Jones fracture
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Jones fracture" fifth metatarsal treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I now have comprehensive information from multiple authoritative sources. Here is a full clinical overview.
Jones Fracture
Definition & Historical Note
The Jones fracture is a fracture at the metaphyseal-diaphyseal junction of the proximal fifth metatarsal (Zone II), specifically extending into the fourth-fifth intermetatarsal articulation. It was originally described by Sir Robert Jones in 1896, though his description actually appears to reference a diaphyseal fracture rather than the avulsion fracture of the base - a source of historical confusion that persists in naming conventions today.
Anatomy & Zone Classification (Lawrence & Botte / Botte Classification)
The fifth metatarsal base is divided into three fracture zones:
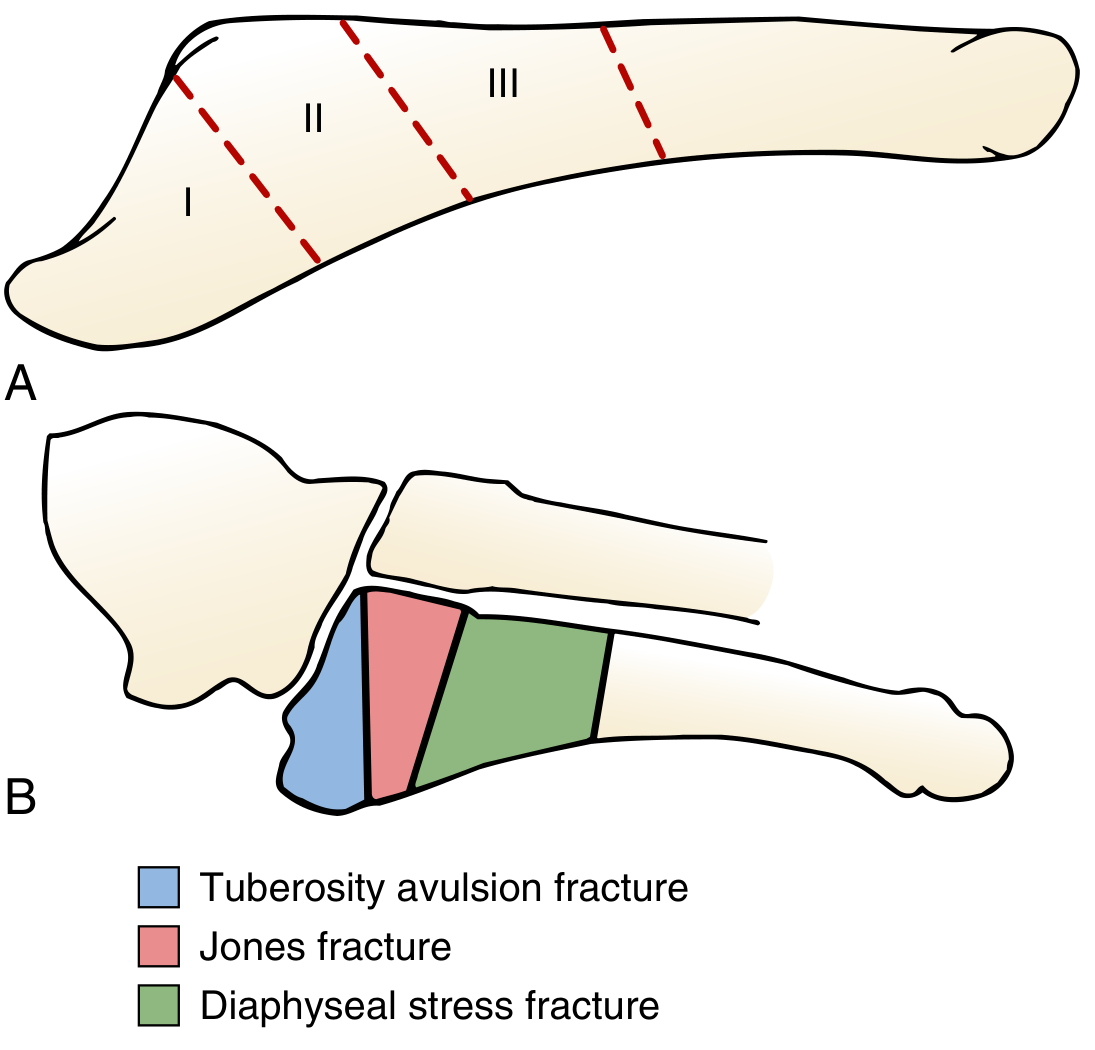
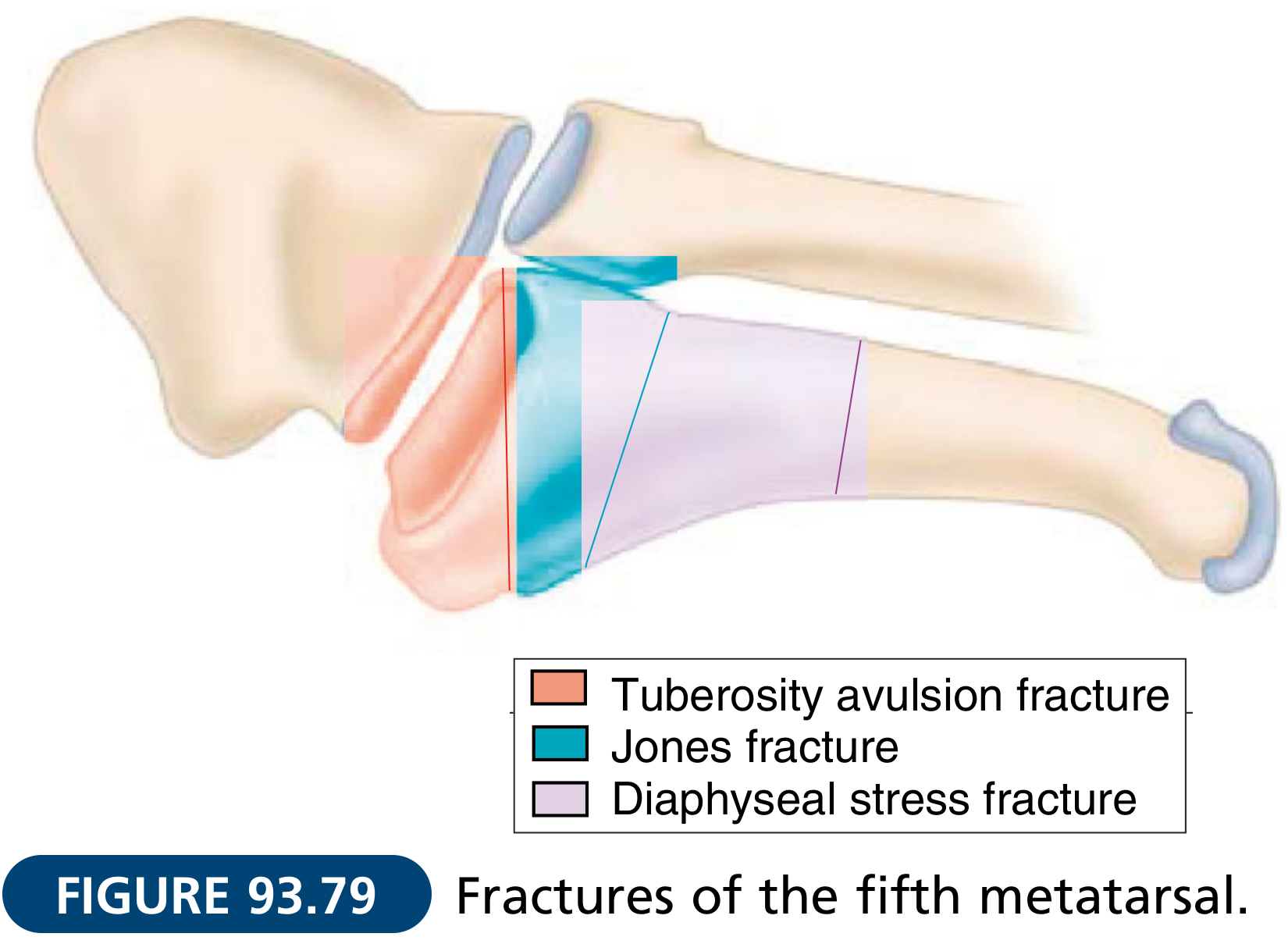
| Zone | Location | Fracture Type | Mechanism |
|---|---|---|---|
| I (Tuberosity) | Most proximal, metatarsocuboid articulation; proximal to 4th-5th metatarsal articulation | Avulsion fracture ("Pseudo-Jones") | Inversion injury; peroneus brevis/plantar fascia avulsion |
| II | Metaphyseal-diaphyseal junction including 4th-5th metatarsal articulation | True Jones fracture | Strong abduction force to forefoot - bending moment at metaphyseal-diaphyseal junction |
| III | Proximal 1.5 cm of diaphysis | Stress fracture | Repetitive microtrauma (athletes) |
Radiograph - Jones Fracture

(Arrow indicates the fracture at the metaphyseal-diaphyseal junction)
Why Jones Fractures Are Prone to Nonunion
The Zone II area lies in a vascular watershed region - the blood supply is relatively poor compared to more proximal or distal zones. This is the primary reason these fractures have a well-known tendency toward delayed union and nonunion.
