IOP). Signs: white fluff/milky flakes in AC, macrophages on gonioscopy, no cells/flare of uveitis (unlike phacoanaphylactic). Painless progressive IOP rise. Treatment: URGENT cataract extraction. Phacoanaphylactic uveitis = granulomatous UVEITIS after lens rupture (mutton-fat KPs).",
memory: "PhacoLYTIC = lens LEAKS (lysis) → proteins → macrophages → OPEN angle. Painless, gradual."
},
{
id: 25,
tag: "Cataract Surgery",
question: "What is the MOST COMMON late complication of phacoemulsification with IOL implantation?",
options: [
"A. IOL dislocation",
"B. Cystoid macular edema",
"C. Posterior capsular opacification (PCO)",
"D. Endophthalmitis"
],
answer: "C",
explanation: "POSTERIOR CAPSULAR OPACIFICATION (PCO) — also called 'after-cataract' or 'secondary cataract' — is the MOST COMMON late complication of cataract surgery. Residual lens epithelial cells (from the germinative zone) migrate posteriorly and populate the retained posterior capsule → form Elschnig pearls (bladder/Wedl cells) → PCO. Presents: months to years post-op with painless gradual visual loss (identical to original cataract). Treatment: Nd:YAG LASER posterior capsulotomy (quick, outpatient, definitive). Endophthalmitis is most feared early complication (not late).",
memory: "PCO = 'cataract comes back ghost' on the retained capsule. Treat with YAG LASER."
},
{
id: 26,
tag: "Cataract Surgery",
question: "After uncomplicated cataract surgery, a patient is left aphakic (no IOL placed). What is the POWER of the corrective spectacle lens needed, and what is its most significant complication?",
options: [
"A. +3D; myopia induced",
"B. +10D; ring scotoma",
"C. +10D; barrel distortion only",
"D. −10D; ring scotoma"
],
answer: "B",
explanation: "APHAKIC SPECTACLES require approximately +10 DIOPTERS (convex) to compensate for the missing lens. Complications: (1) RING SCOTOMA — an annular blind area at ~20–30° from fixation, caused by the prismatic edge effect of the thick convex lens; (2) JACK-IN-BOX PHENOMENON — objects suddenly appear and disappear at the edges; (3) Image magnification of +25–33% — causes diplopia if only one eye is aphakic (aniseikonia); (4) Barrel distortion. The ring scotoma is the most clinically significant and frequently tested complication.",
memory: "+10D for aphakia. RING SCOTOMA is the trap complication! Objects 'disappear' at periphery."
},
{
id: 27,
tag: "Microspherophakia",
question: "A 15-year-old short-statured child with short stubby fingers presents with myopia and bilateral small spherical lenses. On mydriasis the equator of the lens is visible. The lens occasionally slips anteriorly causing angle closure. Diagnosis?",
options: [
"A. Marfan syndrome",
"B. Weill-Marchesani syndrome",
"C. Homocystinuria",
"D. Alport syndrome"
],
answer: "B",
explanation: "WEILL-MARCHESANI SYNDROME — autosomal recessive or dominant. The INVERSE of Marfan: SHORT stature, BRACHYDACTYLY (short stubby fingers), MICROSPHEROPHAKIA (small spherical lens) causing HIGH MYOPIA, and lens dislocation (usually inferiorly). The small spherical lens can dislocate anteriorly through the pupil → PUPIL BLOCK → angle closure glaucoma. Treatment of acute attack: PRONE POSITIONING (lets lens fall back), mydriatics (dilate to prevent pupil block), then lens extraction. Miotic drops are CONTRAINDICATED (worsen pupil block).",
memory: "Weill-Marchesani = ANTI-Marfan: SHORT + stubby + spherical lens. Miosis = DANGER here!"
},
{
id: 28,
tag: "Lens Proteins",
question: "Fabry disease (alpha-galactosidase A deficiency) produces which SPECIFIC lens finding?",
options: [
"A. Sunflower cataract",
"B. Oil-droplet cataract",
"C. Posterior spoke-like (propeller/whorl) opacity",
"D. Anterior shield cataract"
],
answer: "C",
explanation: "FABRY DISEASE (X-linked recessive, alpha-galactosidase A deficiency) → glycolipid (ceramide trihexoside) deposition in tissues. Ocular findings: (1) CORNEA VERTICILLATA — whorl-like corneal opacity (most common), (2) POSTERIOR LENS SPOKE-LIKE/PROPELLER OPACITY (specific to Fabry). The lens opacity has a distinctive radiating spoke or propeller configuration in the posterior subcapsular region. Males (hemizygous) show full features. Also: painful crises, angiokeratomas, renal failure, cardiac disease. Treatment: enzyme replacement therapy.",
memory: "FABRY = 'Verticillata (cornea whorl) + Propeller (lens)' — a spinning theme!"
},
{
id: 29,
tag: "Congenital Anomalies",
question: "Persistent hyperplastic primary vitreous (PHPV) / Persistent Fetal Vasculature (PFV) typically presents as?",
options: [
"A. Bilateral cataracts in a premature infant",
"B. Unilateral leukocoria with microphthalmia in a full-term infant",
"C. Bilateral lens dislocation",
"D. Bilateral lens coloboma"
],
answer: "B",
explanation: "PERSISTENT FETAL VASCULATURE (PFV) / PHPV — failure of regression of the primary vitreous (hyaloid vascular system). Presents as: (1) UNILATERAL leukocoria (white pupillary reflex — must be differentiated from retinoblastoma!), (2) MICROPHTHALMIA (small eye), (3) Full-term infant (not premature — unlike retinopathy of prematurity). On examination: white fibrovascular membrane behind the lens, often with an elongated ciliary process. Retinoblastoma is bilateral in 40%, no microphthalmia, hard white mass on CT. PHPV/PFV: unilateral, small eye, fibrovascular stalk.",
memory: "PFV = Unilateral leukocoria + SMALL EYE (microphthalmia) = failed hyaloid regression"
},
{
id: 30,
tag: "Lens Coloboma / Embryology",
question: "Coloboma of the lens (notch in the lens) is located in which quadrant?",
options: [
"A. Superotemporal",
"B. Inferonasal",
"C. Superonasal",
"D. Inferotemporal"
],
answer: "B",
explanation: "LENS COLOBOMA is located in the INFERONASAL quadrant because it results from incomplete closure of the EMBRYONIC FETAL FISSURE (optic fissure), which is located inferonasal. The same mechanism causes colobomas of the iris, choroid, optic disc, and retina — all inferonasal. The lens coloboma appears as a flat notch or indentation at the equator of the lens, inferonasally. Clinically: the zonular fibers are absent in that area. Associated with various systemic syndromes. This is an anatomy-embryology crossover MCQ.",
memory: "ALL colobomas = INFERONASAL = fetal fissure fails to close. Lens, iris, choroid, disc — all inferonasal!"
}
];
// ─── HELPER FUNCTIONS ───────────────────────────────────
function addCoverSlide(pres) {
const slide = pres.addSlide();
// Background
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: C.darkBg }
});
// Decorative top bar
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 0.08,
fill: { color: C.accent }
});
// Decorative bottom bar
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 5.545, w: 10, h: 0.08,
fill: { color: C.accent }
});
// Left accent strip
slide.addShape(pres.ShapeType.rect, {
x: 0.35, y: 1.1, w: 0.08, h: 3.4,
fill: { color: C.accent }
});
// Eye/lens icon circle (decorative)
slide.addShape(pres.ShapeType.ellipse, {
x: 7.5, y: 0.9, w: 2.1, h: 2.1,
fill: { color: C.optionBg },
line: { color: C.accent, width: 2 }
});
slide.addShape(pres.ShapeType.ellipse, {
x: 8.1, y: 1.5, w: 0.9, h: 0.9,
fill: { color: C.accent }
});
slide.addText("LENS", {
x: 0.6, y: 1.1, w: 6.5, h: 0.8,
fontSize: 52, bold: true, color: C.accent,
fontFace: "Calibri", margin: 0
});
slide.addText("MCQ FLASHCARD DECK", {
x: 0.6, y: 1.85, w: 6.5, h: 0.65,
fontSize: 22, bold: true, color: C.white,
fontFace: "Calibri", charSpacing: 4, margin: 0
});
slide.addShape(pres.ShapeType.rect, {
x: 0.6, y: 2.7, w: 4.5, h: 0.06,
fill: { color: C.lightGrey }
});
slide.addText("NEET PG 2026 | 30 PYQ-Based Questions | Ophthalmology", {
x: 0.6, y: 2.85, w: 8.5, h: 0.45,
fontSize: 13, color: C.lightGrey,
fontFace: "Calibri", margin: 0
});
slide.addText([
{ text: "Topics Covered: ", options: { bold: true, color: C.softGold } },
{ text: "Embryology • Anatomy • Physiology • Age-related Cataract • Systemic Associations", options: { color: C.lightGrey } }
], {
x: 0.6, y: 3.4, w: 9, h: 0.5,
fontSize: 11.5, fontFace: "Calibri", margin: 0
});
slide.addText([
{ text: "Traumatic Cataract • Drug-induced • Pseudoexfoliation • Lens Dislocation • Surgery", options: { color: C.lightGrey } }
], {
x: 0.6, y: 3.82, w: 9, h: 0.45,
fontSize: 11.5, fontFace: "Calibri", margin: 0
});
slide.addText([
{ text: "Lens-Induced Glaucoma • Congenital Anomalies • Flashcard Format (Q → Answer)", options: { color: C.lightGrey } }
], {
x: 0.6, y: 4.2, w: 9, h: 0.45,
fontSize: 11.5, fontFace: "Calibri", margin: 0
});
slide.addText("Orris Medical Mentor | NEET PG 2026", {
x: 0.6, y: 5.1, w: 8, h: 0.3,
fontSize: 9.5, color: "6A7F95",
fontFace: "Calibri", margin: 0
});
}
function addQuestionSlide(pres, card) {
const slide = pres.addSlide();
// Full background
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: C.darkBg }
});
// Top bar
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 0.06,
fill: { color: C.accent }
});
// Tag pill
slide.addShape(pres.ShapeType.roundRect, {
x: 0.4, y: 0.18, w: 2.0, h: 0.38,
fill: { color: C.tagBg },
line: { color: C.accent, width: 1 },
rectRadius: 0.1
});
slide.addText(card.tag.toUpperCase(), {
x: 0.4, y: 0.18, w: 2.0, h: 0.38,
fontSize: 8.5, bold: true, color: C.accent,
align: "center", valign: "middle",
fontFace: "Calibri", margin: 0
});
// Q number
slide.addText(`Q${card.id}`, {
x: 8.8, y: 0.13, w: 0.9, h: 0.46,