Risk factors for fracture/nonunion include:
- Long, narrow, straight fifth metatarsal with an adducted forefoot
- Metatarsus adductus with a curved fifth metatarsal and prominent base
- Cavus foot deformity (mechanical disadvantage for healing)
- Hypovitaminosis D
Diagnosis
- Plain radiographs are usually adequate (AP, oblique, lateral foot views)
- CT scan is considered for more detailed assessment in high-performance athletes
- Must be distinguished from Zone I avulsion fracture (pseudo-Jones) and Zone III stress fracture - the distinction drives management
Torg Classification (for Zone III stress fractures)
| Type | Radiographic Finding |
|---|---|
| I (Acute) | No periosteal reaction, no widening, no sclerosis |
| II (Delayed union) | Periosteal reaction, fracture site widening, some intramedullary sclerosis |
| III (Nonunion) | Intramedullary sclerosis, blunted fracture edges |
Treatment
Zone I (Pseudo-Jones / Tuberosity Avulsion)
- Walking boot, cast boot, or post-op shoe based on symptom level
- Weight bearing as tolerated
- Average healing: ~44 days (range up to 65 days)
- Nonunions rarely painful; if so, can excise the fragment
- ORIF only for displaced intraarticular fractures in young, highly active individuals
Zone II (True Jones Fracture)
Non-operative (non-athletes/non-competitive):
- Non-weight-bearing short leg cast for 6-8 weeks
- 15-25% risk of nonunion with conservative management
- Recent data shows CAM boot with weight bearing as tolerated may achieve equivalent union to surgical treatment
- Up to 25% of patients treated non-operatively ultimately require surgical intervention; one study showed a 44% failure rate with cast alone
Operative (athletes and competitive individuals):
- Intramedullary screw fixation is the preferred technique
- Minimum screw diameter: 4.5 mm (not recommended to go smaller); mean is ~5 mm; use the largest screw to fill the canal to minimize refracture risk
- The AP radiograph determines screw diameter; lateral radiograph determines screw length
- Return to full activity before radiographic union is a predictor of operative failure
- Failure/refracture rates after surgery: 0-40% (most series <5%); nearly all athletes return to sport
Indications for surgery:
- Acute fractures in competitive or elite athletes
- Zone II/III fractures not healing clinically at 8-12 weeks
- Patients whose occupational demands do not permit prolonged non-weight-bearing
- Recurrent fracture after prior non-operative treatment
- Metatarsus adductus or cavus foot (consider operative given mechanical disadvantage)
For nonunion/refracture: Intramedullary screw fixation + consider cancellous bone graft or bone marrow aspirate at the fracture site
Zone III (Diaphyseal Stress Fracture)
- Mostly in athletes (repetitive microtrauma)
- Treatment follows the same principles as Zone II
- One study suggests no distinction needs to be made between Zone II and Zone III in terms of management and outcomes
Key Pitfalls
- Do not confuse Zone I (pseudo-Jones, avulsion) with the true Zone II Jones fracture - they have very different management and prognosis
- In children aged 10-13, a painful secondary ossification center on oblique view = Iselin disease, not a fracture
- Active adolescents with shaft Jones fractures: fixation is increasingly favored to allow faster return to activities and prevent refracture
Recent Evidence
A 2026 systematic review and meta-analysis (Lowe et al., PMID 42031019) examined screw characteristics and intramedullary fixation outcomes for Jones fractures, consistent with the current recommendation to use larger-diameter screws.