fontSize: 14, bold: true, color: "4A6580",
align: "right", fontFace: "Calibri", margin: 0
});
// Question
const questionLines = card.question.length > 110 ? 1.05 : 0.85;
slide.addText(card.question, {
x: 0.35, y: 0.72, w: 9.3, h: questionLines,
fontSize: 14.5, bold: true, color: C.white,
fontFace: "Calibri", wrap: true, margin: 0
});
// Options
const optY = [1.85, 2.58, 3.31, 4.04];
const optColors = [C.optionBg, C.optionBg, C.optionBg, C.optionBg];
card.options.forEach((opt, i) => {
// Option box
slide.addShape(pres.ShapeType.roundRect, {
x: 0.35, y: optY[i], w: 9.3, h: 0.58,
fill: { color: optColors[i] },
line: { color: "2A3F55", width: 0.75 },
rectRadius: 0.07
});
slide.addText(opt, {
x: 0.55, y: optY[i], w: 9.0, h: 0.58,
fontSize: 12.5, color: C.lightGrey,
fontFace: "Calibri", valign: "middle", margin: 0, wrap: true
});
});
// Flip prompt at bottom
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 5.35, w: 10, h: 0.275,
fill: { color: "091523" }
});
slide.addText("▶ Next slide for Answer & Explanation", {
x: 0, y: 5.35, w: 10, h: 0.275,
fontSize: 9, color: "4A6580",
align: "center", valign: "middle",
fontFace: "Calibri", margin: 0
});
}
function addAnswerSlide(pres, card) {
const slide = pres.addSlide();
// Full background
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: C.answerBg }
});
// Top bar
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 0.06,
fill: { color: C.correct }
});
// Left stripe
slide.addShape(pres.ShapeType.rect, {
x: 0, y: 0.06, w: 0.2, h: 5.565,
fill: { color: C.correct }
});
// Answer header
slide.addText("ANSWER", {
x: 0.4, y: 0.1, w: 2.5, h: 0.42,
fontSize: 9, bold: true, color: C.correct,
charSpacing: 5, fontFace: "Calibri", margin: 0
});
slide.addText(`Q${card.id} | ${card.tag}`, {
x: 5.0, y: 0.1, w: 4.8, h: 0.42,
fontSize: 9, color: "5A8070",
align: "right", fontFace: "Calibri", margin: 0
});
// Correct option label
slide.addShape(pres.ShapeType.roundRect, {
x: 0.4, y: 0.65, w: 9.2, h: 0.62,
fill: { color: "1E4D35" },
line: { color: C.correct, width: 1.5 },
rectRadius: 0.08
});
// find full option text for correct answer
const correctLetter = card.answer; // "A", "B", "C", "D"
const correctIdx = ["A","B","C","D"].indexOf(correctLetter);
const correctText = card.options[correctIdx];
slide.addText([
{ text: "✓ ", options: { bold: true, color: C.correct, fontSize: 15 } },
{ text: correctText, options: { bold: true, color: C.softGold, fontSize: 13.5 } }
], {
x: 0.55, y: 0.65, w: 9.0, h: 0.62,
fontFace: "Calibri", valign: "middle", margin: 0, wrap: true
});
// Explanation header
slide.addText("EXPLANATION", {
x: 0.4, y: 1.42, w: 3, h: 0.3,
fontSize: 8.5, bold: true, color: "5A9E80",
charSpacing: 3, fontFace: "Calibri", margin: 0
});
slide.addShape(pres.ShapeType.rect, {
x: 0.4, y: 1.7, w: 9.2, h: 0.02,
fill: { color: "2A5040" }
});
// Explanation text
slide.addText(card.explanation, {
x: 0.4, y: 1.78, w: 9.2, h: 2.6,
fontSize: 11, color: C.lightGrey,
fontFace: "Calibri", wrap: true, valign: "top", margin: 0
});
// Memory hook section
slide.addShape(pres.ShapeType.roundRect, {
x: 0.4, y: 4.52, w: 9.2, h: 0.82,
fill: { color: "162832" },
line: { color: C.softGold, width: 1 },
rectRadius: 0.07
});
slide.addText([
{ text: "💡 Memory Hook: ", options: { bold: true, color: C.softGold, fontSize: 10.5 } },
{ text: card.memory, options: { color: C.lightGrey, fontSize: 10.5, italic: true } }
], {
x: 0.55, y: 4.52, w: 9.0, h: 0.82,
fontFace: "Calibri", valign: "middle", wrap: true, margin: 0
});
}
// ─── BUILD DECK ─────────────────────────────────────────
addCoverSlide(pres);
cards.forEach(card => {
addQuestionSlide(pres, card);
addAnswerSlide(pres, card);
});
// End slide
const end = pres.addSlide();
end.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: C.darkBg }
});
end.addShape(pres.ShapeType.rect, {
x: 0, y: 0, w: 10, h: 0.08,
fill: { color: C.accent }
});
end.addShape(pres.ShapeType.rect, {
x: 0, y: 5.545, w: 10, h: 0.08,
fill: { color: C.accent }
});
end.addText("30", {
x: 2.5, y: 1.0, w: 5, h: 1.2,
fontSize: 90, bold: true, color: C.accent,
align: "center", fontFace: "Calibri", margin: 0
});
end.addText("MCQs COMPLETE", {
x: 1, y: 2.2, w: 8, h: 0.7,
fontSize: 26, bold: true, color: C.white,
align: "center", charSpacing: 6, fontFace: "Calibri", margin: 0
});
end.addShape(pres.ShapeType.rect, {
x: 2.5, y: 3.05, w: 5, h: 0.04,
fill: { color: "3A5570" }
});
end.addText("Revise again in 24h • Attempt weak topics again • Best of luck for NEET PG 2026!", {
x: 0.5, y: 3.18, w: 9, h: 0.55,
fontSize: 11, color: C.lightGrey,
align: "center", fontFace: "Calibri", margin: 0
});
end.addText("Orris Medical Mentor | Lens Flashcard Deck | Ophthalmology", {
x: 1, y: 5.05, w: 8, h: 0.35,
fontSize: 9, color: "4A6580",
align: "center", fontFace: "Calibri", margin: 0
});
pres.writeFile({ fileName: "/home/daytona/workspace/lens-flashcards/Lens_MCQ_Flashcards_NEET_PG_2026.pptx" })
.then(() => console.log("SUCCESS: Flashcard deck created!"))
.catch(err => { console.error("ERROR:", err); process.exit(1); });
cd /home/daytona/workspace/lens-flashcards && node build.js 2>&1
ls -lh /home/daytona/workspace/lens-flashcards/
Lens MCQ Flashcards NEET PG 2026
Presentation · PPTX
What's Inside (61 Slides)
30 MCQs Covering All PYQ Topics:
| # | Topic | What's Tested |
|---|---|---|
| 1-2 | Embryology | Lens origin (surface ectoderm), adult nutrition (avascular/aqueous) |
| 3-4 | Anatomy/Histology | Thinnest capsule (posterior pole), epithelium location (anterior only) |
| 5-6 | Physiology | Presbyopia mechanism, diabetic myopic shift (sorbitol/aldose reductase) |
| 7-8 | Age-related Cataract | PSC worst with miosis, "Second sight of aged" (nuclear sclerosis) |
| 9-10 | Cataract Maturity | Iris shadow test, Morgagnian cataract (sinking nucleus) |
| 11-13 | Systemic Associations | Alport syndrome, Wilson's sunflower, Diabetic snowflake cataract |
| 14-15 | Drug-induced | Steroid → PSC, Chlorpromazine → anterior star |
| 16-17 | Traumatic | Vossius ring, True exfoliation (glassblower) |
| 18 | Pseudoexfoliation | Dandruff on lens + Sampaolesi line + open-angle glaucoma |
| 19-20 | Lens Dislocation | Marfan (superotemporal), Homocystinuria (inferonasal + thrombosis trap!) |
| 21-22 | Congenital Cataract | Surgery timing (amblyopia urgency), Galactosemia reversibility |
| 23-24 | Lens-Induced Glaucoma | Phacomorphic (closed angle), Phacolytic (open angle) |
| 25-26 | Cataract Surgery | PCO/after-cataract (Nd:YAG), Aphakic spectacles ring scotoma |
| 27 | Microspherophakia | Weill-Marchesani + pupil block (miotics contraindicated!) |
| 28 | Fabry Disease | Propeller/spoke lens opacity + cornea verticillata |
| 29-30 | Congenital Anomalies | PFV/PHPV (unilateral + microphthalmia), Lens coloboma (inferonasal) |
Now teach me uveitis and glaucoma based on pyt for neet pg 2026
👁️ UVEITIS + GLAUCOMA — NEET PG 2026
PYQ-Oriented Master Session | Your Mentor's Lecture
📊 EXAM WEIGHT
| Topic | Questions/Exam | Style |
|---|---|---|
| Glaucoma | 2-3 questions | Clinical scenario, visual field image, instrument-based |
| Uveitis | 1-2 questions | Association-based, clinical scenario |
PART A: UVEITIS
MODULE U1: ANATOMY - WHAT IS THE UVEA?