Sources: Campbell's Operative Orthopaedics 15th Ed. 2026, pp. 5210-5211 | Miller's Review of Orthopaedics 9th Ed., p. 606 | Tintinalli's Emergency Medicine, p. 1916
SICK SCAPULA SYNDROME
Finding Sources
Finding Sources
Searching PubMed
"SICK scapula" syndrome scapular dyskinesis
Reading File
Reading File
Finding Sources
Searching PubMed
scapular dyskinesis overhead athlete treatment
Finding Sources
Finding Sources
Finding Sources
Searching the Web
SICK scapula syndrome clinical features assessment treatment rehabilitation
Reading Web Page
https://musculoskeletalkey.com/examination-and-management-of…
Finding Sources
I now have comprehensive information from multiple authoritative sources. Here is the full clinical overview:
SICK Scapula Syndrome
The Acronym
SICK is a mnemonic coined by W. Ben Kibler describing a cluster of findings in overhead athletes with scapular overuse/fatigue dysfunction:
| Letter | Meaning |
|---|---|
| S | Scapular malposition (drooped/protracted scapula on the affected side) |
| I | Inferior medial border prominence (winging) |
| C | Coracoid pain and malposition |
| K | Dyskinesis of scapular movement |
Definition & Context
SICK scapula syndrome is a specific overuse muscle fatigue syndrome seen predominantly in overhead and throwing athletes (baseball pitchers, swimmers, tennis players, volleyball players). It represents a pattern of scapular dyskinesis - an alteration of the normal position or motion of the scapula during coupled scapulohumeral movements - arising from repetitive overuse and cumulative muscle fatigue of the scapular stabilizers.
Scapular dyskinesis itself may be:
- An underlying cause of shoulder pain and dysfunction, OR
- An accompanying result of existing shoulder pathology
The distinction is important: not all scapular dyskinesis is SICK scapula syndrome, and not all SICK scapula is necessarily pathological in isolation - context (symptoms, sport demands, associated injuries) determines clinical significance.
Pathomechanics
Normal Scapular Function
The scapula serves as the dynamic platform linking the axial skeleton to the upper limb. Its normal roles include:
- Positioning the glenoid for optimal glenohumeral joint reaction force (compressive, not shear)
- Providing a stable base for rotator cuff force generation
- Elevating and rotating to maintain subacromial clearance during arm elevation
- Acting as a force transfer link in the kinetic chain
The scapular stabilizers work in coordinated balance:
- Upward rotation / protraction: Serratus anterior, upper trapezius
- Retraction / external rotation / posterior tilt: Middle and lower trapezius, rhomboids
- Elevation: Upper trapezius, levator scapulae
- Resistance to medial rotation: Rhomboids, levator scapulae
How SICK Scapula Develops
With repetitive overhead use, progressive muscle fatigue and imbalance develop in the scapular stabilizers. The typical pattern is:
- Pectoralis minor tightness - pulls the coracoid process anteroinferiorly, causing:
- Anterior tilt of the scapula
- Internal rotation of the scapula
- Inferior displacement ("drooped" scapula)
- Serratus anterior weakness/fatigue - impairs upward rotation, allowing medial border to "wing"
- Lower trapezius inhibition - reduces posterior tilt and external rotation
This results in a scapula that is inferiorly positioned, protracted, anteriorly tilted, and unable to upwardly rotate adequately - the combined picture of SICK scapula.
Consequences of the malalignment:
- Decreased subacromial space (protracted scapula narrows the subacromial outlet) - contributes to impingement
- Coracoid pain from pectoralis minor tension and mechanical loading
- Reduced rotator cuff efficiency (suboptimal glenoid orientation)
- Increased risk of SLAP tears, labral pathology, and AC joint injury
Clinical Presentation
Population: Predominantly competitive overhead/throwing athletes; can occur in any patient with repetitive shoulder use.