- Iris (anterior) → inflammation = Iritis/Anterior uveitis
- Ciliary body (middle) → inflammation = Cyclitis
- Choroid (posterior) → inflammation = Choroiditis
MODULE U2: CLASSIFICATION (The PYQ Framework)
By Anatomical Location:
| Type | Site | Common Causes |
|---|---|---|
| Anterior uveitis | Iris / Ciliary body | HLA-B27 diseases, JIA, HSV, sarcoidosis |
| Intermediate uveitis (Pars planitis) | Vitreous / Pars plana | MS, sarcoidosis, Lyme disease |
| Posterior uveitis | Choroid / Retina | Toxoplasmosis, CMV, TB, syphilis |
| Panuveitis | Entire uvea | Sarcoidosis, VKH, Behcet, Sympathetic ophthalmia |
By Onset:
- Acute: Sudden, painful, photophobic, red eye (<3 months)
- Chronic: Insidious, painless, minimal injection (>3 months)
- Recurrent: Episodes with quiescent periods
MODULE U3: ANTERIOR UVEITIS - THE HIGHEST YIELD
Clinical Features (PYQ-Tested Signs):
| Sign | Description | Significance |
|---|---|---|
| Ciliary flush | Perilimbal injection (circumcorneal) | Differentiates uveitis from conjunctivitis |
| Keratic precipitates (KPs) | Inflammatory cells on corneal endothelium | Type tells the diagnosis (see below) |
| Flare | Protein in AC on slit lamp (Tyndall effect) | Blood-aqueous barrier breakdown |
| Cells | WBCs in AC on slit lamp | Active inflammation grade |
| Hypopyon | Pus layer in AC (gravity) | Severe anterior uveitis / Behcet |
| Posterior synechiae | Iris adheres to anterior lens capsule | Complication → pupil irregularity, iris bombe |
| Iris bombe | Iris balloons forward (aqueous trapped) | → Angle closure → Secondary glaucoma |
| Band keratopathy | Calcium deposits in Bowman layer | Chronic uveitis (especially JIA) |
| Miosis | Small pupil | Iris sphincter irritation / posterior synechiae |
KP Types - THE Critical PYQ Association:
| KP Type | Description | Condition |
|---|---|---|
| Mutton-fat KPs | Large, greasy, coarse deposits | Granulomatous uveitis (Sarcoid, TB, VKH, Sympathetic ophthalmia) |
| Fine stellate KPs | Small, spread over entire endothelium | Fuchs Heterochromic Iridocyclitis (FHIC) |
| Fine non-granulomatous KPs | Small, inferior triangle (Arlt's triangle) | Non-granulomatous (HLA-B27, viral) |
PYQ: "Mutton-fat KPs are seen in?" → Granulomatous uveitis (sarcoid, TB, VKH) PYQ: "Stellate KPs involving entire corneal endothelium?" → Fuchs heterochromic iridocyclitis
MODULE U4: KEY UVEITIS ASSOCIATIONS (Most Tested)
HLA-B27 Associated Uveitis - THE MOST COMMON CAUSE OVERALL
- Ankylosing spondylitis (AS) → ~40% develop AAU in lifetime
- Reactive arthritis (Reiter syndrome)
- Psoriatic arthritis
- Inflammatory bowel disease (Crohn's, UC) → Mnemonic: "ARPI"
- Acute, Anterior, Unilateral (classic)
- Recurrent alternating (one eye then the other) = very characteristic
- Fibrinous exudate, hypopyon
- Non-granulomatous (fine KPs)
- 50% of AAU cases are HLA-B27 positive
PYQ: "Bilateral recurrent alternating anterior uveitis is characteristic of?" → HLA-B27 uveitis
JIA Uveitis - The Silent Blinder
- JIA (pauciarticular, young girls, ANA positive)
- Chronic, PAINLESS, BILATERAL anterior uveitis - no red eye, no symptoms!
- Child presents with COMPLICATIONS (band keratopathy, cataract, glaucoma)
- Screened with routine slit lamp exams
- Associated: ANA positive, RF negative
PYQ: "Painless, asymptomatic anterior uveitis in a child is characteristic of?" → JIA (pauciarticular)
Sympathetic Ophthalmia - High-Yield Classic
- Penetrating injury → exposes sequestered retinal antigens (melanin, S-antigen) to immune system
- Sensitized T lymphocytes attack BOTH eyes
- Injured eye = exciting eye
- Fellow (uninijured) eye = sympathizing eye
- Exciting eye injured first
- Sympathizing eye develops granulomatous panuveitis
- Can occur 2 weeks to many years after injury (most common 4-8 weeks)
- Mutton-fat KPs (granulomatous)
- Dalen-Fuchs nodules = pathognomonic nodules between RPE and Bruch's membrane
- Can blind the famous: blinded Louis Braille
- Enucleation of the injured eye WITHIN 2 WEEKS (before sensitization) can prevent sympathetic ophthalmia
- Once SO has developed: systemic immunosuppressives (steroids)
PYQ: "Sympathetic ophthalmia after penetrating injury - what is pathognomonic finding?" → Dalen-Fuchs nodules PYQ: "To prevent sympathetic ophthalmia, injured eye should be enucleated within?" → 2 weeks
Vogt-Koyanagi-Harada (VKH) Disease - Image-Based
- Bilateral granulomatous panuveitis + systemic features
- Systemic features: Vitiligo, poliosis (white hair), alopecia, meningismus, tinnitus, dysacusis
- Sunset glow fundus (depigmented choroid) - classic fundus image
- Dalen-Fuchs nodules may be seen (similar to sympathetic ophthalmia)
- Exudative retinal detachment
- ANA positive (sometimes)
PYQ: "Sunset glow fundus is seen in?" → VKH disease
Behcet Disease - The Triple Syndrome
- Young adults (20-40 yrs), Middle Eastern/Asian
- Classic triad: Oral aphthous ulcers + Genital ulcers + Uveitis (ocular)
- Ocular: Acute simultaneous BILATERAL anterior uveitis with HYPOPYON (shifting hypopyon)
- Retinal vasculitis (both arteries and veins) with hemorrhages
- Pathergy test positive (exaggerated skin reaction to needle prick)
- HLA-B51 associated
PYQ: "Shifting hypopyon with oral and genital ulcers?" → Behcet disease
Fuchs Heterochromic Iridocyclitis (FHIC) - The Tricky One
- Unilateral, chronic, painless, minimal injection
- Heterochromia - lighter affected eye (iris stromal atrophy)
- Fine stellate KPs distributed over entire corneal endothelium (NOT Arlt's triangle)
- NO posterior synechiae (unique among uveitis - this is a PYQ trap!)
- Complications: Cataract + Glaucoma (common) but no CME
- Fine vessels crossing TM on gonioscopy → anterior chamber bleeding during surgery
- Topical steroids DO NOT help (another unique feature)
PYQ: "Uveitis with NO posterior synechiae and stellate KPs over entire endothelium?" → FHIC
Sarcoid Uveitis
- Most common in African-Americans and Scandinavians
- Bilateral granulomatous uveitis (mutton-fat KPs)
- Iris Busacca nodules (in iris stroma) and Koeppe nodules (at pupil margin)
- Snowball opacities in vitreous (posterior) = classic
- Candle-wax drippings on retinal vessels (retinal periphlebitis)
- ACE levels elevated (serum)
- Chest X-ray: Bilateral hilar lymphadenopathy
- Conjunctival biopsy can confirm diagnosis
PYQ: "Busacca and Koeppe nodules on the iris are seen in?" → Sarcoidosis PYQ: "Candle-wax drippings on fundus?" → Sarcoid periphlebitis
Posterior Uveitis Causes - Quick Table
| Cause | Key Feature |
|---|---|
| Toxoplasmosis | Most common cause of posterior uveitis worldwide; "Headlight in fog" appearance (active white lesion next to old scar); cat exposure |
| CMV retinitis | AIDS patients (CD4 <50); "Pizza-pie/ketchup & cheese" appearance; treated with valganciclovir |
| TB | "Sticky" uveitis; extensive posterior synechiae; bilateral; PPD/IGRA positive |
| Syphilis | Placoid chorioretinitis (virtually pathognomonic); can affect any ocular structure |
| Candida | Immunocompromised; "String of pearls" vitritis; fluconazole |
Uveitis Complications (PYQ Table):
| Complication | Mechanism |
|---|---|
| Band keratopathy | Chronic uveitis → calcium deposits in Bowman membrane (especially JIA) |
| Posterior synechiae | Iris adherent to lens → irregular pupil, seclusio pupillae |
| Seclusio pupillae | 360° posterior synechiae → pupil completely stuck → aqueous trapped → iris bombe |
| Iris bombe | Forward bowing of iris → acute angle closure glaucoma |
| Complicated cataract | PSC → "posterior subcapsular cataract" |
| Hypotony | Ciliary body shutdown → low IOP → phthisis bulbi |
| Secondary glaucoma | Trabecular meshwork blocked by cells/synechiae |
MODULE U5: TREATMENT OF UVEITIS - PYQ Essentials
- Topical steroids + cycloplegics (atropine/cyclopentolate - prevents synechiae, relieves pain)
- Cycloplegic = dilates pupil + paralyzes ciliary muscle → breaks posterior synechiae
- Systemic steroids ONLY after ruling out/treating active TB
- Anti-TB drugs if TB uveitis
- Topical steroids + Methotrexate (DMARDs) for systemic JIA
- Systemic high-dose steroids → Immunosuppressives
PART B: GLAUCOMA
MODULE G1: WHAT IS GLAUCOMA?
- Optic disc changes (cupping)
- Visual field defects (peripheral first, central last)
- IOP elevation (usually, but not always)
MODULE G2: IOP MEASUREMENT - INSTRUMENTS PYQ
Goldmann Applanation Tonometry (GAT) - GOLD STANDARD
- Measures force needed to flatten a 3.06 mm diameter corneal area
- Uses fluorescein stained tear film; viewed with cobalt blue light
- Two green semicircular mires align when correct pressure applied
- Dial reading × 10 = IOP in mmHg
| Factor | Effect on IOP reading |
|---|---|
| Thick cornea (>520 μm) | Overestimates IOP |
| Thin cornea (<520 μm) | Underestimates IOP |
| Post-LASIK/refractive surgery | Underestimates (cornea thin + altered structure) |
| Excessive fluorescein (thick mires) | Overestimates |
| Corneal edema | Underestimates |
PYQ: "Normal CCT assumed by Goldmann tonometry?" → 520 μm PYQ: "Post-LASIK IOP measurement?" → Underestimates (both thinner and structurally altered)
Other Tonometers:
- Schiotz (indentation) - non-contact, portable, less accurate
- Perkins - portable Goldman (bedside use)
- Non-contact (air-puff) - screening only
- Tonopen - portable electronic
MODULE G3: PRIMARY OPEN ANGLE GLAUCOMA (POAG)
The MOST COMMON type of glaucoma worldwide
- Asymptomatic for years (insidious) - diagnosed late
- IOP elevated (usually >21), but may be normal (NTG variant)
- Open angle on gonioscopy
- Progressive optic disc cupping
- Visual field defects (peripheral → central)
- Bilateral (but may be asymmetric)
- Age (>40)
- Family history
- High IOP
- Black race
- High myopia
- Thin CCT
Optic Disc Changes in Glaucoma (PYQ):
| Feature | Description |
|---|---|
| Cup:Disc ratio (CDR) | Normal <0.5; Glaucomatous >0.6-0.7 |