Symptoms:
- Shoulder pain (often anterior - coracoid region, subcoracoid impingement)
- Subacromial/superior shoulder pain with overhead activity
- Generalized aching around the periscapular musculature
- Sense of shoulder fatigue, "heaviness," or instability
- Often bilateral but asymmetric
Key clinical signs on inspection:
- The involved scapula appears "dropped" / inferiorly displaced compared to the contralateral side
- Inferior medial border prominence (winging)
- Coracoid process is prominent and tender to palpation
- Visible asymmetry of scapular resting position
Clinical Assessment
Static Linear Measurements (with arms at side)
Three measurements to quantify asymmetry:
- Infera - vertical height difference of the superomedial angle of the inferior scapula between sides (cm)
- Lateral displacement - horizontal distance of the superomedial scapular angle from midline, compared between sides (cm)
- Abduction - angular difference of the medial scapular border from a midsagittal plumb line between sides (degrees)
Scapular Retraction Test (SRT) - Key Diagnostic Maneuver
A positive SRT strongly supports SICK scapula as a contributing diagnosis:
- Perform Jobe's "empty can" test (shoulder 90° abduction in scapular plane, maximal internal rotation, resisted elevation) - record pain (0-10) and strength
- Manually reposition the scapula into retraction and posterior tilt (correct the dyskinesis)
- Repeat the empty can test
- Positive SRT = ≥2-point decrease in pain OR significant increase in strength with scapular correction - implies scapular malalignment is contributing to symptoms
Dynamic Assessment
Visual observation of scapular motion during:
- Arm elevation (look for premature elevation, asymmetric rhythm, winging)
- Lowering phase (eccentric control - often where dyskinesis is most apparent)
- Throwing or sport-specific movements
Associated Conditions
SICK scapula frequently co-exists with or contributes to:
- Subacromial impingement syndrome
- SLAP tears (superior labrum anterior-posterior)
- Rotator cuff pathology (tendinopathy, partial tears)
- Glenohumeral internal rotation deficit (GIRD)
- AC joint pathology - notably, type III AC dislocations are associated with scapular dyskinesis and SICK scapula
- Shoulder instability (anterior)
- Biceps tendinopathy (coracoid/subcoracoid impingement on the biceps tendon)
Management
Management is predominantly non-operative and rehabilitation-based.
Phase 1 - Addressing Flexibility Deficits
- Pectoralis minor stretching (cornerstone - releases the primary driver of scapular anterior tilt/protraction)
- Posterior capsule stretching (for associated GIRD)
- Thoracic spine mobility work (thoracic kyphosis contributes to scapular protraction)
Phase 2 - Scapular Stabilizer Strengthening
Targets the inhibited/weakened muscles:
- Lower trapezius activation (prone Y-raises, prone rows with external rotation)
- Serratus anterior strengthening (wall push-ups with plus, serratus punches, bear crawl variations)
- Middle trapezius (prone T-raises, seated rows)
- Rhomboids with caution - over-strengthening rhomboids without lower trap/serratus balance can worsen anterior tilt
Phase 3 - Rotator Cuff & Kinetic Chain Integration
- Rotator cuff strengthening in the newly corrected scapular position
- Kinetic chain exercises (hip, core, lumbopelvic) to restore proximal power transfer
- Sport-specific movement re-patterning (throwing mechanics, stroke mechanics, etc.)
Scapular Retraction Taping / Bracing
- Can provide short-term symptom relief and proprioceptive re-education
- Helps athletes "feel" the correct scapular position during early rehab
Biofeedback
- Visual biofeedback has shown immediate benefit for altering scapular muscle activation and motion
- Long-term transferability to functional tasks remains under investigation
Operative Treatment
- Surgery is rarely indicated for SICK scapula itself
- Indicated for specific underlying pathology not responding to conservative care (e.g., SLAP repair, labral reconstruction, AC joint surgery)
- Arthroscopic pectoralis minor release has been described for refractory cases where pectoralis minor tightness is the dominant driver
- Following AC joint surgery: structured rehab addressing SICK scapula improves outcomes - one study showed 18/23 patients with type III AC dislocation and scapular dyskinesis had resolved dyskinesis at 12 months after rehabilitation
Key Points Summary
- SICK = Scapular malposition, Inferior medial border prominence, Coracoid pain & malposition, dysKinesis
- Predominantly an overuse fatigue syndrome in overhead/throwing athletes
- Core mechanism: pectoralis minor tightness + serratus anterior / lower trapezius weakness
- The "dropped scapula" on the affected side is the hallmark clinical sign
- Scapular Retraction Test (SRT) is the key clinical test
- Management is primarily rehabilitation - pec minor stretching + scapular stabilizer strengthening
- Coexists with many other shoulder conditions (SLAP, impingement, instability) - address the whole picture
Sources: Campbell's Operative Orthopaedics 15th Ed. 2026, p. 2892 | Imaging Anatomy Vol. 3, Bones, Joints, Vessels and Nerves, p. 88 | Kibler WB et al. (Musculoskeletal Key) | Physiotutors Clinical Review
This is a shared conversation. Sign in to Orris to start your own chat.