| CDR asymmetry | >0.2 between eyes is significant |
| Bayonetting of vessels | Vessels kink at disc margin |
| Nasal displacement of vessels | Vessels shift nasally |
| Inferior notch | ISNT rule violated (Inferior > Superior > Nasal > Temporal rim width) |
| Disc hemorrhage | Splinter hemorrhage at disc margin → prognostic sign |
| Laminar dot sign | Pores of lamina cribrosa visible (deep cupping) |
| Peripapillary atrophy | Alpha and beta zones around disc |
Visual Field Defects in Glaucoma (PYQ Image-Based):
| Defect | Stage |
|---|---|
| Enlarged blind spot | Earliest |
| Bjerrum scotoma (arcuate) | Early - arises from blind spot, curves around fixation |
| Ronne nasal step | Early - defect respects horizontal midline nasally |
| Ring scotoma | Advanced - Bjerrum scotoma above + below fuse |
| Tubular (gun-barrel) vision | Very late - only central island remains |
| Central + Temporal island | End-stage before total blindness |
PYQ: "Earliest visual field defect in glaucoma?" → Enlarged blind spot (or Bjerrum scotoma — depends on source) PYQ: "Visual field defect respecting horizontal midline nasally?" → Ronne's nasal step
MODULE G4: PRIMARY ANGLE CLOSURE GLAUCOMA (PACG)
Acute PACG - THE EMERGENCY
| Feature | Detail |
|---|---|
| Pain | Severe, excruciating, may radiate to head |
| Nausea/Vomiting | Vagal response to high IOP |
| Colored halos | Around lights (corneal edema causing light diffraction) |
| Vision | Suddenly blurred/reduced |
| Cornea | Steamy, edematous, hazy |
| Pupil | Fixed, mid-dilated, oval (6-8 mm) |
| Anterior chamber | Shallow |
| IOP | >40 mmHg (often 60-80!) |
| Circumcorneal injection | Ciliary congestion |
- Dark room (pupil dilates)
- Emotional stress
- Mydriatic drops
- Anticholinergic drugs (atropine, tricyclics, antihistamines)
- Reading (prolonged near work)
- Hypermetropia (small eye, shallow AC)
- Female > Male (3:1)
- Asian > Caucasian
- Age (lens grows with age → shallower AC)
| Step | Drug/Procedure | Mechanism |
|---|---|---|
| 1. Lower IOP medically | IV Acetazolamide 500mg + Oral glycerol (osmotic) | Reduce aqueous production |
| 2. Miotic | Pilocarpine 2-4% every 15 min × 2-3 doses | Pulls iris away from angle |
| 3. Beta-blocker | Timolol 0.5% topical | Reduce aqueous production |
| 4. Definitive | Nd:YAG laser peripheral iridotomy (PI) | Creates hole in iris → relieves pupil block |
| Fellow eye | Prophylactic laser PI | High risk of fellow eye attack |
PYQ: "First-line definitive treatment of angle closure glaucoma?" → Laser peripheral iridotomy PYQ: "Drug contraindicated in angle closure glaucoma?" → Anticholinergics (atropine), mydriatics
MODULE G5: GLAUCOMA DRUGS (PYQ Pharmacology)
| Drug Class | Drugs | Mechanism | IOP Reduction | Key Side Effect |
|---|---|---|---|---|
| Beta-blockers | Timolol, Betaxolol | ↓ Aqueous production | 20-25% | Betaxolol = cardioselective (safer in asthma); Timolol → bradycardia, bronchospasm |
| Prostaglandin analogs | Latanoprost, Bimatoprost | ↑ Uveoscleral outflow | 30-35% (MOST effective) | Iris pigmentation, eyelash growth (hypertrichosis), periorbital fat atrophy |
| Alpha-2 agonists | Brimonidine | ↓ Aqueous production + ↑ outflow | 20-25% | Drowsiness, allergic conjunctivitis; avoid in infants (apnea) |
| Carbonic anhydrase inhibitors | Dorzolamide (topical), Acetazolamide (oral) | ↓ Aqueous production | 15-20% | Acetazolamide → metabolic acidosis, renal stones, Steven Johnson syndrome; avoid in sulfa allergy |
| Miotics (cholinergics) | Pilocarpine | ↑ Trabecular outflow (TM pulled open by ciliary muscle) | 20-25% | Miosis, brow-ache, induced myopia |
- Oral: 500mg loading, then 250mg QID
- IV: 500mg for acute attack
- Mechanism: inhibits carbonic anhydrase in ciliary body → ↓ aqueous secretion
- Contraindicated in: Sulfa allergy, severe renal failure, hepatic failure
PYQ: "Most effective class of anti-glaucoma drug in terms of IOP reduction?" → Prostaglandin analogs (~30-35%) PYQ: "Anti-glaucoma drug causing eyelash growth and iris pigmentation?" → Latanoprost/Bimatoprost (prostaglandin) PYQ: "Drug used in acute angle closure glaucoma (oral/IV)?" → Acetazolamide
MODULE G6: SPECIAL TYPES OF GLAUCOMA (PYQ Favorites)
Normal Tension Glaucoma (NTG)
- IOP always ≤21 mmHg but glaucomatous disc + field changes
- Vascular insufficiency to optic nerve (rather than just pressure)
- Associated: Vasospasm, migraine, sleep apnea, low diastolic BP
- CCT tends to be thinner (GAT underestimates true IOP)
Pigmentary Glaucoma
- Young myopic males
- Krukenberg spindle (vertical pigment on corneal endothelium)
- Iris transillumination defects (slit-like, mid-peripheral) - melanin lost from posterior iris
- Deep anterior chamber
- Exercise/dilation → acute IOP spikes (pigment showers)
Pseudoexfoliative Glaucoma
- Open angle; hardest to control IOP
- White dandruff-like material on lens capsule + TM
- Sampaolesi line on gonioscopy
- Asymmetric, elderly
Sturge-Weber Syndrome → Glaucoma
- Port-wine stain (facial haemangioma in V1/V2 distribution)
- Ipsilateral glaucoma in ~30%
- Episcleral hemangioma → elevated episcleral venous pressure → glaucoma
- Buphthalmos if onset <2 years
- Brain: Leptomeningeal angioma → seizures, intellectual disability
- Tram-track calcification on CT
PYQ: "Glaucoma + port wine stain on face?" → Sturge-Weber syndrome PYQ: "Mechanism of glaucoma in Sturge-Weber?" → ↑ Episcleral venous pressure + trabeculodysgenesis
Buphthalmos (Congenital Glaucoma / Ox Eye)
- Onset <3 years; IOP elevation causes globe to enlarge (cornea/sclera still pliable)
- Features: Enlarged globe, Haab's striae (breaks in Descemet's membrane), Epiphora, Blepharospasm, Photophobia (classical triad of symptoms)
- Corneal diameter >12 mm (normal = 10 mm at birth)
- Treatment: Trabeculotomy + Trabeculectomy (surgical; NOT medical first-line)
PYQ: "Symptoms triad of congenital glaucoma?" → Epiphora + Blepharospasm + Photophobia PYQ: "Haab's striae are seen in?" → Congenital glaucoma / Buphthalmos
MODULE G7: SURGICAL TREATMENT
| Procedure | Indication | Notes |
|---|---|---|
| Laser PI (YAG/Argon) | Angle closure, prophylaxis | Definitive for pupil block |
| Selective Laser Trabeculoplasty (SLT) | POAG | Opens TM |
| Trabeculectomy | POAG/CACG when drugs fail | Creates filtration bleb; MMC used to prevent scarring |
| Trabeculotomy | Congenital glaucoma | Opens TM from inside |
| Ahmed/Baerveldt valve | Refractory glaucoma | Drainage tube implant |
| Cyclodestructive procedures | End-stage | Diode laser cycloablation |
📋 RAPID FIRE PYQ RECALL
UVEITIS:
Mutton-fat KPs → Granulomatous (TB, Sarcoid, VKH, Sympathetic ophthalmia)
Stellate KPs (entire endothelium) → Fuchs HIC
Fine KPs in Arlt's triangle → Non-granulomatous (HLA-B27)
HLA-B27 uveitis → Acute, unilateral, recurrent alternating
Bilateral recurrent alternating AAU → HLA-B27
Painless bilateral uveitis in child → JIA (pauciarticular, ANA+)
Band keratopathy in child → JIA uveitis
Shifting hypopyon + oral/genital ulcers → Behcet
Sunset glow fundus → VKH
Dalen-Fuchs nodules → Sympathetic ophthalmia / VKH
Blinded Louis Braille → Sympathetic ophthalmia
Enucleation within 2 weeks → prevents Sympathetic ophthalmia
No posterior synechiae in uveitis → Fuchs HIC
Busacca + Koeppe nodules → Sarcoidosis
Candle-wax drippings → Sarcoid periphlebitis
"Headlight in fog" → Toxoplasmosis (posterior uveitis)
CMV retinitis + AIDS → CD4 <50; pizza-pie appearance
GLAUCOMA:
GAT CCT assumption → 520 μm
Thin cornea → underestimates IOP
Post-LASIK → underestimates IOP
Most common glaucoma worldwide → POAG
Earliest field defect → Enlarged blind spot
Bjerrum scotoma → arcuate, around fixation
Nasal step → Ronne's
ISNT rule → Inferior > Superior > Nasal > Temporal (glaucoma violates)
Acute angle closure → Fixed mid-dilated oval pupil + severe pain + colored halos
Definitive treatment PACG → Laser peripheral iridotomy
Most effective IOP-lowering drug → Prostaglandin analogs
Eyelash growth + iris pigmentation → Latanoprost
Betaxolol = cardioselective beta-blocker (safe in asthma)
Acetazolamide contraindicated → Sulfa allergy
Krukenberg spindle + mid-peripheral TIDs → Pigmentary glaucoma
Port-wine stain + glaucoma → Sturge-Weber
Epiphora + blepharospasm + photophobia → Congenital glaucoma
Haab's striae → Congenital glaucoma
Surgery for congenital glaucoma → Trabeculotomy
Normal IOP + optic disc cupping + field defects → Normal tension glaucoma
Pilocarpine contraindicated → Weill-Marchesani (microspherophakia)